
Abstract
In 2016, the World Health Organization developed a plan for viral hepatitis elimination by 2030. Globally, control of hepatitis B virus (HBV) and hepatitis C virus (HCV) are the most challenging aspects of viral hepatitis elimination. In many developed countries elimination of HBV could be targeted to special populations mostly immigrants from low resource settings. Elimination of HCV, however, remains a challenge globally. Barriers to HCV elimination include high cost of medications and the ability to engage specific at-risk populations as well as individuals who are out of medical care. In the context of the coronavirus disease 2019 (COVID-19) pandemic, treatment access and screening have been further negatively impacted by social distancing rules and COVID-19-related anxieties. This threatens to throw most countries off course in their elimination efforts. Before the pandemic, some states in the United States had scaled up their elimination efforts with plans to ramp up testing and treatment using Netflix-like payment models for HCV direct acting antiviral drugs. Most of these efforts have stalled on account of the health system's focus on COVID-19 control. To prevent further delays in achieving elimination targets, programs would need to explore new models of care that address COVID-19-related access hurdles. Systems that leverage technologies such as telemedicine and self-testing could help maintain treatment levels. Mathematical models estimate that COVID-19-related delays in 2020 could lead to 44,800 hepatocellular cancers and 72,300 liver-related deaths for the next decade.
Introduction
In 2016,
Current Status and Efforts at Elimination
In the current DAA era, many are working to push the HCV elimination agenda. A recent report by Gamkrelidze et al. 8 revealed that only 18 countries were on track to meet their elimination targets by 2050. Among these, 11 countries Australia, Canada, France, Germany, Iceland, Italy, Japan, Spain, Sweden, Switzerland, and the United Kingdom were on track to eliminate HCV by 2030 based on 2019 data. The United States was projected to achieve elimination sometime after 2050. To advance this imperative and in recognition of changes in HCV epidemiology the CDC now recommends screening of all adults >18 years at least once in their lifetime and annual screening for at risk individuals. 9
Further elimination efforts include encouraging the use of simplified treatment algorithms with new laboratory orders available both through Quest Diagnostics and Laboratory Corporation of America (the two major commercial laboratory companies in the United States) for HCV antibody testing with reflex HCV RNA. This allows diagnosis of active HCV infection to be achieved with one laboratory order and blood draw. The American Association for the Study of Liver Diseases has developed simplified guidelines to assist generalists in managing HCV in their patients to assist in ramping up therapy. Currently for treatment-naive HCV patients without decompensated cirrhosis, pretreatment evaluations no longer require determination of HCV genotype or resistance-associated strains testing. Such patients can be treated using any one of the two available pangenotypic DAAs sofosbuvir/velpatasvir or glecaprevir/pibrentasvir. 10 Only common routine laboratory tests such as complete blood counts and platelets, comprehensive metabolic panel, coagulation profile, and of course HCV RNA levels to confirm active disease are required before treatment initiation. Physicians and other prescribers would, however, need to confirm such patients do not have advanced cirrhosis using the Child–Pugh score and the Fibrosis-4 (FIB-4) index for liver fibrosis, which can both be easily determined using web-based and smart phone applications. This strategy was recently tested in an international patient population in the MINMON Study; conducted by the AIDS Clinical Trials Group and was shown to be safe and effective. 11 Additional simplification features include, no on treatment clinic visits and laboratory monitoring, making this strategy easily scalable in even resource-constrained settings.
In the United States, efforts at reducing the cost of HCV treatment by using special Netflix-like subscription payment models initiated by the Veterans Administration and later by States such as Washington State and Louisiana is addressing the cost barrier. 12 The use of subscription payment contracts with pharmaceutical companies provides health care plans and states with the ability to treat as many affected patients as they can over a given time at a fixed cost. These efforts have become very relevant to U.S. state Medicaid programs since Medicaid covers more HCV positive enrollees when compared with private insurance. 13 The National Governors Association identified the use of subscription payment model as one possible solution to the ever-increasing cost of drugs as a percentage of the state Medicaid expenditure. 14 Before 2020 many states started ramping up testing and treatment using different medication payment models.
Barriers and Challenges Related to Coronavirus Disease 2019
Efforts by states such as Washington and Louisiana to eliminate barriers related to costs using subscription payments and improve access to treatment were expected to make significant impact on disease burdens. Unfortunately, these efforts may be negatively impacted by the coronavirus disease 2019 (COVID-19) pandemic. Social distancing and focusing of the health system on COVID-19 control is, however, adding additional challenges to HCV elimination.
A recent survey by the World Hepatitis Alliance revealed that HCV treatment programs are experiencing barriers to medication access secondary to COVID-19. Survey respondents identified avoidance of health facilities on account of fear of COVID-19, refocusing of services toward pandemic control, travel restrictions, closure of health care facilities and drug shortages as some of the leading causes of poor access to medications. 15 Another consequence of the COVID-19 pandemic is the disruption of available harm reduction services in many communities which could worsen risk of HCV and other blood-borne pathogens. A recent report by the Overdose Detection Mapping Application Program of the University of Baltimore reported a 42% increase in reports of overdoses in May 2020 compared with 2019 numbers. This report also revealed a 17.6% increase in suspected overdose deaths since social distancing and stay-at-home orders were implemented in March 2020. 16
There are currently no reliable estimates on the impact of COVID-19 on viral hepatitis programs in the United States, but the National Alliance for State and Territorial AIDS Directors information suggests that >90% of providers anticipate a decrease in outreach, testing, and linkage services. 17 With most infectious disease providers involved with the COVID-19 control efforts to varying extents the impact of COVID-19 on HCV infection and diagnosis rates will be difficult to quantify. The World Hepatitis Alliance survey suggested that screening rates may be reduced. 15 On this account we can assume that any gains made in HCV elimination efforts may be reversed or at best stalled by the pandemic. This concern has been raised by many providers in the field. 18,19 Treatment delays for vulnerable patients with HCV has potential to lead to further disease progression and development of fibrosis. These delays could lead to both poorer health status and increases in the cost of care for individual patients affected. The global impact will be seen in delays in achieving set targets as well as increased overall system costs. Mathematical models assuming a 1-year delay in HCV elimination programs secondary to COVID-19 predicted 44,800 excess hepatocellular cancers and 72,300 excess liver-related deaths globally for the next 10 years. This delay scenario is also expected to lead to 746,000 missed treatments. Most of these missed treatments are expected to be in World back Income-designated high- and middle-income countries with <3% from low-income countries. 20 Thus, the cost in quality of life and the excess morbidity and mortality due to these delays cannot be overemphasized.
Solutions and the Path Forward
To reduce these negative impacts, all health systems and providers need to be cognizant that social distancing rules and other COVID-19 precautions could exacerbate high-risk behaviors. State, federal, and other municipalities across the globe should acknowledge the scientific data on COVID-19 and develop and enforce public health efforts to contain and control the pandemic. Within this climate viral hepatitis and other health programs should proactively develop solutions to resume and maintain appropriate health services during the pandemic. Alternate service delivery models that prioritize continuity of care without increased face-to-face contacts must be explored. Any such adopted service models would require active evaluation to determine effectiveness and participant acceptability. Programs, systems, and providers can modify some of the suggestions provided in Table 1 for COVID-19-related barriers to elimination. Service organizations and program funders need to remain cognizant of ongoing issues within their relevant target populations and quickly adapt programs to rapidly changing situations. Programs must maintain active communication with their clients to help identify potential gap areas and develop interventions to address these gaps.
Potential Solutions to Pandemic-Related Barriers to Hepatitis C Virus Elimination
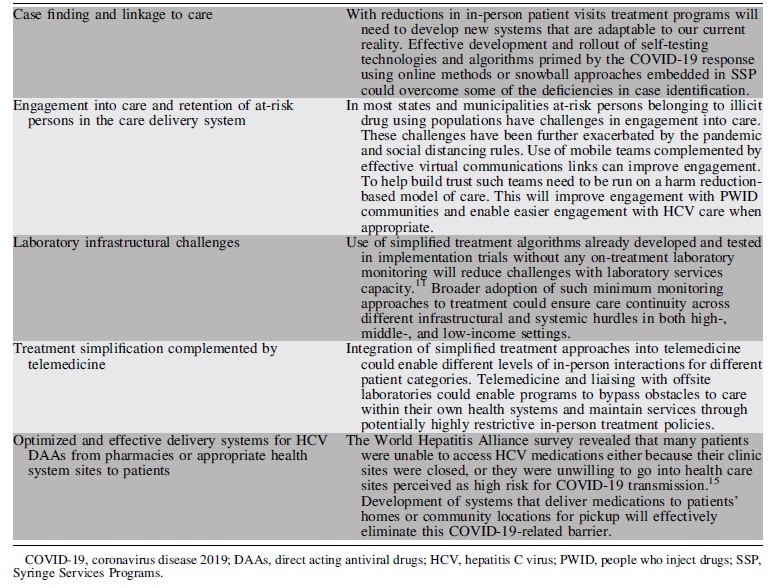
In these times of social distancing interventions such as home self-testing for HCV/HBV and HIV could be considered with appropriate regulatory controls. In the absence of such services many states, and municipalities would experience significant short falls in gains made in the past few years. This would further delay efforts at meeting the 2030 HCV elimination targets.
The current laser focus on COVID-19 while expedient would need to be done while remaining cognizant of potential unintended consequences of the pandemic response. Providers and programs in HCV care delivery must stay abreast with the impact of the COVID-19 pandemic on HCV risk groups. All stakeholders involved in HCV care must consider service modification to reduce the negative impact of COVID-19 on HCV elimination efforts.
Footnotes
Acknowledgments
We thank colleagues and family who were instrumental in helping with the development of this article. We would like to specifically mention Dr. Beverly Alston-Smith of the Division of AIDS who provided advice on content and my spouse Dr. Aisha Yansaneh of United States Agency for International Development (USAID) who provided editorial assistance.
Authorship Confirmation Statement
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the study to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in AIDS Research and Human Retroviruses.
Author Disclosure Statement
All the authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors did not receive any funding for this article.