
Abstract
To evaluate the efficacy, safety, and tolerability of switching to a dolutegravir (DTG)-based regimen in a cohort of virological suppressed HIV-infected patients who have previously been treated with different antiretroviral combination. The dynamics of total HIV-DNA and levels of high-sensitivity c-reactive protein, interleukin-6, soluble-CD14, and D-Dimer were also analyzed. Ninety-six individuals who switched to a DTG-containing regimen were followed up for 48 weeks. HIV RNA, CD4+ T cell count, weight, and levels of laboratory parameters were recorded at baseline, after 24 and 48 weeks of treatment for all study participants. In a subgroup of patients, HIV DNA and inflammation/coagulation marker levels were also analyzed until week 24. Ninety-three out of 96 patients maintained virological suppression, including patients who switched to dual-therapy from triple-drug combination. Eighteen out of 96 patients had residual viremia at baseline, of which 13 reached the maximal viral suppression at W48. Serum creatinine levels showed a significant increase at weeks 24 and 48. A progressive reduction of total cholesterol was observed from week 24 and up to week 48. No variation in body mass index was detected. HIV DNA, inflammation, and coagulation marker levels did not significantly change during follow-up. Switching to a DTG-based regimen may be a key option for achieving and maintaining maximal virological suppression, even in patients showing residual viremia at baseline. Furthermore, the improvement in blood lipid profile and the overall tolerability observed in this study strongly support the use of these regimens in the aging HIV population.
Introduction
The introduction of combined antiretroviral therapy (cART) has had a powerful impact on HIV transmission and disease progression, but it is not curative and lifetime treatment remains needed to prevent virus reactivation from latently infected cells. 1,2 Despite the effectiveness of cART in promoting recovery of CD4+ T cell counts and control of viral replication, long-term exposure to drugs may contribute to the onset of non-AIDS-related complications, for which chronic immune activation and inflammation are known to play a decisive role. 3,4
In recent years, monitoring studies have reported many evidence and assumptions about adverse events related to prolonged ART assumption, including renal, liver, and cardiovascular dysfunctions. 5 –8
Consequently, the development of new compounds and antiretroviral combinations has become critically important for patients who had treatment failure and to consider switching strategies for those who achieved stable virological suppression (defined as plasma viral load <50 copies/mL) and require a therapeutic optimization. In the latter population, according to current antiretroviral guidelines, regimen switching to reduce pill burden or dosing frequency, to improve adherence and tolerability, to reduce toxicity and costs, and to prevent drug–drug interaction is indicated. 9,10 The physicians' goal is to reach one or more of these benefits in their patients while maintaining HIV RNA levels below the detection limit.
The integrase strand transfer inhibitors (INSTI) are widely used in clinical practice for their highly specific action to viruses and low toxicity. 11 Among these, dolutegravir (DTG) has shown, from the beginning, high antiviral activity and excellent safety profile. Moreover, it is characterized by favorable pharmacokinetic properties, few drug–drug interactions, and a high genetic barrier to resistance development compared with first-generation INSTI. 12,13
Data from clinical trials performed on a cART-experienced population showed the immunological and virological efficacy of DTG-based regimen both as salvage therapy in individuals with documented drug resistance 14,15 and as dose simplification option (DTG coformulated with abacavir and lamivudine, once daily) in virologically suppressed adults. 16 Even more, a case report has documented the virological efficacy of DTG despite the presence of archived INSTI mutations. 17
To minimize drug exposure and related toxicity, DTG has been investigated as a part of dual regimen in combination with rilpivirine in a phase 3 trial involving virologically suppressed patients on a stable cART, showing noninferiority to conventional three- or four-drug regimen. 18 Moreover, results from clinical trials and observational studies support the therapeutic potential of the combination DTG plus lamivudine, as maintenance strategy in virologically suppressed patients. 19 –22
On the contrary, there are conflicting data regarding the tolerability of DTG in a real-life setting. Some publications have reported variable rates of drug discontinuation due to drug-related adverse effects, 23 –25 in contrast with more recent evidence indicating a good tolerability profile. 26 –28
The aim of this study was to evaluate the efficacy, safety, and tolerability of switching to a DTG-based regimen in a cohort of persons with HIV-1 infection with a stable virologic control. In addition, the dynamics of viral reservoir (total HIV DNA) and levels of high-sensitivity c-reactive protein (hsCRP), interleukin-6 (IL-6), soluble-CD14 (sCD14), and D-Dimer were analyzed.
Materials and Methods
An observational study was conducted on patients with HIV-1, attending Umberto I University Hospital, who have switched to a DTG-based regimen. All patients were adults and underwent suppressive antiretroviral therapy for a median of 72 (IQR 40–92) weeks. Plasmatic HIV RNA, CD4+ T cell count, weight, and levels of laboratory parameters related to hepatic, hematological, and renal functions were recorded at baseline (W0, corresponding to the time of regimen change), after 24 (W24) and 48 (W48) weeks of treatment for all study participants. Furthermore, in a subgroup of 34 patients, HIV DNA levels were monitored until W24 and inflammation/coagulation markers were analyzed at W0 and W24.
Plasma and peripheral blood mononuclear cell (PBMC) samples were collected at each time point and stored at −80°C until needed.
The study was authorized by the local Ethics Committee and written informed consent for the anonymous use of clinical and biological data was obtained from all patients (Protocol No. 3673).
Plasmatic HIV RNA was quantified using Versant HIV-1 RNA 1.0 kPCR assay (Siemens Healthcare Diagnostics) with a limit of detection of 37 copies/mL. This assay provides two possible outputs: a quantitative result for HIV RNA values ranging from ≥37 to 11,000,000 copies/mL; a qualitative result for HIV RNA values between 1 and 37 copies/mL, and an “undetectable” result if no signal can be detected.
PBMCs were obtained by Ficoll-Hypaque density gradient centrifugation. Total DNA was extracted from PBMCs using a QIAmp DNA Mini Kit (Qiagen, Hilden, Germany) and DNA quality and quantity were assessed by a NanoDrop 2000 Spectrophotometer (Thermo Scientific). Quantification of total HIV DNA was performed by using the commercial kit “Biocentric Generic HIV DNA Cell” (Biocentric, Bandol, France), which amplifies the long terminal repeat region of viral DNA. To reduce variations, all samples from a single patient were analyzed at the same time.
Stored plasma specimens, collected at W0 and W24, were used to evaluate hsCRP and IL-6 as inflammation markers, sCD14 as a marker of bacterial LPS-induced monocyte/macrophage activation, and D-Dimer as a marker of hypercoagulability. All samples were assayed using enzyme-linked immunosorbent assay kit (Abcam Human SimpleStep kit for D-Dimer; R&D Systems Quantikine for sCD14 and IL-6; BioVendor Human hsCRP for hsCRP) according to manufacturer's instructions.
CD4+ T cell counts, estimated glomerular filtration rate (eGFR, measured using the CKD-EPI formula), levels of creatinine, alanine aminotransferase and aspartate aminotransferase, total cholesterol, triglycerides, low-density lipoprotein and high-density lipoprotein, platelets, hemoglobin, and body mass index (BMI, calculated by dividing weight in kilograms by height in meters squared) were recorded at baseline, week 24 and 48.
Levels of virological, biochemical parameters, and inflammation/coagulation markers were described using median and interquartile range (IQR) and comparative analysis between the different time-points was performed by nonparametric Mann–Whitney U test. The p values were adjusted for multiple comparisons by the Bonferroni method. Differences in inflammation/coagulation marker levels deemed significant with p < .05, while comparison between each time points for HIV DNA and biochemical parameters were considered significant with p < .0083 and p < .016, respectively. All statistical analyses and graphs were computed using GraphPad Prism version 6.
Results
Ninety-six individuals who switched to a DTG-containing regimen were followed up for 48 weeks. At baseline, patients were on a stable suppressive cART for a median of 72 (40–92) weeks. The main characteristics at baseline are summarized in Table 1. Overall, the population composition was 74% male, median age 53 years (45–57), and median duration of HIV-1 infection and cART before enrolment were 17 (10–23) and 16 (10–21) years, respectively. The main risk factor for HIV-1 infection was unprotected heterosexual intercourse with 37.5%, followed by being men who have sex with men with 35.4%, injection drug use with 18.7%, and other with 8.5%. Hepatitis B virus coinfection was detected in 1 patient, while 12 patients were positive for antihepatitis C virus antibodies.
Characteristics at Baseline of 96 Patients
cART, combined antiretroviral therapy; DTG, dolutegravir; HBV/HCV, hepatitis B or C virus; INSTI, integrase strand transfer inhibitor; IQR, interquartile range; MSM, men who have sex with men; MVC, maraviroc; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
The decision to switch cART was made because of an adverse event to the previous treatment or a simplification strategy aimed at reducing drug burden or daily doses/pills.
At switch, 65 subjects were taking a triple-drug regimen being the most common backbones 2 nucleoside reverse transcriptase inhibitors (NRTIs, 62 patients) or protease inhibitor plus integrase inhibitor (PI+INSTI, 3 patients). In addition, 29 subjects were on a dual therapy based on PI in combination with INSTIs (25 patients), NRTIs (3 patients) or non-NRTIs (NNRTIs; 1 patient). Only two subjects were on monotherapy with a boosted PI. Overall, 34 patients have been previously treated with INSTIs (33 raltegravir; 1 elvitegravir) and no mutations of resistance have been detected.
As shown in Table 1, 61.5% (59 patients) switched to triple-drug regimens containing DTG +2 NRTIs, whereas 38.5% (37 patients) changed to DTG-based dual therapy in combination with a PI (19 patients), an NNRTI (12 patients) or an NRTI (6 patients). In the latter group, 13 subjects have simplified to DTG-based less drug regimens in combination with rilpivirine (7 patients), lamivudine (4 patients) or darunavir/cobicistat (2 patients). Among 96 study participants, the prevalence of hypertension was 23.9%, whereas 22.9% and 8.3% of patients were found to be dyslipidemic and diabetic, respectively.
Plasma levels of HIV RNA and CD4+ T cell count were obtained from patients' monitoring as a part of routine analyses in the clinical practice. At enrollment, all study participants had HIV RNA levels <37 copies/mL and most of them (96.8%) maintained virological suppression throughout the follow-up, including all patients who switched to dual-therapy from previous triple-drug combination. Eighteen out of 96 patients had viral load below 37 copies/mL but detectable (HIV-RNA 5–37 copies/mL) at baseline, of which 13 patients reached the maximal viral suppression at week 48.
The median CD4+ T cell count showed a slight but not significant increase from 700 cells/μL (IQR 519–885) before starting DTG-based regimen to 772 cells/μL (IQR 521–955) at W48 (p = .239).
Table 2 showcases the changes in laboratory/clinical parameters over the 48 weeks. As shown, serum creatinine levels showed a significant increase at weeks 24 and 48 [W0 0.90 (0.80–1) vs. W24 1 (0.85–1.1), p = .01; W0 vs. W48 0.99 (0.9–1.14), p = .0006], without exceeding the reference values. Besides, in accordance with the increase of creatinine levels, a significant decrease was observed in eGFR values at 24 and 48 weeks [W0 90 (79–102) vs. W24 82 (71–95), p = .01; W0 vs. W48 81 (70–94), p = .003].
Changes in Laboratory/Clinical Parameters During the Follow-Up for 96 Patients
Data are presented as median value (IQR). p ≤ .016 was considered as significant (Bonferroni correction).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; HGB, hemoglobin; LDL-C, low-density lipoprotein cholesterol; PLT, platelets.
A marked and progressive reduction of total cholesterol was observed from week 24 and up to week 48 of treatment [W0 209 (181–232) vs. W24 190 (159–219), p = .003; W0 vs. W48 190.5 (174–216), p = .01].
Furthermore, the trends of the above-mentioned parameters were stable, even stratifying the population into two groups according to the drug burden in the switch regimen (dual- or triple-drug combination). Although no differences were observed at baseline between groups, a slight but significant increase in creatinine levels and a significant reduction of total cholesterol were maintained in both groups at W48 (data not shown). Moreover, median changes from baseline in CD4+ cell count at W48 were 63 and −19 cells/μL for triple and dual regimen, respectively, without statistically significant difference (p = .093). No variation in BMI was observed after 48 weeks of treatment.
For 34 of 96 patients enrolled, HIV-DNA and inflammation/coagulation markers (hsCRP, IL-6, sCD14, and D-Dimer) were also analyzed on the same blood draw. Characteristics at the time of enrollment are shown in Table 3.
Baseline characteristics of all 34 patients in the subgroup
HIV-RNA levels remained unmodified below the limit of detection during the study period.
For viral reservoir quantification in the subgroup of 34 participants, all samples were suitable to measure total HIV DNA at baseline, while after 2 weeks (W2), 12 weeks (W12), and 24 weeks (W24), only 26, 28, and 24 samples were available, respectively.
Median total HIV DNA quantification at baseline was 2.84 log copies/106 PBMCs (2.45–3.12) and no significant variation was found at W2 [2.82 log copies/106 PBMCs (2.55–3.13), p = .791]; W12 [2.78 log copies/106 PBMCs (2.46–3.07), p = .692], and W24 [2.86 log copies/106 PBMCs (2.56–3.06), p = .902] (Fig. 1a).
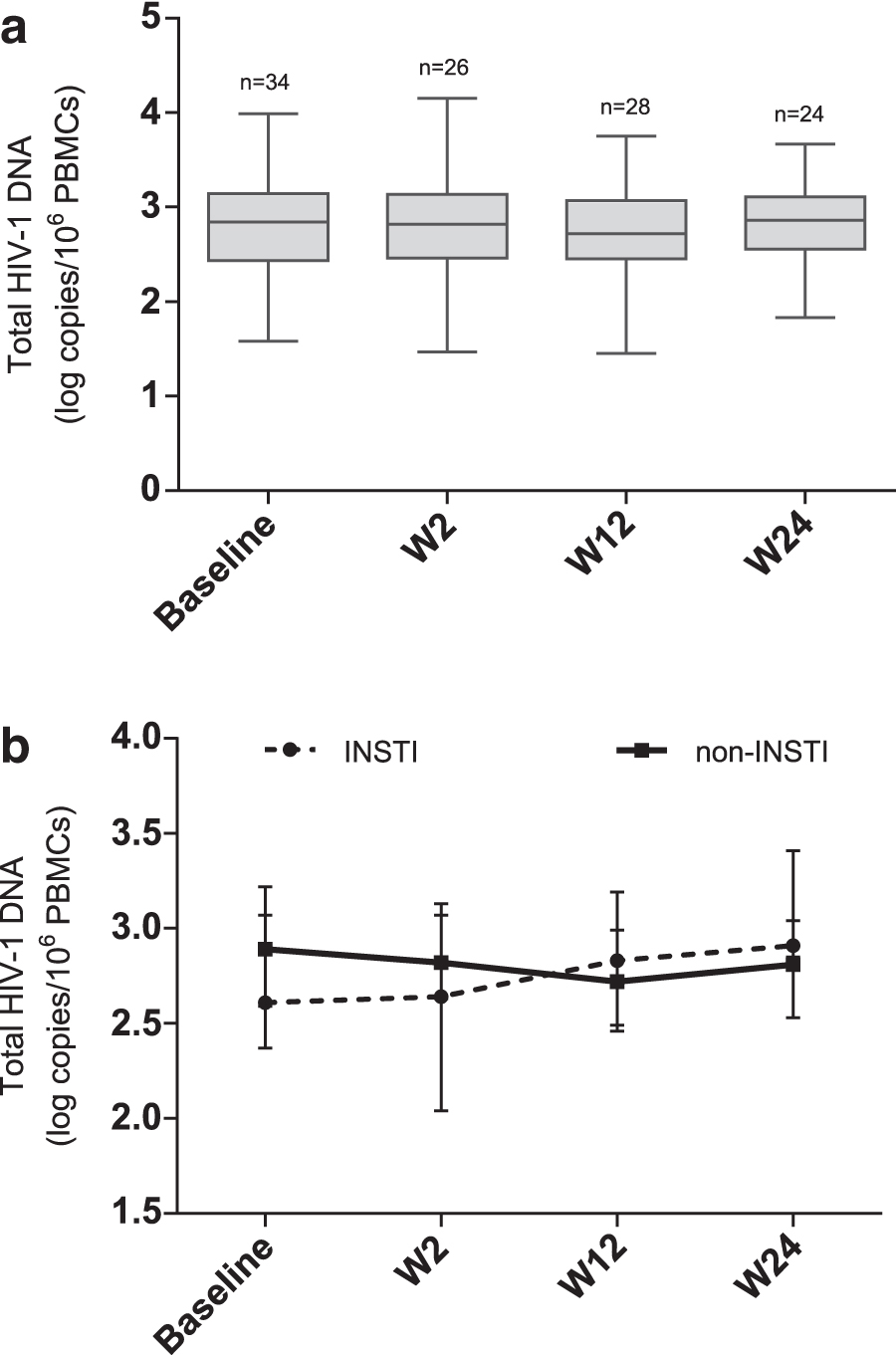
In this subgroup, patients were further divided into 2 groups based on previous exposure to integrase strand transfer inhibitors: INSTI group included 14 patients previously treated with raltegravir, whereas non-INSTI comprised 20 patients never been exposed to integrase inhibitors. The median values of total HIV DNA showed no significant variations from baseline to the end of follow-up in both groups [INSTI: 2.61 log copies/106 PBMCs (2.37–3.22) vs. 2.91 log copies/106 PBMCs (2.85–3.41), p = .167; non-INSTI: 2.89 log copies/106 PBMCs (2.59–3.07) vs. 2.81 log copies/106 PBMCs (2.53–3.04), p = .687] (Fig. 1b). More in depth, median HIV DNA levels in the INSTI group were 2.64 log copies/106 PBMCs (2.04–3.13) at W2 and 2.83 log copies/106 PBMCs (2.49–3.19) at W12. In the non-INST, the total HIV DNA amount was 2.82 log copies/106 PBMCs (2.63–3.07) at W2 and 2.72 log copies/106 PBMCs (2.46–2.99) at W24. Also, no differences were found between the two groups at each time point (data not shown).
Among the subgroup of 34 individuals, plasmatic levels of hsCRP, IL-6, sCD14, and D-Dimer were measured for all participants at entry and after 24 weeks to assess the overall differences in terms of systemic inflammation and coagulation.
Despite no significant variations in inflammation and coagulation markers levels, a slight decrease of IL-6 and sCD14 and an increase of D-Dimer levels was observed (Fig. 2). In addition, no significant difference was observed when subgroup (n = 34) was stratified based on the previous intake of INSTIs or between patients with detectable viremia (n = 13) and patients with undetectable viremia (n = 21) at baseline (data not shown). Considering the importance of CD4 T cell counts for monitoring immune reconstitution, CD4s have been correlated with inflammation markers' levels without showing a significant trend (data not shown).
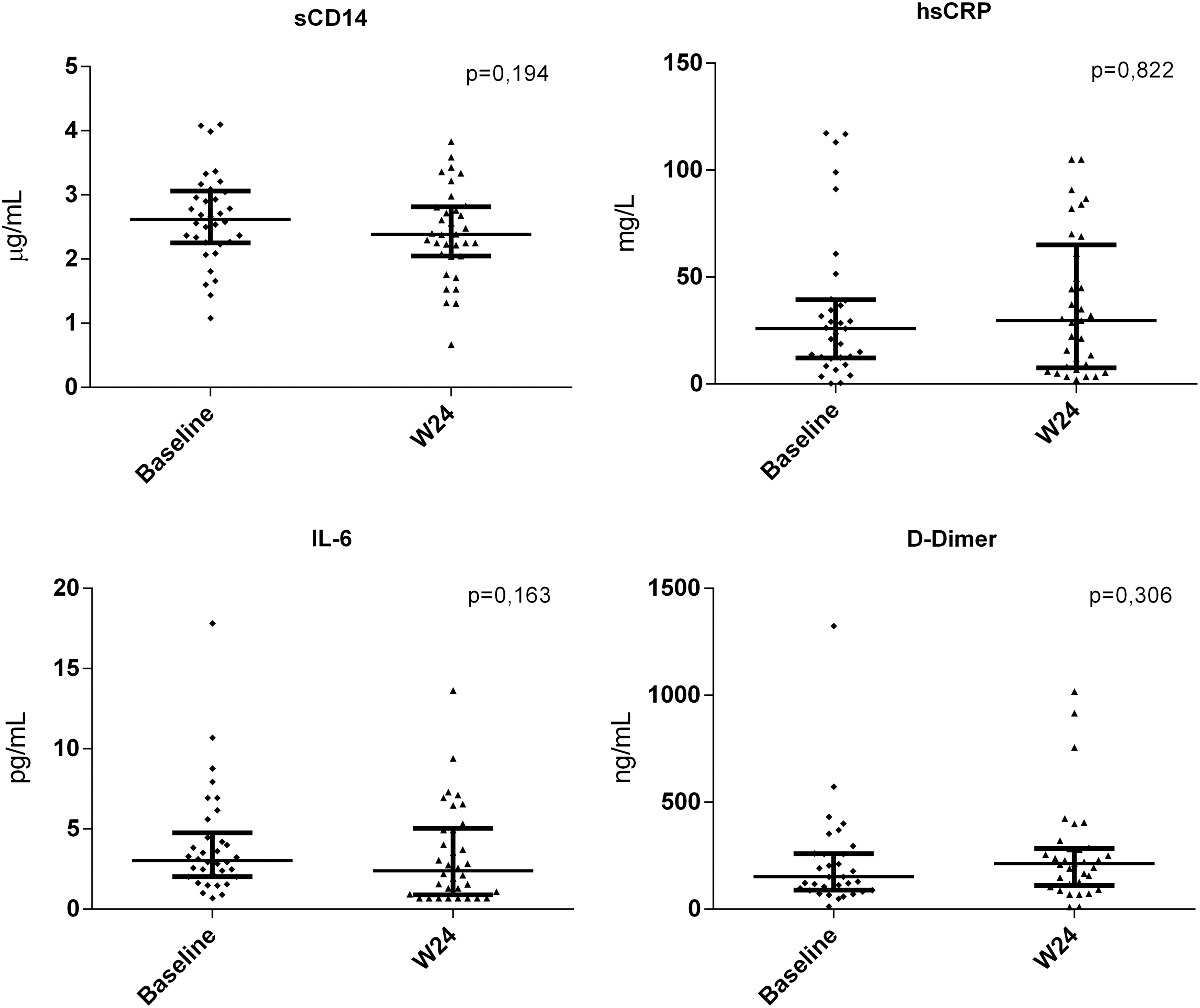
Levels of soluble CD14, hsCRP, IL-6 and D-Dimer within serum in a subgroup of 34 virologically suppressed patients who have switched to DTG-based regimens. p Value ≤.05 were considered statistically significant. hsCRP, high-sensitivity c-reactive protein; IL-6, interleukin-6.
According to the results of randomized clinical trials with DTG, adverse events leading to drug discontinuation were sporadic in the study population. Discontinuation of DTG treatment occurred only in three patients (3.1%), mainly due to drug-related adverse events such as anxiety and insomnia.
Discussion
The advent of integrase inhibitors has radically changed the clinical management of patients with HIV infection. To date, due to outstanding antiviral efficacy and safety profile, DTG is recommended for the treatment of both naive and experienced patients. 9,10 Furthermore, several clinical trials show the potential of DTG-based dual therapy as a simplification strategy to improve adherence and reduce cART toxicity and drug–drug interaction. 18 –20 Given the broad and growing use of DTG, it has become important to assess its tolerability and safety profile in a real-life setting.
In this observational study, a high rate of virologic suppression (96,8%) was maintained in the entire population over 48 weeks, regardless of the type of DTG-based regimen started. Moreover, 13 out of 18 patients who had detectable viremia at entry reached maximal virological suppression at week 48. Only three patients who switched to DTG/abacavir/lamivudine showed detectable viremia (<100 copies/mL) at the end of the follow-up. All three individuals were reported as adherent to antiretroviral therapy with no evidence of treatment-emergent resistance, zenith HIV RNA <500,000 copies/mL, and no experience of viral blips for two out of three. It is noteworthy that two of them had residual viremia (<37 copies/mL) before switching, while the third subject had suspended antiretroviral drugs due to the treatment of melanoma. Even when the population was stratified according to the type of treatment after the switch (dual regimen vs. triple regimen), a high virological efficacy was maintained. These results confirm the potency of DTG in countering HIV replication.
Drug-sparing strategies have gained increasing interest in the last few years, even as maintenance options in virologically suppressed patients. Data from clinical practice have shown that switching to a dual combination of DTG plus lamivudine or rilpivirine was effective and safe. 22,29 Further evidence of the potency of DTG plus lamivudine was provided by an observational study performed by Borghetti et al. that highlighted its comparable efficacy and greater durability when compared to the combination lamivudine plus PIs. 30 Likewise, DTG has been shown to be effective even in combination with ritonavir or cobicistat-boosted darunavir both as a rescue therapy (because of the combined high genetic barrier), as well as simplification strategy. 31,32
Although our patients in dual therapy showed a high rate of second antiviral agent heterogeneity, the remarkable efficacy observed in viral replication control reflects what is reported in the studies mentioned above.
In the last years, more attention has been paid to the impact of different antiretroviral regimens on the latent HIV reservoir. Falasca et al. showed a reduction in integrated HIV DNA levels 52 weeks after switching to an INSTI-based regimen and not matched by a concomitant decrease in total HIV DNA loads; it should be noted that the work was carried out on viraemic patients at baseline, and total HIV DNA levels could be maintained either by unintegrated viral DNA produced following the inhibition of the integration process, or migration from sanctuary sites to the peripheral blood of cells that contain unintegrated viral DNA. 33
Several studies have also focused on the dynamics of HIV reservoir in virologically suppressed patients showing, in specific conditions, a reduction of the HIV DNA levels in this population. 34,35
Recently, Lombardi et al. reported that maintainence therapy with DTG/lamivudine had the same impact as the triple regimen on HIV DNA levels after 48 weeks of treatment. 36
Here, to assess whether the switch to a DTG-based regimen impacted the size of the viral reservoir, we analyzed the dynamics of total HIV DNA within a short period of time starting from the switch in a subgroup of 34 patients that switched to DTG/abacavir/lamivudine. The analysis showed minimal changes in total HIV DNA levels across 24 weeks in these subjects, even if the patients were stratified based on their previous intake of integrase inhibitors. To note, patients have been subject to treatment for a long time (median of 16 years), and at the beginning of the study they were virologically suppressed for a median of 60 weeks. Moreover, only few individuals analyzed in this study showed residual viremia suggesting that the contribution of unintegrated forms to the size of the total HIV DNA burden could be considered negligible. Consequently, our observation reflects the dynamics of the viral reservoir that, after years of cART and control of viral replication, seems to reach a plateau phase. 37 It has been reported that during this phase, viral reservoir is mostly represented by integrated forms that persist in the memory CD4+ T cell subset. 38
Commonly, surrogate markers used to monitor patients with HIV are plasma HIV RNA to assess viral replication and CD4 T cell count to evaluate immune function. 9,10 Although combined antiretroviral treatment can effectively control viral replication and favor CD4+ T cells reconstitution, chronic immune activation and inflammation persist in treated patients and have been linked with the onset of severe non-AIDS events that would generally occur in the elderly population. 3,4 In a previous study, we showed a significant variation in sCD14 and tumor necrosis factor α levels, even among patients with undetectable and residual viremia, 39 indicating that minimal changes in the viral load could continue to affect the immune activation and the inflammatory response.
In this setting, in a comprehensive study by Castillo-Mancilla et al. it was also reported that suboptimal adherence to cART could have negative effects on residual inflammation and immune activation even in patients with long-term HIV suppression. 40
Although there seems to be an association between systemic inflammation and HIV viral load, there is a lack of data concerning the impact of the different antiretroviral drugs on residual inflammation.
In agreement with the maintenance of viral suppression, in our study, the therapeutic switch to DTG-containing regimen did not affect the levels of IL-6, hsCRP, sCD14, and D-Dimer even in patients who switched to dual therapy. These levels, almost unchanged over time, could be justified by the optimal adherence to cART reported for all patients before and during the follow-up, excluding one person for missing data. Furthermore, from the comorbidity perspective, clinical condition of the patients remained stable during the observation period.
Previous findings have shown that adults who switched from non-INSTI to INSTI antiretroviral treatment significantly increase weight and BMI. 41,42 Here, we found no evidence of BMI index increase in patients receiving DTG for 48 weeks and it is probably due to a shorter observation period than the evidence reported in the literature.
To verify the tolerability profile of DTG-based regimen, in the whole population enrolled, several blood analytes were measured throughout 48 weeks.
It has been shown how the inhibition of renal cation transporter 2 (OCT2) by DTG can lead to an increase of creatinine concentration. 43 A slight significant increase in serum creatinine was observed and maintained at week 48 regardless of the switching therapy. Despite the rise of creatinine levels, our population did not reach pathological values.
Moreover, in our study, a significant decrease of eGFR after 24 and 48 weeks of DTG use was found. These results are consistent with findings in the “early-switch arm” of the STRIIVING study, where patients who had switched from the beginning to DTG/abacavir/lamivudine showed an increase of creatinine concentration and concomitant decrease of eGFR at weeks 24 and 48. 16 Changes in eGFR have also been reported in the dual combination setting of DTG plus rilpivirine, lamivudine, or darunavir. 29 –32 This finding could be due to the increase of serum creatinine and did not support a causal effect of DTG on eGFR levels.
It is known that the incidence of metabolic disorders is greater in patients with HIV infection than in healthy population. 3,4 As a result, it is crucial to evaluate the impact of different drugs on the lipid profile during antiretroviral therapy assignments, especially in patients at high risk for cardiovascular diseases. Although DTG has shown a neutral effect on serum lipids on comparative clinical trials, 44 we found a marked decrease in total cholesterol over 24 weeks, further confirmed at week 48. These findings are consistent with previous observations, 45,46 although in our population, only 46% of subjects switched from boosted PIs (n = 33)- or efavirenz (n = 11)-based regimens, known to be associated with dyslipidemia. 9 The observed reduction of total cholesterol could be due to the continued intake of statins from several patients throughout the follow-up.
The discontinuation rate in this analysis is 3% approximately and due to neuropsychiatric adverse events, such as the occurrence of anxiety and insomnia, observed within 3 months from starting the DTG treatment. Despite the lower incidence of discontinuation (3.1% vs. 5.6%), the early appearance of these side effects reflects the early discontinuation reported by Hoffman et al. 24 in a large Dutch cohort.
Conclusions
Our study has several limitations, mainly related to the small size of the study population and the high heterogeneity of both previous treatments and drugs in association with DTG in the switch regimens, which do not allow to generalize what has been observed. Nonetheless, despite these limitations, our data further support the evidence that switching to a DTG-based regimen may be a key option for achieving and maintaining maximal virological suppression, even in patients showing residual viremia at baseline.
Furthermore, with the substantial increase in the number of HIV-infected patients aged 50 years or older, the improvement in blood lipid profile and the overall tolerability observed in this study strongly support the use of these regimens in aging HIV population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the PRIN 2015 (Progetti di ricerca di Rilevante Interesse Nazionale 2015).