
Abstract
There are about 2.1 million children infected with HIV globally and about 120,000 deaths annually. Nigeria has one of the highest rates of pediatric HIV infection globally. Pretreatment HIV drug resistance data inform the choice of first- and second-line antiretroviral therapy (ART) regimens. This study investigated the prevalence of HIV drug-resistant strains among ART-naive children in Ibadan, Nigeria. A total of 20 children aged <15 years were enrolled. Demographic, clinical, and laboratory data were documented. Total nucleic acid was extracted from blood samples after which amplification of HIV-1 pol gene was done using polymerase chain reaction. Amplified gene was sequenced using big dye sequencing method. The sequenced HIV-1 pol gene was typed and analyzed for identification of mutations indicative of drug resistance across the different classes of ART. HIV-1 RNA pol gene was successfully amplified in 12/20 (60%) children. All were identified as HIV-1 and the subtypes were G and CRF 02AG, recombinant of 02_AG/G and recombinant of 02_AG/A1. Drug-resistant mutations (DRMs) were identified in 4/12 (33%). Three out of the four mutations were identified as non-nucleoside reverse transcriptase inhibitors DRM (K103N), whereas the fourth had nucleoside reverse transcriptase inhibitors DRM (M184V). Results from this preliminary study show that drug resistance among ART-naive children is a problem in Ibadan. Pretreatment drug resistance testing is desirable in children before initiation of ART to guide effective treatment.
Introduction
There are about 1
Prevention of mother-to-child transmission (PMTCT) of HIV includes the use of combination ART for infected mothers during pregnancy and chemoprophylaxis of nevirapine and/or zidovudine for exposed children. Infected children are placed on ART for life. 10 There has been a rapid scale up of PMTCT in sub-Saharan Africa since 2010, which has reduced the burden of newly infected HIV children by 41%. 11 This gain is, however, constantly threatened by the selection and emergence of HIV drug resistant (HIVDR) variants especially in countries with limited or low access to treatments. HIVDR is due to several factors, which include the high rate of mutation of the virus and viral recombination of quasi species. 12,13 It could also be due to drug pressure in patients receiving ART because of suboptimal adherence, pharmacodynamic factors, or use of inadequate or suboptimal regimes. 12 The probability of drug resistance escalation during treatment has been estimated at 27% every 6 years, this is particularly a major threat for countries with limited treatment access for children. 13
According to World Health Organization (WHO), HIVDR can be classified as pretreatment drug resistance [PDR, (among ART initiators or re-initiators with or without prior exposure to ARVs)], transmitted drug resistance (TDR, among recently infected individuals with no prior exposure to ARVs), and acquired drug resistance (among infected individuals on ARVs treatment). PDR is either transmitted (at the time of infection) or acquired (by virtue of prior ARV drug exposure) drug resistance, or both. 14 This resistance may limit virological response to use of antiretroviral medications especially in children. 15,16 HIVDR also reduces or even eliminates the efficacy of ART, increasing the risk of treatment failure, which in the case of children leads to poor growth and immunological outocmes. 17 –19 Mutations in the HIV genome that cause HIVDR acquired during ART failure might limit the response to subsequent lines of treatment. 18
Mutations in the structural genes of HIV especially the pol gene that codes for reverse transcriptase, protease and integrase gene have been associated with drug resistance. 20 Some of the common mutations are M181V/I, K65R, K103N, V106M, and D67N, whereas a comprehensive database of possible mutations can be found at HIV Stanford database. 20 It is important to continually monitor emergence of drug resistance in children as this will greatly improve HIV control and treatment outcomes among this vulnerable population. Furthermore, a better understanding of the resistance and cross-resistance profiles among antiretroviral drugs is important for predicting response to treatment and surveillance of TDR.
HIV drug resistant is not the only consequence of the high mutability of HIV. The propensity for accumulation of mutant strains by the HIV enzyme-reverse transcriptase-also partly explains the high genetic diversity of the virus. As at 2020, HIV-1 has four groups (M, N, O, and P), M has subtypes A–D, F–H, J, and K. Ninety-eight combination recombinant forms and many unique recombinant forms. 21,22 HIV subtype B is the major subtype circulating in the western region, whereas sub-Saharan Africa, especially West Africa, has the highest diversity of circulating HIV strains. Nigeria has one of the highest diversity of circulating HIV strains, which includes CRF02_AG, Subtypes G, A, K, and Recombinant GD. 23 Certain HIV strains have previously been associated with drug resistance, 24 –26 although scanty data exist for strains circulating in the African region especially as it relates to children. Therefore, the aim of this study is to determine the prevalence of HIV drug resistance among treatment-naive children.
Methods
This cross-sectional study was conducted at the children's HIV clinic in the University College Hospital and Adeoyo Maternity Teaching Hospital Ibadan, Nigeria, between June and December 2016. HIV positive children <15 years old were recruited at the centers. As at the time of this study, 66 children were being followed up in the clinics, out of which 46 were already on treatment. Demographic and virological information of the 66 children was gotten from the case records is shown in Table 1. HIV-1 genetic diversity and drug resistance profiles of the antiretroviral naive children (n = 20) were investigated in this study. These treatment-naive children were never exposed to ART at any point in time.
Clinical Details of HIV Cohort
ART, antiretroviral therapy; CI, confidence interval; SD, standard deviation; WHO, World Health Organization.
Ethical approval was obtained from the University of Ibadan/University College Hospital Ethics Review Committee (UI/EC/16/0084). Demographic data were collected from each participant after counseling and obtaining their informed consent to participate in the study using a structured questionnaire. Each patient was sampled 5 mL of venous blood into well-labeled ethylenediamine tetraacetic acid (EDTA) bottles and transferred in a cold chain to the laboratory. Other information such as viral load and history of ART use were obtained from the patient's hospital records.
Laboratory procedure
Blood specimens were obtained and transported to the laboratory in a cold box within 6 h of collection. Plasma was removed after centrifugation at 1,500 × g for 15 min and stored at −80°C until analyzed. HIV RNA in the plasma sample was extracted using Jena Bioscience total RNA purification kit according to the manufacturer's instructions. Complementary DNA (cDNA) synthesis was then carried out using Jena Bioscience SCRIPT one-step reverse transcriptase polymerase chain reaction (RT-PCR) kit. A nested PCR reaction was carried out for the amplification of the cDNA product with an Applied BiosystemVeriti™ 9700 Thermal Cycler with the appropriate cycling conditions. Primers used were RT21 (CTGTATTTCTGCTAT-TAAGTCTTTTGATGGG; HXB2 3,509–3,539), MAW 26 (TTggAAATgTggAAAggAAggAC; HXB2 2,027–2,050), PRO-1 (CAgAgCCAACAgCCCCACCA; HXB2 2,147–2,166), and RT20 (CTgCCAgTTCTAgCTCTgCTTC; HXB2 3,441–3,462). The nested PCR products were purified and sequenced using the Big Dye Terminator kit and a set of four bidirectional primers. The primers used for DNA sequencing were PRO-1, RT-20, RT-A (gTTgACTCAgATT-ggTTgCAC; HXB2 2,519–2,539), and RT-B (CCTAg-TATAAACAATgAgACAC; HXB2 2,946–2,967). Sequences were assembled using CLC Main Workbench Version 7.6.2 QIAGEN Aarhus A/S
Statistical analysis
Data analysis was performed using SPSS for Windows 18.0 (IBM-SPSS Inc., IL). Demographic, clinical, and virological and immunological data were stratified based on ART exposure were analyzed with t-test, analysis of variance, and Fisher's exact test (significant level was set at 0.05). Phylogenetic and similarity index analysis of aligned sequences were constructed using ggplot2 package in R. 27
Results
Baseline characteristics and HIV-1 genotyping of study participants
Demographic and virological information of the cohort from which the participants were recruited is as shown in Table 1. HIV-1 pol gene was detected in 12 of the 20 samples of the pretreatment samples and sequenced. Figure 1 shows the phylogenetic tree of the aligned sequences. Sequences gotten from samples in this study are highlighted in yellow. As shown in Figure 1, samples collected in this study clustered with previously identified reference sequences for G, CRF 02AG and Recombinant of 02_AG/G. the similarity index plot (Fig. 2) shows a high diversity of the aligned sequences. Using the REGA subtyping tool, HIV-1 subtypes G, CRF 02AG, Recombinant of 02_AG/G, and Recombinant of 02_AG/A1 were the subtypes gotten from sequences amplified from the study as shown in Figure 3.

Phylogenetic tree of the pol gene of HIV-1. Reference sequences are shown with their accession numbers. Sequences obtained from samples in this study are in grey highlights. Subtypes A1, G, CRF02_AG, and other recombinants were identified as shown. Grey dots represent unassigned sequences. Multiple sequence alignment and phylogenetic tree were constructed using ggtree package in R (64).

Similarity index plot of aligned sequences.
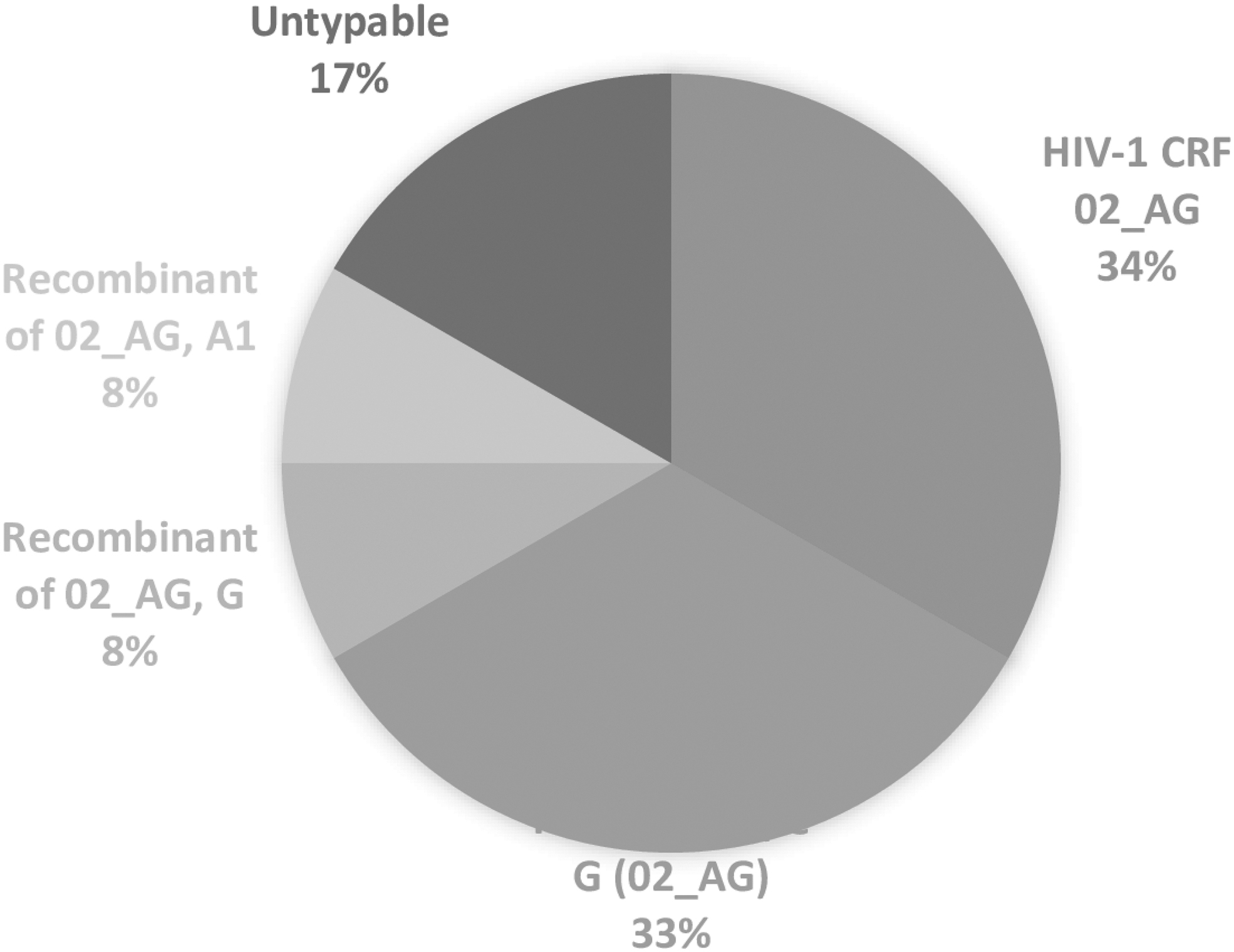
Pie chart showing the HIV-1 subtypes among antiretroviral naive children in Ibadan, Nigeria.
Drug resistance profiling
Table 2 shows the distribution of the surveillance drug resistance mutation points, and susceptible drugs across the sequenced samples. Non-nucleoside reverse transcriptase inhibitors (NNRTI) (K103N, three samples) and nucleoside reverse transcriptase inhibitors (NRTI) (M184V, one sample) were detected. Mutation K103N has previously been shown to confer resistance on nevirapine and efavirenz, whereas M184V mutation confers resistance on lamivudine, emtricitabine, and abacavir. CRF 02AG strain had the highest number of mutations detected.
Distribution of Drug Resistance Patterns Among Study Participants by HIV-1 Subtypes
3TC, lamivudine; ABC, abacavir; EFV, efavirenz; FTC, emtricitabine; NA, not applicable; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NVP, nevirapine; PI, protease inhibitor; SDRM, surveillance drug resistance mutations.
Discussion
Our study described pretreatment antiretroviral drug resistance, which is a major drawback of the PMTCT program in most developing countries. We identified HIV-1 subtypes G, CRF 02AG, Recombinant of 02_AG/G, and Recombinant of 02_AG/A1 among the samples analyzed. Furthermore, K103N (NNRTI) and M184V (NRTI) mutations were detected. From the cohort, ART-naive children were younger. This may be due to the fact that a vast majority of HIV-1 positive children are infected in the first 2 years of life. HIV-exposed children are tested at 6–8 weeks of age and 12 weeks after cessation of breastfeeding so children in the PMTCT program are detected early. 10 Also, Nigeria currently follows the option of test and treat. So infected children with known status are commenced on treatment immediately they are discovered to be positive. About 50% of the children were stunted (low height for age z scores) and underweight (low weight for age z scores). This is consistent with findings of a high incidence of both stunting, wasting, and underweight among HIV-infected children. 7,9,28 –30
ART-experienced children in the cohort had higher CD4 count as ART initiation leads to CD4 cell count recovery and immune reconstitution. 9,31 Studies have shown that commencing ART at a younger age leads to an accelerated and long-lasting CD4 recovery, and a long-term immune reconstitution. This is important in the management of HIV-infected children as they require lifelong treatment. 31 –34 Naive children had a poor clinical outcome as observed by WHO staging (34% in stages 3 and 4) low CD4+ counts and high HIV-1 RNA viral loads. This is due to the prolonged time interval between infection with HIV and enrolment into the study among naive children as >90% of them would have been infected from infancy through MTCT. 3,35 Exposure and compliance to therapy significantly improves the clinical outcome and physical state of ART-experienced children. Early HIV detection and initiation of ART are, therefore, very crucial in the care of children living with HIV. 36 –38
Identification of subtype G, CRF 02AG, and two different recombinants in this study attest to the highly diverse nature of circulating HIV-1 strains in Nigeria. 23,39 –41 Although there were slight discrepancies between the subtypes gotten using REGA subtyping tool compared with phylogenetic analysis, this might not be unconnected with use of pol gene for subtyping. The pol gene is a highly variable region in the HIV genome. Resolution of genotypes were done using the phylogenetic analysis. As shown in the similarity index plot (Fig. 2), there are highly diverse strains in the aligned sequences. This is in tandem with previous studies as Nigeria has one of the highest HIV-1 diversity globally. 40,42 HIV-1 genetic diversity have been shown to impact diagnosis, pathogenesis, and ART treatment response. 40,43 –45 The occurrence of different HIV-1 recombinants in ART-naive children of this study is of grave concern. There is an urgent need to implement PDR testing among HIV-exposed children especially in regions such as Nigeria where diverse HIV-1 strains circulate. 41,42
The high prevalence of TDR found is in tandem with the trend of rising levels of HIV-1 TDR mutations in sub-Saharan Africa. 46 It has been reported that the risk of TDR rises by 38% each year after ART rollout. 46,47 With increasing coverage of PMTCT in the country, the number of perinatally infected children is decreasing; this may, however, aid in the emergence of TDR HIV-1 strains as majority of the mothers of ART-naive HIV-1-infected children were recently diagnosed with HIV and were ART naive. The most common mutations observed in this study were K103N, which confers resistance to NNRTI drugs efavirenz and nevirapine, and M184V, which confers resistance to NRTI drugs lamivudine, emtricitabine, and abacavir but delays resistance to zidovudine and stavudine. 20 These mutations were similar to what had been observed in other studies carried out in sub-Saharan Africa, including Nigeria. 47 –51 These mutations lead to poor treatment outcomes for children on NNRTI-based ART. PDR is a very important predictor for treatment failure and results in further accumulation of drug-resistant mutations. 18,19,47,52
Despite its increasing frequency, there are few published guidelines for treating patients with TDR HIV-1 strains (TDR). Multiple studies indicate that boosted PIs are highly effective for initial treatment for patients with isolated NNRTI resistance. 38,53 –57 In patients with transmitted NRTI resistance, the selection of first-line therapy should be based on the extent of NRTI resistance. 41 Owing to historically lower levels of TDR in low- and middle-income countries (LMICs) and cost-effectiveness considerations, individual-level baseline standard genotypic drug resistance testing is not recommended by the WHO in LMICs. However, population-level HIVDR surveillance programs are strongly recommended as they play a key role in tracking TDR trends and in shaping first-line ART regimen recommendations. 14,58 The fact that CRF 02AG is the most prevalent among the resistant strains emphasizes the circulatory and transmissibility predominance of the strain in the West Africa epicenter. 23,59
The limitation of this study is the small sample size; however, it should be noted that it is difficult to recruit treatment-naive children because of the test and treat policy and zero tolerance to MTCT of HIV in Nigeria.
Conclusion
Despite the numerous benefits that rapid ART scale-up has had on AIDS-related morbidity and mortality, the potential for emergence and transmission of HIV drug resistant (HIVDR) has been a major concern of public health experts. 14 This study reiterates this challenge and has shown the presence of TDR HIV-1 strains among infected children in Ibadan, Nigeria.
Footnotes
Authors' Contributions
F.I.O., R.O., and C.O.F. conceptualized and designed the study. F.I.O. preformed the experiments. F.I.O. and B.A.O. analyzed and interpreted the data as well as wrote the first draft of the article. C.O.F. and R.O. supervised the study and reviewed the article. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank the children who participated in this study and their caregivers who gave the permission for them to participate. We also thank Miss. Grace Egunyomi, Mrs. Iyabode Abdulsalam, Mrs. Bolatito Akinyele, and Mrs. Gbemisola for their assistance in the recruitment, sample collection, and getting the records of the study participants.
Ethics Statement
The studies involving human participants were reviewed and approved. This research was conducted in accordance with the declaration of Helsinki. Experiments were conducted with the understanding and the consent of each participant. Ethical approvals for this research were obtained from the University of Ibadan/University College Hospital (UI/UCH) Research and Ethics Committee (UI/EC/16/0084). All results were delinked from patient identifiers and anonymized. The patients/participants provided their written informed consent to participate in this study.
Sequence Data/Accession Number(s)
Sequences have been deposited in GenBank Sequence Database under the following accession numbers MT036498–MT036509.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. All authors declare no conflicting financial interest.
Funding Information
No funding was received for this article.