
Abstract
The analysis of a pol gene fragment encoding protease and part of reverse transcriptase was carried out for 55 sera collected in 2016 and 2018 from HIV-1-infected patients diagnosed in 2014–2018 living in the south of Western Siberia, Russia: Altai Territory (n = 11), Republic of Altai (n = 15), Kemerovo region (n = 18), and Novosibirsk region (n = 11). CRF63_02A was the dominant genetic form (>70%) in the Altai Territory and Kemerovo and Novosibirsk regions, with subsubtype A6 comprising <30% of samples. In the Altai Republic, subsubtype A6 was predominant (53%), with 33% of viruses belonging to CRF63_02A. Four CRF63_02A/A6 unique recombinant forms were identified in the Altai Territory, Kemerovo Region, and the Altai Republic. A majority (11 of 15) of CRF63_02A viruses from Kemerovo were grouped in a cluster. Antiretroviral (ARV) drug resistance mutations were found in 6 (14%) of 43 drug-naive patients. This study provides new insights in HIV-1 molecular epidemiology and prevalence of transmitted ARV drug resistance mutations in Southwestern Siberia.
Introduction
Currently, about 37 million people in the world are living with HIV-1, which makes this disease one of the leading global public health problems. Despite decades of intensive research, due to the great ability of the virus to elude the immune response, an effective strategy to cure HIV-1 infection has not been developed yet.
Russia is one of the leading countries in HIV-1 incidence in the world, surpassing some African countries. According to the molecular epidemiological analysis of HIV-1 isolates circulating in Russia, the A6 subsubtype continues to dominate in most of the Russian Federation, with the exception of some areas of Siberia, where the recombinant variant CRF063_02A prevails, with lower prevalences of CRF02_AG and unique recombinant forms (URF). 1 –5 In 2019 and 2020, according to the official data from the Federal Scientific and Methodological Centre for the Prevention and Control of AIDS, the majority of HIV-positive patients in Russia became infected through heterosexual contact (62.7% and 65%, respectively), and the proportion of HIV infections acquired through drug use was decreasing (33.6% and 31.5%, respectively), with 2.5% infections diagnosed in men who have sex with men. 6 This represents a change in the predominant transmission route compared to 2015, when among newly HIV-diagnosed persons, 52.3% became infected through drug use, 45.1% through heterosexual contact, and 1.5% infections were diagnosed in men who have sex with men. 6
Currently, in the Russian Federation, 770,122 HIV-infected patients are under regular medical follow-up, which is 68.8% of the people living with a diagnosis of HIV infection. Of these, 581,555 patients receive antiretroviral (ARV) therapy, corresponding to a treatment coverage of 52.0% of people living with HIV and of 75.5% of those who are under medical follow-up. 6
According to the Central Scientific Research Institute of Epidemiology of the Federal Service on Customers' Rights Protection and Human Well-being Surveillance, in 2015, the primary HIV-1 ARV drug resistance rate in the Russian Federation was around 6% in 2015, and in 2017 in some regions of the country it increased to 9.7%. 7 If the ARV drug resistance in the population reaches 10%, this means that it is necessary to review the treatment strategy. 8 At the same time, according to the results of Kirichenko et al., the prevalence of transmitted drug resistance associated with mutations from the Surveillance Drug Resistance Mutation (SDRM) list in nine federal districts of the Russian Federation amounted to 5.3%, which is classified by World Health Organization as moderate. 9 The highest prevalence of drug resistance was found for nonnucleoside reverse transcriptase inhibitors (NNRTIs) (rilpivirin, nevirapine, and efavirenz). 9 In the neighboring country of Kazakhstan, a low prevalence (3%) of drug resistance mutations to ARV drugs in the group of untreated patients was noted. 10 Overall, ARV drug resistance in former Soviet Union countries has been reported to range from 3.4% in Latvia to 8.3% in Georgia. 11
The development of HIV-1 resistance derives from the selection of viruses bearing certain mutations, which occur in large numbers in the viral genome under the influence of various evolutionary factors, which include low accuracy of reverse transcriptase and high viral replication rates, and of other concomitant factors, such as poor patient compliance, inappropriate choice of ARV agent, and pharmacokinetic factors that can affect blood levels of ARV agents, including poor oral absorption. 12 At the same time, drug resistance appears not only in patients with ARV drug experience due to the occurrence of mutations (acquired) but also in patients without ARV drug experience (drug-naive patients) as a result of the transmission of HIV-1 variants that already contain resistance mutations (primary or transmitted). 13,14
This study aims to determine the genetic diversity and drug resistance mutations in reverse transcriptase and protease genes of HIV-1 isolates from Southwestern Siberia, the region most affected by HIV-1 in the Russian Federation.
Materials and Methods
Patients
The study included 55 sera from HIV-1-infected patients collected in 2016 and 2018: 11 from the Novosibirsk Region, provided by the Center for the Prevention and Control of AIDS and Infectious Diseases of Novosibirsk; 18 from the Kemerovo region, provided by the Kemerovo Regional Center for the Prevention and Control of AIDS and Infectious Diseases; 11 from the Altai Territory, provided by the Altai Regional Center for the Prevention and Control of AIDS and Infectious Diseases (Barnaul); and 15 from the Altai Republic, provided by the Center for the Prevention and Control of AIDS of the Republic of Altai. Serum samples were related to demographic and clinical data by anonymous codes according to the ethical requirements of the Russian Federation. All the procedures involving human objects were conducted in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 2013.
RNA extraction
The total RNA pool was isolated from the sera of HIV-1-infected patients using the QIAamp Viral RNA Mini Kit reagent kit (QIAGEN, Germany) and the RNA/DNA Reagent Kit from the MAGNO-sorb clinical material (AmpliSens, Russia) according to the manufacturer's recommendations.
Polymerase chain reaction and sequencing
Amplification of a fragment of the HIV-1 pol gene encoding protease and reverse transcriptase (PR-RT) was performed by reverse transcription-polymerase chain reaction (RT-PCR) followed by nested PCR as described previously. 2,15 The nucleotide sequence of the amplified fragments was obtained by the Sanger method using the BigDye Terminator v 1.1 Cycle Sequencing Kit (Applied Biosystems) on the ABI PRISM Genetic Analyzer 310 instrument at the Genomika Research Center, Novosibirsk, and ABI 3730 XL DNA Analyzer at Genomic Unit, Centro Nacional de Microbiología, Instituto de Salud Carlos III, Majadahonda, Madrid, Spain.
Sequence analysis
Electropherograms were assembled, analyzed, and edited using the SeqMan v6.1 (DNASTAR, Inc., Madison, WI) and BioEdit v7.2.5 (Tom Hall) programs. Multiple alignment of the nucleotide sequences was performed with MAFFT v7. 16 Phylogenetic analysis was performed using maximum likelihood with IQ-TREE v1.6.1217 using the general time reversible with FreeRate evolutionary model (GTR + R). Node support was assessed by ultrafast bootstrapping with 1,000 replicates. To construct the phylogenetic trees, reference sequences from the Los Alamos HIV Sequence Database were included. Recombination was analyzed by bootscanning using the SimPlot 3.5 program. 18 This analysis was done using a window of 180 nt moving in 20 nt increments, with tree construction using the neighbor-joining method and the Kimura 2-parameter substitution model.
ARV drug resistance mutations were determined using the HIVdb program at the Stanford University HIV Drug Resistance Database. 19 Levels of resistance to ARV drugs were determined according to the HIVdb program: 15–29, low level of resistance; 30–59, intermediate level of resistance; and 60 or more, high level of resistance.
Results
Epidemiological data
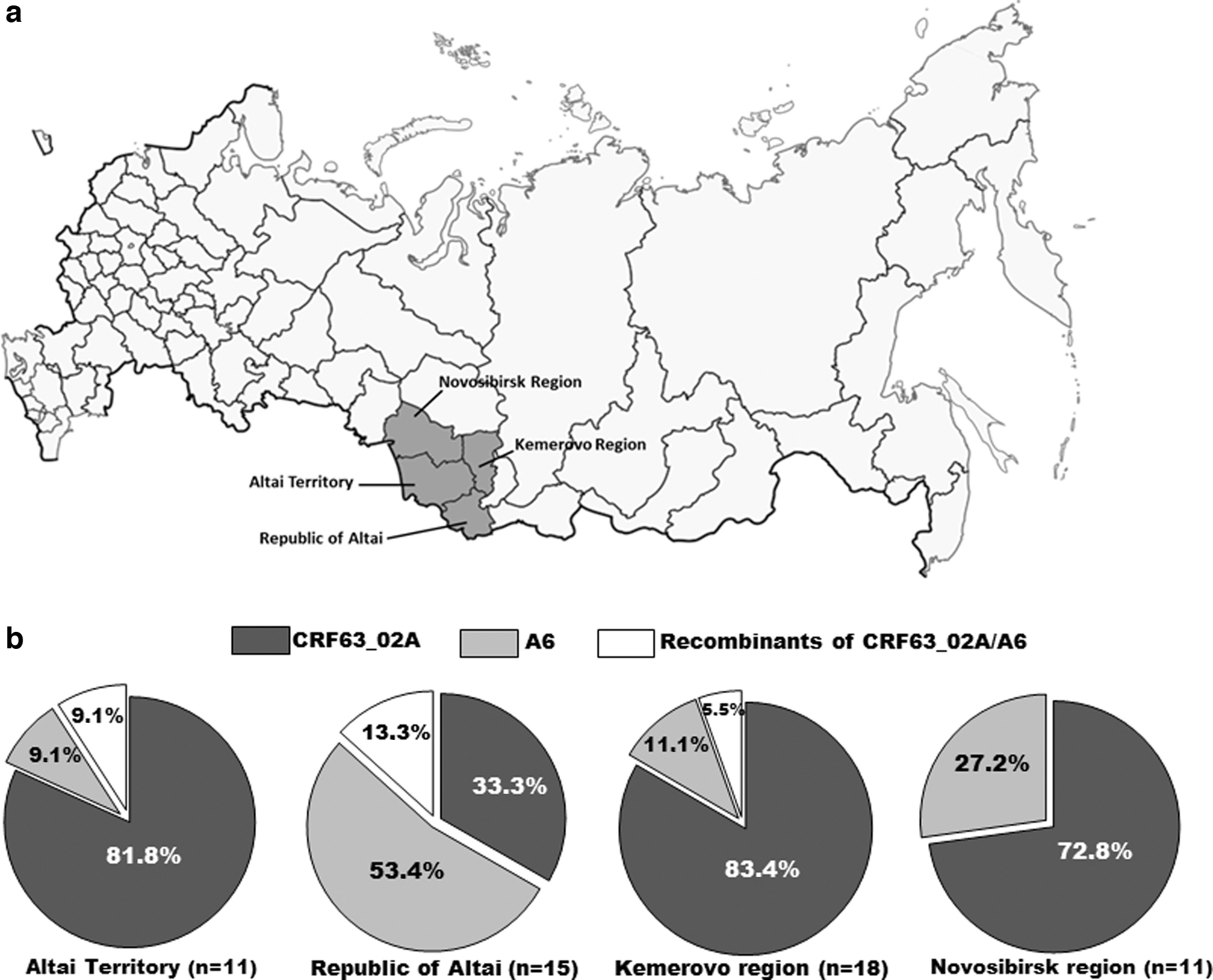
The study analyzed a total of 55 sera of HIV-positive patients living in the south of Western Siberia: Altai Territory (whose capital is Barnaul), the Republic of Altai (whose capital is Gorno-Altaisk), Kemerovo region (whose capital is Kemerovo), and Novosibirsk region (whose capital is Novosibirsk city) (Fig. 1a).
Data from HIV-1-infected patients (Table 1 and Supplementary Table S1) indicate that there were more men included in the study than women: 51.8% (29/55) men versus 48.2% (25/55) women. The average age of the patients was 38 ± 8.9 years (range, 25–62 years). In 58.2% (32 of 55) of cases with known transmission routes, infection occurred through heterosexual contact; in 34.5% (19 of 55), it was transmitted through intravenous drug use; and in 4 (7.3%) cases the transmission route could not be established. The proportion of patients on ART was 21.8% (12/55). Most of them (10 patients) were from the Altai Republic, and 2 were from the Altai Territory.
Summary Information of Samples Analyzed in This Study
ARV, antiretroviral; ABC, abacavir; FTC, emtricitabine; 3TC, lamivudine; TDF, tenofovir disoproxil fumarate; EFV, efavirenz; NVP, nevirapine; ART, antiretroviral therapy; ZDV, Zidovudine; LPV/r, lopinavir/ritonavir.
Phylogenetic analysis of pol gene
To molecularly characterize HIV infection, amplification of a portion of the pol gene encoding PR-RT was performed. The phylogenetic analysis of the amplified fragment showed that the recombinant form CRF63_02A prevails in the examined samples from three regions and that the A6 subsubtype also circulates in all four regions, reaching 53.4% in the Republic of Altai (Fig. 1b). Eleven of 15 (73.3%) CRF63_02A sequences from Kemerovo Region were grouped in a strongly supported cluster (Fig. 2).

Maximum likelihood phylogenetic tree of HIV-1 pol genes constructed with IQ-TREE. Only bootstrap values ≥90% are shown. Samples from this study are labeled with circles. CRF63/A6 recombinants are indicated with arrows.
Recombination analysis by bootscanning showed that among the 55 studied HIV-1 variants, 4 were CRF63_02A/A6 recombinants in PR-RT fragment: 1 (18RU04GA and 18RU14GA) from the Republic of Altai, 1 (16RU38) from the Altai Territory, and 1 (16RU39) from the Kemerovo Region (Fig. 3).
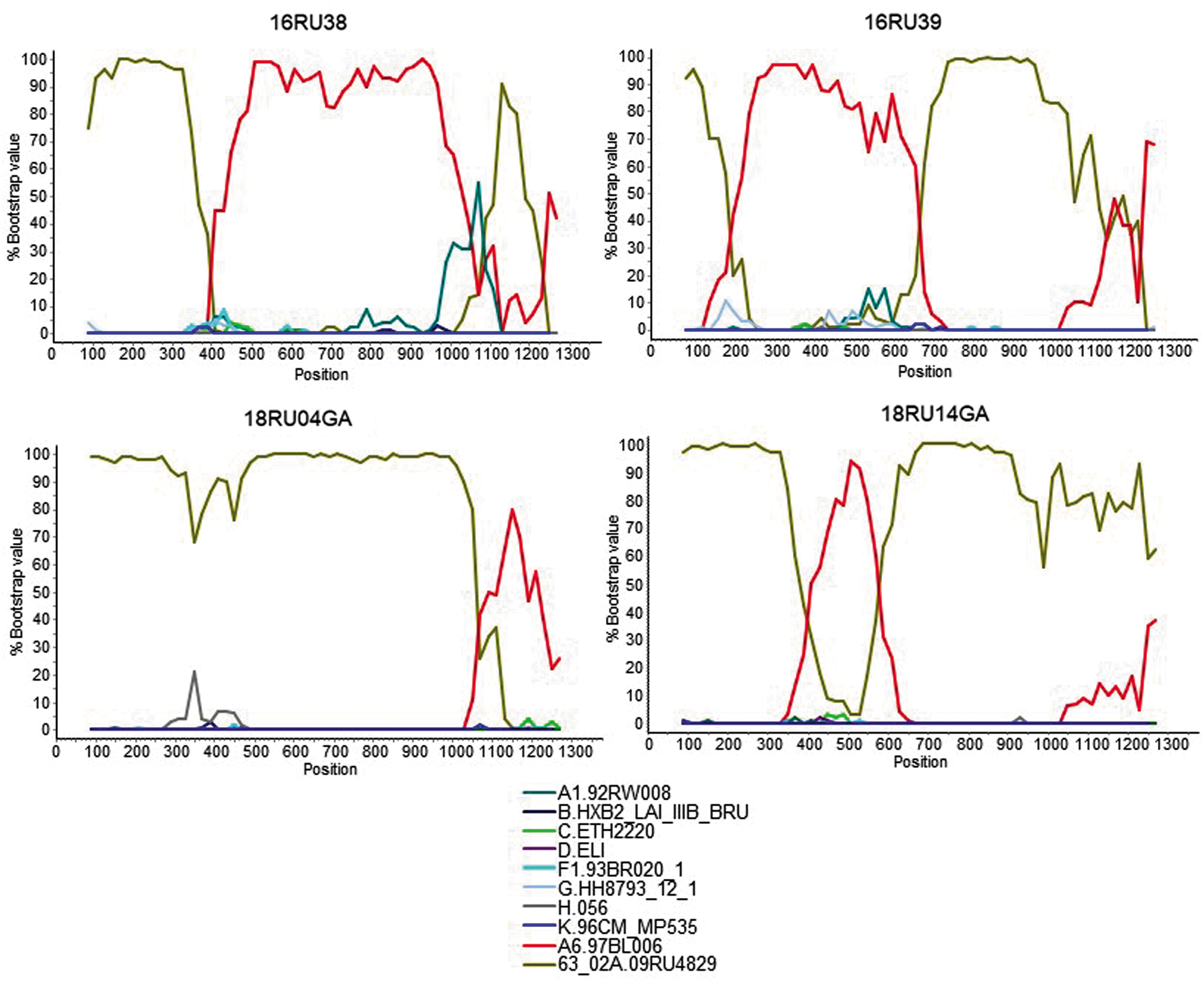
Bootscan analyses of four protease and reverse transcriptase CRF63_02A/A6 recombinant sequences from Siberia. Horizontal axis represents nt position from nt 1 of protease. Vertical axis represents bootstrap values supporting clustering with clade references, shown below.
Drug resistance mutations to protease inhibitors, nucleoside reverse transcriptase inhibitors, and NNRTIs
Major mutations associated with drug resistance to protease inhibitors (PIs) were not detected in the analyzed nucleotide sequences. Most of the studied samples contained polymorphic mutations K20I (70%), L10I/V (22%), and V11I (2%).
Regarding the reverse transcriptase segment, nucleoside reverse transcriptase inhibitor (NRTI) and NNRTI drug resistance mutations were detected (Table 2). Among the NRTI drug resistance mutations, M41L (in two drug-naive patients) and K65R (in two drug-naive patients) were found. The M41L mutation causes low levels of azidothymidine (AZT) resistance; and the K65R mutation results in a moderate level of resistance to abacavir (ABC), emtricitabine (FTC), and lamivudine (3TC) and a high level of resistance to tenofovir disoproxil fumarate (TDF). This represents a NRTI SDRM prevalence of 9.3% (4 out of 43 drug-naive patients analyzed). Among the mutations that confer resistance to NNRTI drugs, K103N, which leads to a high level of resistance to efavirenz (EFV) and nevirapine (NVP), was identified in three drug-naive patients. This represents an NNRTI SDRM prevalence of 7% (3 out of 43 drug-naive patients analyzed). In one drug-naive patient, two mutations, K65R and K103N, associated with resistence to different drug classes, were found. This represents a NRTI + NNRTI SDRM prevalence of 2.3% (1 out of 43 drug-naive patients analyzed). Thus, among the 43 drug-naive HIV-1-infected participants, 6 (14%) were infected with HIV-1 variants with SDRMs.
Sequences with Surveillance Drug Resistance Mutations
Mutations shown in bold correspond to WHO designated SDRMs.
SDRM, Surveillance Drug Resistance Mutation; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
Discussion
According to official statistics of the Federal Scientific and Methodological Centre for the Prevention and Control of AIDS, in 2019 the total number of HIV-infected people registered in the Russian Federation was 1,420,975. 6 The Siberian Federal District is one of the areas most affected by the HIV epidemic in the Russian Federation, with 280,788 HIV-infected individuals. 6 The leading regions in Siberia in terms of infection are Kemerovo, Novosibirsk, Tomsk, and Omsk regions and Krasnoyarsk and Altai Territories. 20 –25 In these regions, epidemiological surveillance of circulating strains is being carried out, and the dominant variants of HIV-1 have been identified in most of them. At the same time, information on the subtype of HIV-1 isolates in some regions is completely lacking. An example would be the Altai Republic. While infection rates are currently low in the region, there has been a significant increase in new infections in recent years. In the Altai Republic, for a total population of 220,181 inhabitants, 1,050 HIV-infected people were registered for all the years of observation (from 1999 to 2019). Of them, 597 persons were HIV diagnosed since 2015. In 2019, 696 HIV-positive patients were under regular medical follow-up.
In this work, we investigated the genetic diversity of HIV-1 isolates circulating in the south of Western Siberia, and we also analyzed the prevalence of HIV-1 drug-resistant strains in this territory and their mutation profiles.
Phylogenetic and recombination analyses showed that the recombinant form CRF63_02A continues to dominate in the south of Western Siberia, which occurs in more than 70% of cases in the Novosibirsk and Kemerovo regions and in the Altai Territory, with the A6 subsubtype accounting for <30% of isolates. At the same time, in the Altai Republic (where genetic diversity of circulating HIV-1 strains is first reported here) a different picture is observed in the distribution of HIV-1 subtypes; more than 50% of the studied circulating HIV-1 strains belong to the A6 subsubtype, and the proportion of CRF63_02A is 33% (Fig. 1b). The observed predominance of CRF63_02A in Novosibirsk and Kemerovo regions is in accordance with previous reports. 1,2 It is interesting to note that 11 of 15 (73.3%) CRF63_02A viruses from Kemerovo were grouped in a local cluster, indicating that most CRF63_02A infections from this region derive from a single introduction. This is similar to the reported A6 subsubtype clusters found in other areas of Russia. 26 –29 With regard to the Altai Territory, we observe a major shift in the genetic composition of the HIV-1 epidemic, with a change from A6 subsubtype predominance (100%) in samples collected in 200828 to CRF63_02A predominance (82%) in samples collected in 2016. In addition, it should be noted that among the isolates circulating in the territories of the Kemerovo Region, Altai Territory, and the Altai Republic, in isolated cases, CRF63_02A/A6 URF were identified. Similar recombinants are found in Siberia and are described in the literature. 1,20,21,25
Analysis of the protease gene showed no major mutations associated with the resistance to PI drugs. Nevertheless, most of the studied CRF63_02A and A6 strains contained polymorphic mutations K20I, L10I/V, and V11I in the protease gene. Among the mutations causing resistance to NRTI and NNRTI, M41L, K65R, and K103N were found. It should be noted that this mutation profile is typical and correlates with previously published data. 1,2,9,21 The overall prevalence of mutations associated with resistance to reverse transcriptase inhibitors was 14%, higher than the data obtained earlier for Russia, where the level of transmitted drug resistance was 5.3%. 9 The detection of such mutations in drug-naive patients indicates infection with a resistant variant of the virus and prevents the use of these drugs in the ART regimen.
Conclusion
The current molecular epidemiological situation of HIV-1 infection in the southwestern Siberian regions of Altai Territory, Republic of Altai, Kemerovo region, and Novosibirsk region is due to the circulation of CRF63_02A and the A6 subsubtype, which have given rise to cases of CRF63_02A/A6 recombinants. In this study, a relatively small group of people who received ARV therapy and those who did not take ARV drugs were examined. The number of studied samples does not allow to reliably assess the level of primary resistance in the studied sample; however, the frequency of transmitted drug resistance observed in this study was 14%. Research in this direction needs to be continued and expanded both for the purpose of monitoring the spread of HIV-1 drug-resistant strains and for studying the characteristics of the spread of HIV-1 variants in the regions of the Russian Federation.
Sequence Data
The HIV-1 protease-reverse transcriptase sequence data were submitted to the GenBank database under the accession numbers MT101799–MT101834 and MT811096–MT811114.
Footnotes
Authors' Contributions
N.B.R.: conceived and designed the analysis; collected the data; contributed data or analysis tools; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. N.S.S.: conceived and designed the analysis; collected the data; contributed data or analysis tools; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. D.N.S.: conceived and designed the analysis; collected the data; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. E.V.M.: collected the data; wrote the article; drafting the work or revising it critically for important intellectual content. E.D.: contributed data or analysis tools; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. A.A.I.: conceived and designed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. L.I.K.: conceived and designed the analysis; collected the data; contributed data or analysis tools; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published. M.M.T.: conceived and designed the analysis; contributed data or analysis tools; performed the analysis; wrote the article; drafting the work or revising it critically for important intellectual content; final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially funded by Russian Foundation for Basic Research (RFBR) and Novosibirsk region, according to the research project No. 19-44-543013, and was funded through Acción Estratégica en Salud Intramural, Instituto de Salud Carlos III, project “Estudios sobre vigilancia epidemiológica molecular del VIH-1 en España,” PI16CIII/00033.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.