
Abstract
HIV drug resistance testing is fundamental in clinical patient management, but data on HIV-1 drug-resistant mutations (DRMs) is scarce in the Caribbean and in Suriname limited to one survey on transmitted resistance. The aim of this study was to address this gap, to gain insight in acquired HIV drug resistance (ADR) prevalence and mutation patterns, and to improve HIV-1 treatment outcome of people living with HIV (PLHIV) in Suriname. A prospective cross-sectional study was conducted from July 2018 through January 2019 among treatment-experienced PLHIV (n = 72), with either treatment failure or antiretroviral therapy restart. Genotypic drug resistance testing was performed and DRM impact on drug effectiveness was examined. Genotypic drug resistance testing revealed 97.2% HIV-1 subtype B, 2.8% B/D recombinants and a ADR prevalence of 63.2% in treatment failure patients, with a predominance of nonnucleoside reverse transcriptase inhibitor (NNRTI) mutations. The most common DRMs were M184V (23.6%) and K103N (18.8%). A high level of non-DRM polymorphisms was observed in both the reverse transcriptase (RT) and protease (PR) gene. Interesting deviations from the existing mutation datasets were noted at position E248 and R83 of the RT gene and L63 and V77 in the PR gene. Full susceptibility to all examined drugs was 54.2%, while high-level drug resistance was estimated at 37.5%, which seems promising for treatment outcomes for PLHIV in Suriname, although cross-resistance to next-generation NNRTIs was already estimated for nearly a quarter of the patients. The meager 2.9% of PR DRMs rendered protease inhibitors as an effective rescue HIV-1 treatment.
Introduction
The number of people living with HIV (PLHIV) in 2019, amounted to 38.0 million worldwide 1 and in the absence of an effective vaccine to control the HIV spread, the reduction of HIV-1-related mortality, disease progression, and transmission relies heavily on the use of antiretroviral therapy (ART). The global scale-up of highly active ART has revolutionized the HIV pandemic in the last two decades, with a spectacular reduction in HIV-1 mortality, mother-to-child transmission, adult HIV-1 incidence, and an improved quality of life of PLHIV. The number of people having access to ART reached 25.4 million in 2019 compared to just 7.8 million in 2010 and the annual number of new HIV infections in 2019 was 1.7 million, a 19.0% drop since 2010. 1 However, selective pressure from massive use of ART has led to the emergence of HIV drug-resistant mutations (DRMs), causing a decreased drug susceptibility in virus variants, thus compromising treatment success. Initial World Health Organization (WHO) guidelines for first-line ART regimens, consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) and one nonnucleoside reverse transcriptase inhibitor (NNRTI) were updated in 2016 with the replacement of thymidine analogs by tenofovir (TDF), alongside a cytidine analog. For the NNRTI backbone regimen, nevirapine (NVP) was phased out from first-line regimens, and efavirenz (EFV) was recommended. Accumulation of scientific evidence resulted in the recommendation in 2018 for preferential use of integrase strand transfer inhibitors (INSTI), dolutegravir and raltegravir.
Antiretroviral (ARV) treatment failure is especially high in patients using early regimens with NRTI/NNRTI combinations and overall drug resistance among patients with HIV-1 subtype B, ranged from 16.4% in treatment-naive persons in Croatia 2 to more than 80% in treatment-experienced patients in Brazil. 3 HIV drug resistance testing is not only crucial in clinical patient management but also in gathering scientific data to guide policy decisions regarding national treatment regimens. Nevertheless, financial constraints have impeded most low- and middle-income countries (LMIC) in implementing routine HIV genotyping, despite the fact that LMIC have adult HIV prevalence rates ranging from 1.2% to 7.5%.
The Caribbean region is the second most affected region of HIV in the world, next to Africa.
Suriname is often considered as a Caribbean country, due to political ties with the region and cultural similarities, which is also mirrored in the HIV prevalence rate (1.3%). 4 Limited use of ART started around 1996 in Suriname and 23.4% of PLHIV had free access to ART in 2010. This percentage doubled to 49.5% in 2018 and the mortality declined with 28.6%, between 2010 and 2017. 4 Against the backdrop of these achievements, AIDS is still among the top 10 causes of death, and data on HIV DRMs in Suriname are limited to the results from one study conducted in 2009 among treatment-naive adults. 5 Moreover, most LMIC, especially in the Caribbean are battling with paucity of data on acquired HIV DRMs.
To address this gap and to gain insight in acquired HIV drug resistance (ADR) prevalence and mutation patterns, a cross-sectional study was conducted among treatment-experienced PLHIV in Suriname. Genotypic drug resistance testing was performed for all PLHIV, visiting a hospital in the capital in the period from July 2018 through January 2019, either with treatment failure or restarting ART. The type and frequency of DRMs and their predicted impact on drug effectiveness were examined, thus improving clinical patient management.
Methods
Study setting
Suriname is a small country located along the northeastern coast of South America, with a multiethnic population of ∼580,000, mostly living in and around the capital Paramaribo. Suriname is classified as upper-middle-income country, but is battling a recession and provision of health services are especially difficult in the scarcely populated and hard to reach interior. Nevertheless, HIV testing, counseling, and treatment are widely available and free of charge within the decentralized HIV care model. However, specialized HIV care is only available in the main hospitals in Paramaribo. HIV prevalence was 1.3% for the age group 15–49 years in 2018, 1,4 while higher prevalence rates were noted for key populations. In 2005, the country adopted a zidovudine (AZT), lamivudine (3TC), and NVP-based drug combination as preferred first-line regimen.
Study population
A prospective cross-sectional study was conducted from July 2018 through January 2019, including all consenting treatment-experienced PLHIV visiting the main hospitals in Paramaribo, with either treatment failure or ART restart after treatment interruption. Treatment failure (clinical or virological) was defined according to WHO guidelines. 6 Patients restarting ART after treatment interruption were considered as treatment-experienced, because of prior ART use for more than 6 months. Treatment interruption was defined as an episode of at least 30 days of ART interruption. No age or sex restrictions were applied, but patients with a viral load below 1,000 copies/mL were excluded.
Peripheral whole-blood samples were collected from all enrolled PLHIV for HIV-1 genotyping, and a physician-administered questionnaire was used to collect demographic data, including age, sex, and ethnicity alongside reason for genotyping and HIV-1 history. Anonymized data were entered in an electronic database by double-entry.
RNA extraction, PCR's, and DNA sequencing
Viral RNA was isolated from 560 μL plasma with the QIAamp Viral RNA kit (QIAGEN, Inc., Valencia, CA). PCR amplification of the pol gene covering the HIV-1 protease (PR) gene (codons 1–99) and the N-terminal region of the reverse transcriptase (RT) gene (codons 1–300) was performed utilizing in-house master-nested RT-PCR protocols from WHO. 7 Sequencing reactions were conducted with the BigDyeTM v3.1 Cycle Sequencing Kit (Applied BiosystemsTM, Foster City, CA), after PCR product cleanup with ExoSAP-ITTM Express PCR Product Cleanup Reagent (Affymetrix, Inc., Santa Clara, CA). Sequencing products were purified with the BigDye XterminatorTM Purification Kit (Applied Biosystems) and subsequently sequenced on an ABI 3500XL genetic analyzer (Applied Biosystems).
Data analysis
The Stanford HIV Drug Resistance Database v8.7 (
Data were analyzed using Tableau version 2019.2.2. Age analysis was performed for the age groups <35 years (n = 27) and ≥35 years (n = 45).
The chi-square test and the Fisher's exact test were used for associations between groups. The Student's t-test was used for comparisons of overall mutation frequency between individuals with and without DRMs. A p value <.05 was considered statistically significant.
Ethics statement
After obtaining informed consent, clinicians shared patient demographics and HIV-1 history with the principal investigator, adhering to all precautions to safeguard patient confidentiality, including data anonymization. HIV-1 genotyping was incorporated in clinical management and the testing was according to the national Ethics Committee not subject to additional consent requirements.
Results
A total of 72 treatment-experienced PLHIV were enrolled. Genotypic drug resistance testing for the RT gene was successfully performed for all 72 samples, while the success rate for PR was 94.4% (68/72), due to inadequate PCR amplification. Due to a RT-PR amplification overlap, the absent PR sequences also resulted in missing, respectively, 89, 104, 106, and 108 starting amino acids from the RT sequences for these four patients.
Subtype determination revealed 97.2% HIV-1 subtype B and 2.8% B/D recombinants. The male-to-female ratio was 1.1 and the median age was 36, ranging from 15 to 73 years. Data on ethnicity were incomplete, but based on available data (n = 50), the majority of patients were of African descent (68.0%).
Treatment records were provided by the hospitals for 66 patients and NRTI-based treatment had been registered for all these patients, while 83.3% and 72.7% had also used NNRTIs and protease inhibitors (PIs), respectively. Experience with ARVs from all three classes (NNRTI, NRTI, and PI), was recorded for 50.0% of the patients, and INSTI was also used by 15.2% of this category.
Throughout patient treatment histories, highest use was recorded for the NRTIs 3TC (81.8%); AZT (77.3%), and TDF (77.3%), while NVP (74.2%) and EFV (36.4%) were the most common NNRTIs.
All PIs were ritonavir-boosted, with lopinavir/r (LPV/r, 51.5%) and atazanavir/r (ATV/r, 28.8%) as main PI-based drugs.
Although INSTIs were not included in the national regimen, INSTI use was registered for 10.6% of the patients, most likely brought along from neighboring French Guiana.
A total of 34 different ARV combinations were recorded with predominant use of the regimen consisting of AZT, 3TC, and NVP, in line with the national treatment guidelines.
Drug resistance mutations
ARV-resistant viruses were revealed in 45.8% of the patients, with a predominant occurrence of NNRTI-associated DRMs. An overview of the observed frequency of DRMs is represented in Table 1. As expected, the ADR prevalence was significantly higher in patients with treatment failure (63.2%) than in patients restarting ART, where DRMs were less common (24.2%).
Drug Resistance Mutations Within Different Drug Classes
Protease mutations were determined for 68 sequences.
The test reason was not recorded for one patient.
For differences in DRM frequency between patients with treatment failure and patients restarting ART.
χ 2 test.
Fisher's exact.
DRM, drug-resistant mutation; ART, antiretroviral therapy; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
DRM differences between these categories did not reach significance for particular ARV classes (Table 1).
An even distribution was observed for single class (22.3%) and double class DRMs (22.2%), while triple class DRMs were restricted to patients with treatment failure (2.6%).
Resistance associated with PI mutations was rare (2.9%) and could only be demonstrated in combination with DRMs from another class.
The overall prevalence of the major NRTI, NNRTI, and PI-associated DRMs is presented in Table 2. Amino acid mixtures, mostly consisting of a wild-type/mutant combination, were commonly observed at major DRM positions and no deletions or insertions were detected.
Prevalence of Drug-Resistant Mutations
Overall prevalence of major drug RT resistance mutations observed in the study population determined for, respectively, 72 sequences or a68 sequences.
69 sequences.
70 sequences.
PR resistance mutations were determined for 68 sequences.
TAM, thymidine analog mutation; RT, reverse transcriptase; PR, protease.
The predominant NRTI-associated resistance mutation was M184V and the most common thymidine analog mutations (TAMs) included T215FY and D67N. The K65R mutation, which is linked to resistance to TDF, was detected in two participants, one with a TDF history and one with a missing treatment record.
TAMs were only present in patients with a drug history with thymidine analogs.
Neither the multidrug resistance mutations, MDR151 and MDR69, nor the accessory TAMs, E40F or E44A, were observed within our study population.
The most prevalent NNRTI-associated mutation was K103N, while K103S was observed once. The second and third most frequent NNRTI-associated mutations were G190A (6.9%) and Y181C (5.6%), respectively.
The occurrence of the leading DRMs M184V and K103N was further elevated in the category of patients with treatment failure to 34.2% (13/38) and 27.8% (10/36), respectively.
Only two major PI-associated DRMs were observed (I54V and V82A), both present in the same protease sequence, together with the accessory mutations L10F and Q58E. In addition, another single protease sequence carried K20T as an accessory mutation.
The male-to-female ratio was similar between the resistant and the nonresistant population (1.2 vs. 1.1; p = .782).
Overall development of resistance between the age groups <35 years (median age 27) and ≥35 years (median age 44) was not significantly different (p = .760).
Analysis of the number of regimen switches versus presence of DRMs did not show a positive association, although it should be noted that patient history information was generally limited, thus also precluding analysis of the relationship between DRM prevalence and time elapsed since first ARV use.
Other mutations
Investigation of polymorphisms, not classified as DRM (other mutations) in the RT gene demonstrated a considerable sequence diversity as illustrated in the overall mutation profile in Figure 1. The mean observed mutation frequency of non-DRMs at all amino acid positions was 4.6% for RT and 7.4% for PR. A multitude of nucleotide substitutions was demonstrated, resulting in amino acid changes at 45.3% of the examined amino acid positions (1–300). The most common mutated site in the RT gene was I293, with I293V detected in 79.1% of all participants. Especially notable are RT positions 200, 207, 211, 272, and 293, where the majority of the observed variation could be attributed to a single mutation, while on the other hand E297, displayed extensive diversity, resulting in nine different amino acids.

Cumulative mutation frequency in the RT gene. Amino acid positions 1–100, 101–200 and 201–300 in the RT gene are displayed along the X-axis in the panels
No significant difference was observed between viruses with and without major DRMs in their overall mutation frequency of other mutations (p = .207).
Despite the low DRM frequency for the PR gene, a considerable genetic diversity was displayed in the protease sequence (Fig. 2).
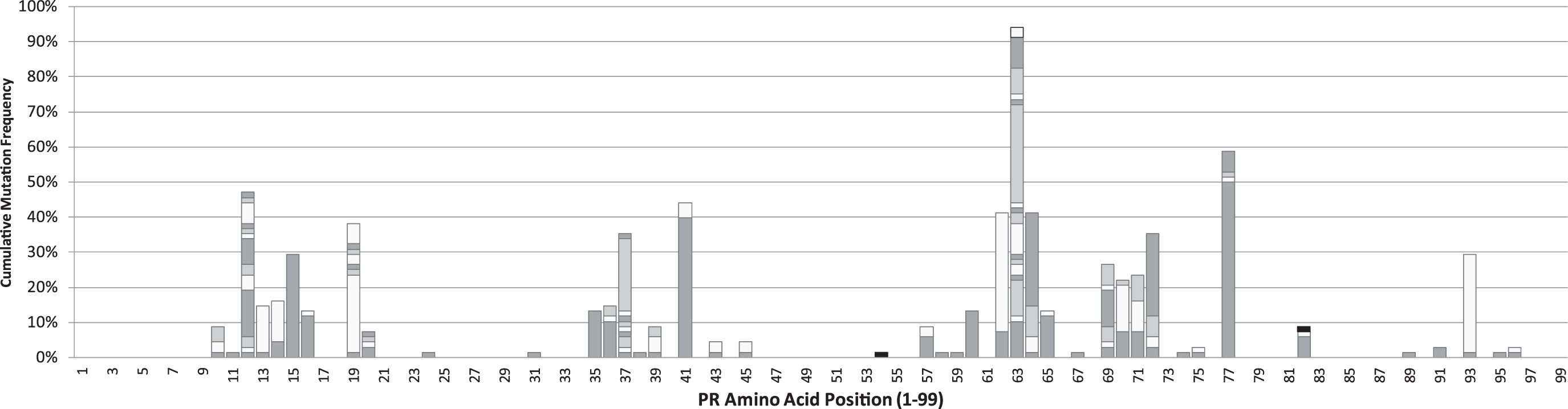
Cumulative mutation frequency in the PR gene. Amino acid positions in the full PR gene (1–99) are displayed along the X-axis. Bars represent cumulative mutation frequencies at each amino acid position. Each block in a bar, irrespective of the gray shade, represents different mutations and areas in black represent DRMs. The mutation frequency is determined for 68 sequences. PR, protease.
Mutations were observed at 42.4% of the examined amino acid positions, with V77I as most common mutation. Noteworthy is the extreme variation at position L63, not only reaching 94.1% conversion with respect to the wild-type virus but also displaying an assortment of 17 different amino acid combinations, characterizing L63 as hotspot in our cohort.
Impact DRM on drug effectiveness
Fully susceptible profiles were observed in 54.2% of the patients and even in 36.8% of the treatment failure cohort. The predicted effectiveness of three ARV classes in Suriname based on the impact of observed DRMs in the patient cohort is illustrated in Figure 3.
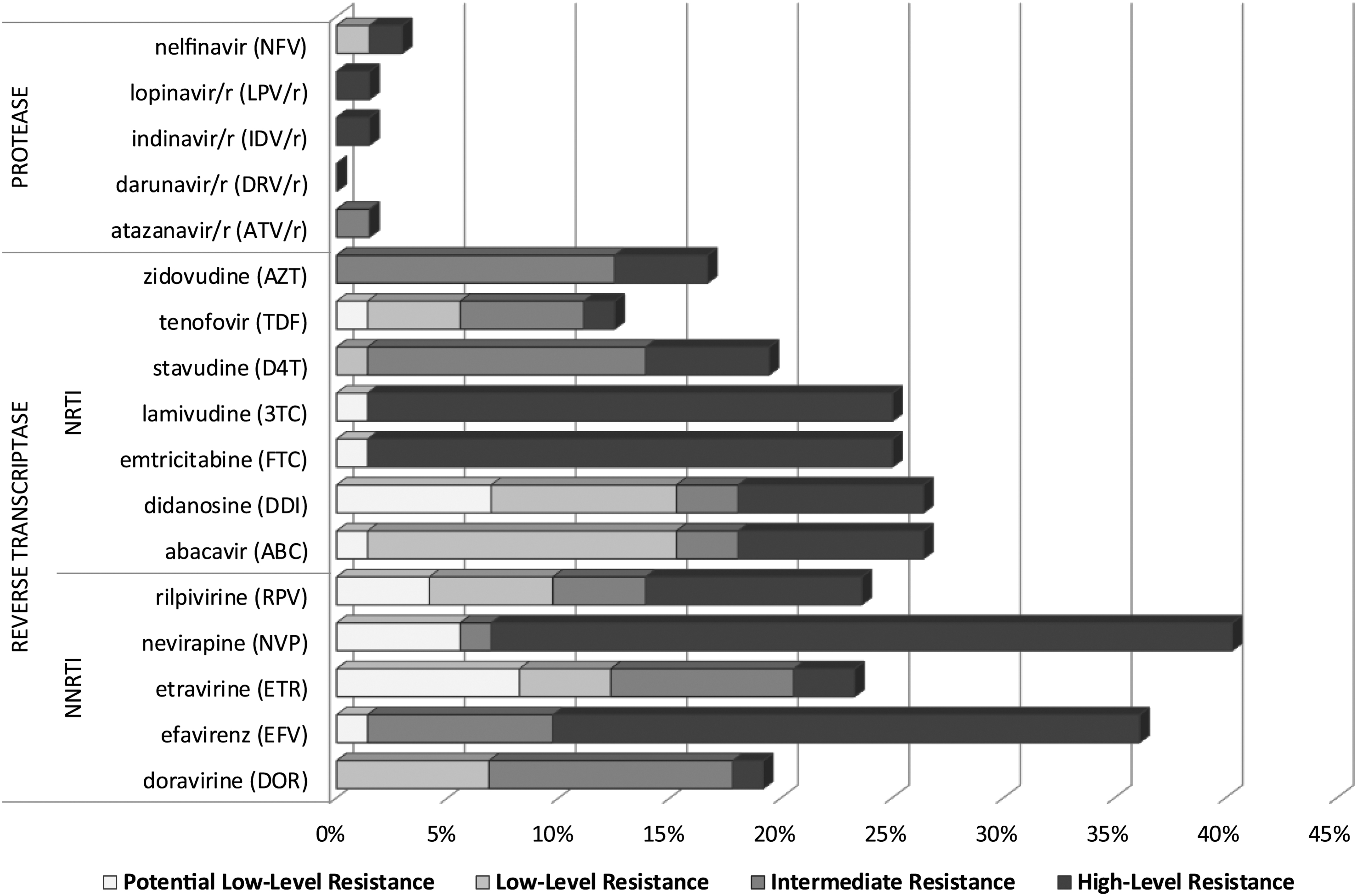
Predicted effectiveness of ARV drugs per drug class. Drug resistance predictions are based on the impact of DRMs in the study population (n = 72). The expected cumulative resistance for each ARV is depicted as a horizontal bar and the different shades in each bar represent different levels of resistance. “Potential low-level resistance” is considered as “susceptible,” but is depicted to provide overall insight. NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; ARV, antiretroviral.
NNRTIs were the most compromised ARVs, although the majority of patients (58.3%) were still deemed susceptible to EFV, NVP, doravirine (DOR), etravirine (ETR), and rilpivirine (RPV).
The highest frequency of high-level drug resistance was projected for NVP (33.3%) and EFV (26.4%), while nearly one-quarter of the patients did not even retain full susceptibility to second-generation NNRTIs as ETR and RPV.
NRTIs are also becoming less useful, since 26.4% of patients harbored DRMs causing some level of resistance. Noteworthy is that both abacavir and didanosine were compromised for all these patients. Caution is also warranted for 3TC and emtricitabine (FTC), because of the high occurrence of M184V, which is known to confer high-level in vitro resistance to these drugs.
Almost all patients (97.1%) remained fully susceptible to the class of PIs.
Discussion
This study presented the first HIV-1 drug resistance patterns in treatment-experienced PLHIV in Suriname. Subtype determination based on both PR and RT genomic regions revealed 97.2% subtype B and 2.8% B/D recombinants, which is similar to the 5.1% presence of B/D recombinants, observed in an earlier study in Suriname among treatment-naive PLHIV. 5 Although predominant presence of subtype B in Suriname was in accordance with the Mesoamerican region, non-B subtypes and recombinants have been frequently observed in treatment-naive populations in the Caribbean. 10
ADR prevalence in this setting was 45.8% and even reached 63.2% in the treatment failure cohort. Caution is warranted that this reflects the upper limit of the national ADR prevalence, as enrollment was restricted to treatment-experienced PLHIV, visiting the hospital either with treatment failure or restarting ART.
Scarcity of DRM data from Caribbean countries precluded comparative analysis within the Caribbean, but the estimated ADR prevalence in Suriname was lower than in neighboring Brazil, with a drug resistance level above 80% among treatment-experienced patients 3 and in other similar patient cohorts in Asia 11 and Europe 12 reporting 75.5% and 77.9%, respectively.
However, national and global estimates of DRM rate for HIV are highly variable, driven by several factors as number and type of available ARV regimens, access to ART, period of availability of ARV in the country, patient compliance, and suboptimal clinical drug resistance monitoring.
The significantly lower DRM frequency in patients restarting ART was consistent with the view that a lack of drug-selective pressure allows reemerging of the wild-type virus. 13 An uneven distribution for resistance prevalence by drug class was demonstrated in the treatment failure cohort with 55.3% NNRTI DRM versus 36.8% NRTI DRM. The higher NNRTI mutation rate, despite the slightly higher current use of NRTIs in our setting, was probably incited by the early availability of NNRTIs on the global market and the reported low genetic barrier of first-generation NNRTIs toward drug resistance.
Predominance of NNRTI DRMs has also been reported in studies from Chile 14 and China, 15 although others have observed similar DRM rates 11,16 or even prevailing NRTI resistance. 17
The premise that younger age (<35 years) seemed to be associated with the development of resistance 11 could not be substantiated within our patient cohort.
Likewise, our results did not corroborate the observation that NNRTI DRMs are nearly twice as high among women in comparison with men 18 as NNRTI resistance in women in our study was even lower than in men. However, similar results were registered for Brazil and Colombia, 18 although these studies were conducted among treatment-naive populations. More detailed records on duration of treatment, number and type of regimens and actual level of adherence are required to adjust for confounding factors in the investigation of this phenomenon.
Despite a relatively short country history of ARV use, the majority of listed DRMs for RT were detected within our cohort. The poor compliance as reported by clinicians and the use of 34 different ARV combinations within the clinical cohort may be at the basis of this outcome.
The absence of the K70E, M230L, and Y188L mutations was not surprising, as K70E is regarded as an uncommon nonpolymorphic mutation and ETR and DOR, which have been linked to the M230L and Y188L mutation, respectively, had not been prescribed to the study population.
The absence of multidrug-resistant mutation Q151M was in line with near zero prevalence reports from Europe, 19 but in contrast with prevalence rates ranging from 2.1% to 11.3% in LMIC. 20,21
The finding of M184V as leading NRTI mutation was in line with international data, although our observed prevalence (23.6%) was lower than reported in Panama 22 and northern Brazil, 17 with prevalence rates of 76.0% and 80.1%, respectively.
Tenofovir's signature K65R mutation was only detected in 2.9% of participants, despite the common use of TDF. However, subtype C has been suggested as strong risk factor for K65R development 23 and low occurrence of K65R in our subtype B setting was concurrent with low prevalence rates in other studies among HIV subtype B patients.
K103N, Y181C, and G190A were the most prevalent NNRTI mutations, consistent with earlier observations, 24 most likely due to their limited effect on viral fitness.
Notwithstanding our high use of PIs (72.7%), PI resistance seemed restricted to just 2.9% of all patients, concurrent with other reports from Panama 22 and China. 15 However, high PI-DRM rates have been reported, even up to 32.5% in Western Europe. 25 The high genetic barrier of PI toward resistance and exclusive use of ritonavir-boosted PIs in our cohort may partially account for the observed high preservation of susceptibility to PI. Possible underestimation of PI resistance should not be ruled out, as some PI mutations may be located outside the screened pol gene. 26
The occurrence of other mutations, currently not classified as DRM, provided some insight in these usually overlooked polymorphisms. A high level of polymorphism was observed in both the RT and PR gene in this cohort. The premise that higher overall mutation frequencies could serve as indicator for increased risk of treatment failure could not be corroborated.
As foreseen, the mutation frequencies in our treatment-experienced setting were generally higher than naturally occurring polymorphisms as reported earlier in Suriname 5 and in the Stanford Database for treatment-naive persons. Surprisingly, especially in light of the relatively brief history of ARV use, the same trend of elevated mutation frequencies was observed in the comparison with the Stanford datasets covering treatment-experienced persons, with exceptions only at position R83 (1.5% vs. 15%), I135 (39.4% vs. 48.1%), and A272 (50.7% vs. 59.7%) in the RT gene.
Interestingly, the observed allelic variation at these positions was even lower than the mutation level registered for naive patients in the Stanford database. Further research with more detailed patient and treatment histories is required to comprehend the relevance of this finding. The two most common naturally occurring RT-variants at I293 and R211 were also leading in our cohort, whereas outliers displaying the highest divergences from the Stanford datasets for treated persons were observed at positions E248 and R83. In Suriname, the mutation level at position E248 was almost fourfold higher, while the occurrence of natural variants at this position was similar to international results. On the contrary, the mutation rate at the R83 position was remarkably demoted in our treated cohort, accentuating the earlier observed lack of mutations at this position among treatment-naive participants in Suriname. 5
The dynamic interplay between host, environment, geographical region, therapeutic selections, and patient adherence could have coerced the rate of genomic virus evolution resulting in the noted deviations from the existing mutation datasets.
Polymorphisms in the PR gene were quite analogous to data for natural variants, in line with the extremely low DRM frequency in our cohort. The highest-ranking protease mutation at position L63 was characterized as distinct mutation hotspot with an assortment of allelic variants in nearly all participants (94.1%), consistent with the leading position in the Stanford database, although the prevalence and allelic variation were markedly amplified in our cohort. The conformity with the aforementioned database did not extend to our second common mutation V77I, which displayed a higher mutation frequency than aforementioned datasets, but analogous to results from Puerto Rico. 27 The high occurrence of V77I in Suriname was unsettling, as evidence exists linking this polymorphism to resistance to Nelfinavir. 28
The first insight on DRMs in treatment-experienced patients in Suriname revealed a limited high-level drug resistance predicted for any ARV (37.5%) and even 54.2% of fully susceptible isolates, which seems promising for clinical management in Suriname. However, these numbers are actually less favorable, since 36.8% of patients with treatment failure harbored the wild-type virus, thus indicating that adherence was an issue. Clinical management in Suriname should therefore also implement measures to improve patient discipline toward treatment adherence and continue to endorse routine viral load testing, which may have aided in circumvention of drug resistance accumulation.
Use of NNRTIs induces cross-resistance, which was indeed observed in our patient cohort. Next-generation NNRTIs as RPV, DOR, and ETR were scarcely or not used, but cross-resistance was estimated for 19.4%, 19.4%, and 15.3% of the participants, respectively, which negatively impacts their use in future regimen choices.
High-level NRTI resistance was most frequently observed for the still recommended FTC and 3TC, due to the high occurrence of M184V. However, this mutation positively impacts the use of AZT, stavudine, and TDF because of reduced viral fitness and increased virus sensitivity to these drugs, but combined presence with the L74V mutation annuls the positive effect. The finding of this combination in one patient cautioned for close monitoring of the development of the L74V mutation in Suriname, which would limit future salvage regimen choices, especially important for TDF as the least compromised NRTI and the recommended NRTI backbone drug as replacement for thymidine analogs. Also, reassuring was the absence of other TDF-associated mutations, such as K70E and T69 insertions.
The low observed DRM frequency for PIs rendered almost all examined viruses susceptible to PIs.
The study had some limitations, centered on incomplete patient data, which precluded analysis of interesting correlations of DRM prevalence versus time since first ARV use and versus demographic characteristics like ethnicity.
The poor adherence of patients did not allow for reliable determination of the duration of virologic failure for each patient with each particular treatment, thus challenging the evaluation of the clinical impact of the various ARV combinations. Some caution is warranted in the data interpretation, as results may have been impacted by conventional PCR pitfalls such as substandard RNA quality, reduced primer binding in case of genetic variability at the primer binding site and PCR introduced errors, in addition to the difficulties to detect low-level presence of variant sequences or viral quasispecies.
Nevertheless, the results enabled assessment of current regimens and can serve as baseline to allow monitoring of trends of HIV-1 drug resistance, thus strengthening the national HIV program, although prospective studies should ensure more detailed patient histories and broaden the study population. Furthermore, these results can guide national treatment policies and future treatment regimens containing at least one PI could be an effective option to rescue HIV treatment for almost every patient, underscoring the importance of utilization of local data.
Conclusion
The first assessment of HIV-1 DRMs in treatment-experienced PLHIV in Suriname demonstrated a relatively low HIV ADR prevalence of 45.8%, although almost all major DRMs for RT were detected within our cohort. Predominance of NNRTI DRMs was demonstrated, despite the slightly higher current use of NRTIs in the study setting, consistent with international data.
Likewise, the finding of M184V and K103N, Y181C, and G190A as leading NRTI and NNRTI mutations was in line with international data, but the presented DRM patterns are a valuable addition to the scarce international data on HIV-1 DRMs in LMIC.
A high level of non-DRM allelic variation was observed in both the RT and PR gene, but higher overall mutation frequencies did not indicate an increased risk of treatment failure.
Interesting deviations from the existing mutation datasets were noted at position E248 and R83 of the RT gene and L63 and V77 in the PR gene.
The DRM assessment revealed 54.2% of preservation of full susceptibility to all examined drugs and 37.5% of high-level drug resistance to any ARV, which seems promising for clinical management and treatment outcomes for PLHIV in Suriname, although cross-resistance to next-generation NNRTIs was already estimated for nearly a quarter of the patients. The meager 2.9% of PI DRMs rendered PIs as an effective option to rescue HIV treatment for almost every patient.
Footnotes
Author Contributions
M.R.A. conceived of the study. M.R.A., R.S., M.Y.L.-B., and M.G.G. contributed to the study design and analyzed the data. R.S., M.Y.L.-B., and M.G.G. performed the laboratory work. Drafting and reviewing of the article was carried out by M.R.A., R.S., M.Y.L.B., and M.G.G.
Acknowledgments
We express our gratitude to the participating clinicians. We gratefully acknowledge D. Stijnberg for statistical support and J. Faerber, R. Rakhan, S. Pancham, and M. Oron for laboratory assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study; genotypic drug resistance testing for all eligible patients was part of national Human Immunodeficiency Virus-testing, financed by the Ministry of Health through the Global Fund Human Immunodeficiency Virus/Tuberculosis grant #SUR-C-MOH 17/43.