
Abstract
HIV-associated neurocognitive disorder (HAND) covers a spectrum of neurological and cognitive dysfunction affecting the day-to-day life of persons infected with HIV. Although neurological complications are believed to be significantly reduced upon administration of effective and stable combined antiretroviral therapy (cART), there is evidence to suggest that persons with chronic HIV-1 infection exhibit an increased prevalence of milder forms of cognitive decline despite effective treatment. 1
In an effort to examine metabolic alterations associated with HIV-1 infection that are known to impact the brain and cause neuropathological conditions, we evaluated a cohort of 22 HIV-1–infected persons with a median age of 45 years on standardized first-line ART regimen (zidovudine/tenofovir and lamivudine with nevirapine/efavirenz) for a median duration of 9 years and compared their metabolic profile with that of an equal number of age-matched HIV-uninfected control subjects. Blood samples were collected, processed for plasma separation, and subjected to untargeted metabolomics using ultrahigh-performance liquid chromatography/mass spectrometry/mass spectrometry (UHPLC/MS/MS). Welch's two-sample t-test was used to identify metabolites that were significantly different (p ≤ .05) between the two groups.
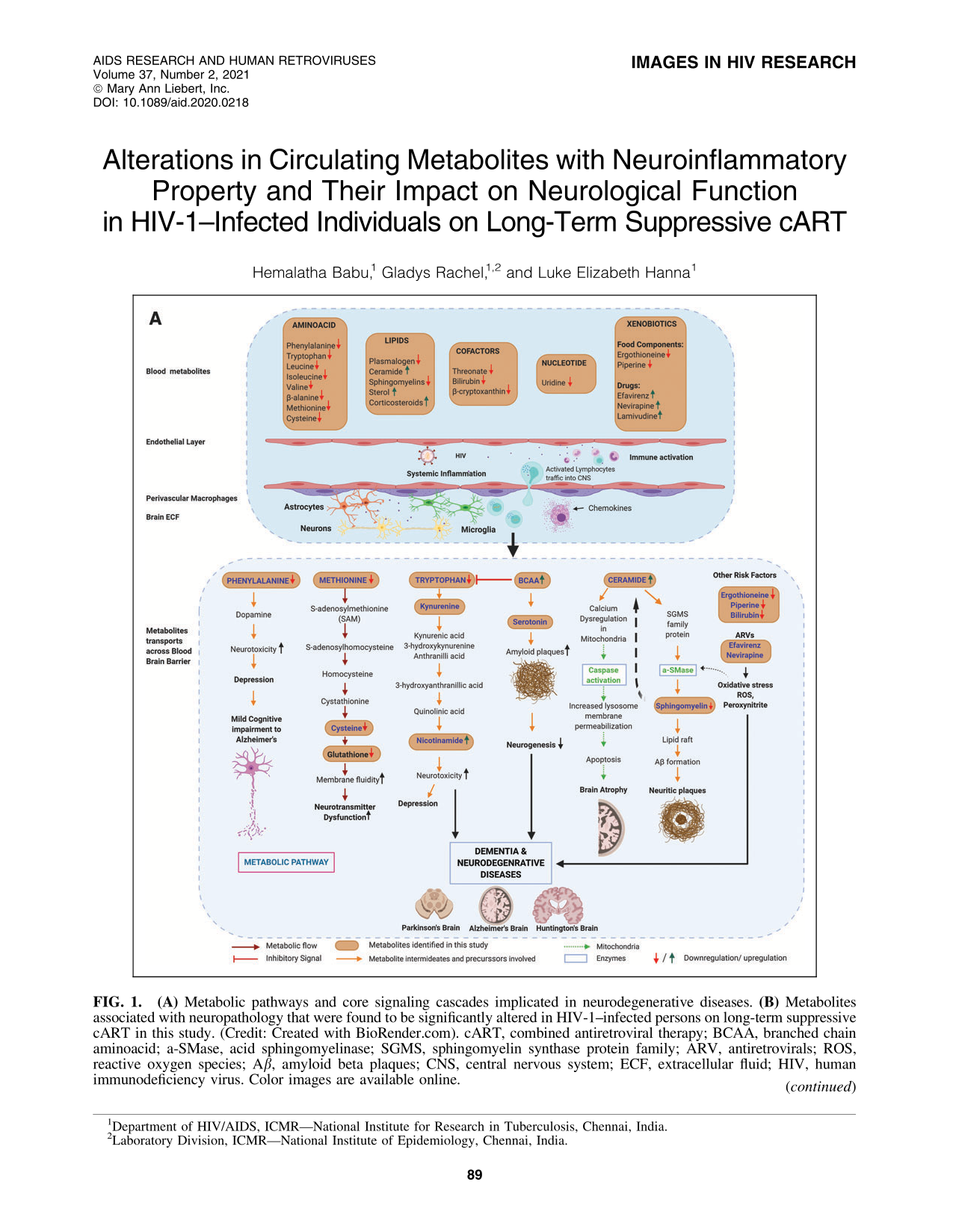
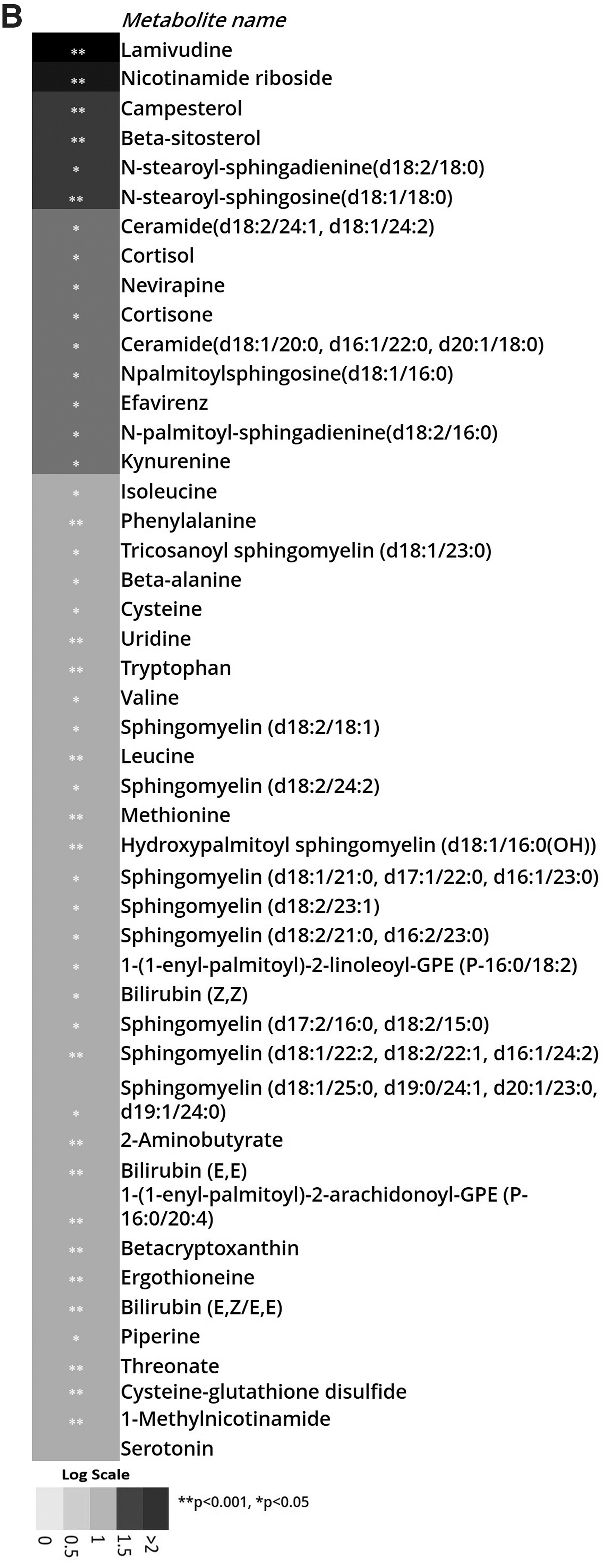
We observed significant alterations in the levels of several blood metabolites that possess the ability to penetrate the blood–brain barrier and impact neurological pathways in HIV-1–infected persons, clearly indicating a higher risk for neuropathological conditions in these individuals despite effective long-term ART (Fig. 1). Levels of essential amino acids such as phenylalanine, methionine, cysteine, and tryptophan, as well as branched-chain amino acids, known to play an important role in maintaining neurotransmitter and cognitive function, were found to be significantly lower in the HIV-1–positive group. Increased levels of ceramides and decreased levels of sphingomyelin were also observed, indicating an increased risk of mitochondrial dysfunction and β-amyloid protein formation in the central nervous system. Besides alterations in the classic biomarkers of neurological disease such as tau and amyloid β (Aβ) peptides in cerebrospinal fluid (CSF) and blood, 2 similar studies have reported alterations in several endogenous and diet-derived metabolites associated with cognitive abnormalities. We also found higher levels of metabolites such as ergothioneine, piperine, and bilirubin, as well as antiretroviral drugs such as nevirapine and efavirenz in HIV-1–infected persons. These metabolites may contribute significantly to neuropathology by increasing oxidative stress and inflammation levels. Elevated systemic inflammation and machine learning predictions of inflammatory and neurological disease risks in HIV-1–infected persons from our previous studies also provide supportive evidence for the observed metabolic abnormalities associated with the central nervous system in HIV-1–infected individuals despite long-term suppressive ART. 3,4

To summarize, we identified alterations in levels of circulating metabolites that could increase the risk of developing neurological disorders in HIV-1–infected patients despite viral suppression. Even though neuronal cells are not directly infected by HIV-1, low-level replication in reservoirs such as microglia, accumulation of viral tat protein, blood–brain barrier injury, inflammation, and antiretroviral toxicity along with this metabolic imbalance can cause structural and functional damage to the brain, thus affecting cognitive ability and lead to neurodegeneration in a worst-case scenario.