
Abstract
Hepatitis E virus (HEV) is thought to be common in the United States with increased prevalence in those with concomitant hepatitis C virus (HCV) or HCV/HIV coinfection. Little is known regarding true prevalence, incidence, and antibody seroreversion in these populations. We sought to define these rates among HCV and HCV/HIV coinfected persons in the Washington, DC area. Two longitudinal cohorts of HCV and HCV/HIV coinfected subjects from the Washington, DC area were evaluated. Multiple HEV test modalities were deployed including immunoglobulin G (IgG) and immunoglobulin M (IgM) antibody testing, evaluation of antibody avidity, HEV RNA testing, and HEV enzyme-linked immune absorbent spot (ELISPOT) analysis. A total of 379 individuals were evaluated including 196 who were HCV monoinfected and 183 HCV/HIV coinfected. Anti-HEV IgG was detected and confirmed in 18.7% of the cohort at baseline. None demonstrated anti-HEV IgM positive or HEV RNA positive results. Proportions of HEV antibody prevalence did not significantly differ between groups. Longitudinal follow-up samples were available for 226 individuals with a mean follow-up time of 24 months. Seroreversion was noted in 1.8%. One HCV/HIV infected person seroconverted to HEV IgG positivity in the followed cohort. About 40% of the positive population demonstrated high avidity suggestive of more remote exposure. Interferon gamma ELISPOT was performed in 70 subjects and false negative and false positive HEV enzyme-linked immunosorbent assay antibodies were identified. In HIV-infected persons in the United States HEV exposure and seroconversion is frequent enough that HEV should be considered in the differential diagnosis of acute hepatitis. Seroreversion may lead to underestimation of true infection risk.
Introduction
The hepatitis E virus (HEV) is a hepatotropic virus in the family Hepeviridae. It is mainly transmitted through fecal-oral contact in much of the developing world, with the majority of endemic and epidemic disease spread through contaminated water. Various genotypes of the virus appear to demonstrate some degree of host preference but not host specificity. In places where sanitation is better, zoonotic forms of the virus appear to predominate, with man serving as a terminal or near-terminal host. In these areas, including the United States and Europe, infection appears to be associated with consumption of swine products, though other animals (e.g., deer, rabbits) may also transmit the virus. 1 Human to human transmission occurs with a low frequency after receipt of blood and blood products donated by infected individuals, 2,3 and sexual transmission is suspected but not confirmed. 4
In the United States, serosurveys conducted by the CDC through the NHANES datasets suggest relatively high rates of population exposure with peak prevalence in the Midwestern United States. 5 It appears that overall prevalence (as evidenced by antibody detection) is declining. Some studies have suggested higher rates of infection in those with chronic hepatitis C virus (HCV) infection. 5 Higher rates among persons living with HIV infection have also been described including those with end-stage liver disease and end-stage renal disease. 6 –8 However, other HIV-infected cohorts did not yield high rates of acute or chronic HEV infection. 9 The reason for this discrepancy is not clear, but it is suspected that standard methodologies for detection of previous exposure to HEV infection, especially in HIV or HCV/HIV co-infected subjects, may be unreliable leading to incorrect attribution or exclusion of disease.
Therefore, we sought to define the prevalence, incidence, seroreversion rates, and false negative/positive rates of HEV infection among HCV and HCV/HIV coinfected persons in the metropolitan Washington, DC/Baltimore area using two alternative methods to characterize humoral (enzyme-linked immunosorbent assay [ELISA]) and cellular immune responses (enzyme-linked immune absorbent spot [ELISPOT]) to HEV.
Materials and Methods
Study cohort
Under the auspices of the U.S. National Institutes of Health, two longitudinal cohorts were developed and linked to characterize viral liver disease and factors affecting the natural history of patients with HCV/HIV coinfection or HCV alone in the Washington, DC metropolitan area. The cohorts were designed to study research questions with respect to liver disease, disease pathogenesis using genomics, proteomics, and immunologic disease models. They consisted of chronic HCV monoinfected and HCV/HIV coinfected subjects seeking care at clinical facilities in the District of Columbia and surrounding environs in Maryland. HCV chronicity was defined as HCV RNA present for more than 6 months. All subjects enrolled in the DC cohort eventually were treated, primarily in the context of clinical trials or standard of care for HCV.
Samples were collected between 2009 and 2017. Serum/plasma and peripheral blood mononuclear cells (PBMCs) were collected at baseline enrollment and approximately every 6 months thereafter. Samples were collected, separated, and stored in a manner compatible with viral RNA preservation. All available longitudinal samples were evaluated. Demographic data and relevant clinical lab data were collected. Information regarding HEV exposure risk (men who have sex with men, drug use, overseas travel, or farm animal exposure) and specific ART treatment was not available. All subjects provided informed consent and the protocol was approved by the Institutional Review Boards associated with the collection sites. Testing was performed on deidentified samples.
Serologic methods
HEV immunoglobulin G (IgG) was evaluated in all available samples, and HEV immunoglobulin M (IgM) in the IgG positive samples, using sensitive diagnostic ELISA assays (Wantai Biological Pharmacy Enterprise, Beijing, China). The assays were performed according to the manufacturer's recommendations including retesting/confirmation of all positive results. Manufacturer-reported specificities for the IgG and IgM assays were greater than 99.93% and 95.3%–100.0% respectively. Reported sensitivity of the IgM ELISA was 100% for the first serum sample, and 97.62% for serial samples. This assay is highly sensitive and specific in comparison to other commercially available tests. 10
Secondary testing of selected samples was performed when ELISPOT assays suggested discordance between Wantai serologic results and interferon gamma (IFN-γ) response to HEV antigens. The Mikrogen Diagnostik (Neuried, Germany) assay was performed in duplicate according to the manufacturer's recommendations. Manufacturer-reported specificity and sensitivity for the IgG assay were 98.5% and 98.9%.
HEV avidity testing was performed on paired samples of IgG+ sera as described. 11,12 Briefly, one serum sample was tested by the standard ELISA method and the second was exposed to 5M urea as a chaotropic reagent to interrupt the interaction of low-avidity antibodies with antigens. Optical density (OD) of the pairs was measured and avidity calculated as OD urea-treated sample × 100/OD untreated sample. Samples with avidity of <50 were classified as low avidity and those >50 as high avidity.
HEV ELISPOT was used to evaluate T cell immune responsiveness to HEV ORF2 Recombinant; Protein ORF2; pORF2 HEV ORF2 (452–617 a.a.) (Cat. No. GWB-C95428; Genway Biotech, Inc., San Diego, CA, USA). ORF2 is the most immunogenic HEV protein as described. 13 ELISPOT assay was performed with the precoated human γ-IFN ELISPOT plus Kit (Cat. No. 3420-4APW-10; MABTECH, Cincinnati, OH, USA) according to the manufacturer's instructions. Briefly, the plates were washed and blocked with 10% fetal calf serum (FCS) in complete media 1 h at 37°C/5% CO2. To estimate the number of HEV-specific interferon-γ secreting cells (ISC), previously thawed PBMCs were added at concentrations of 1 × 105 cells/well in a 200-μL volume of complete medium (RPMI-1640 containing 10% FCS serum).
For stimulation, PBMCs were pulsed with the HEV ORF2 protein at 1 μg/mL, positive control (anti-CD3 at 1 μg/mL, or PHA at 1 μg/mL) and negative control (no stimulus/complete media) in duplicates. After 24-h incubation at 37°C/5% CO, the plates were washed five times with distilled water and washing buffer phosphate-buffered saline (PBS) (Sigma, St. Louis, MO, USA). Biotinylated anti-human IFN-γ monoclonal antibody (mAb) (7-B6-1-biotin) at a concentration of 1 μg/mL in dilution buffer (PBS +0.5% FCS) was added, and the plates were incubated at room temperature for 2 h. Plates were then washed again five times, and streptavidin– alkaline phosphatase (1:1,000) in dilution buffer was added and incubated at room temperature for 1 h, followed by washing five times with washing buffer and the addition of the ready to use substrate (BCIP/NBT-plus) reagent (Mabtech, Cincinnati, OH, USA).
After developing the spots for 5–30 min, the plates were washed with distilled water and air-dried. The number of spot-forming cells was enumerated using the automated ELISPOT 3B analyzer (CTL, Cleveland, OH, USA) designed to detect spots with predetermined criteria based on size, shape, and colorimetric density, and expressed per 106 cells. Results were calculated from the following equation:
We determined the cutoff level of ISC as the average number of ISC in the presence of no stimulus (medium) +2 standard deviation, and plotted HEV-specific ISC after subtracting the number of ISC induced by no stimulation. 14
Virologic methods
Viral RNA was extracted from patient plasma samples using the QIAamp Viral RNA Mini Kit according to the manufacturer's instructions, including 4 μL of an internal RNA extraction control added to the lysis buffer. The 30 μL reverse transcriptase-quantitative polymerase chain reaction (RT-qPCR) reaction mix contains modified primers and FAM-labeled probe modified from the method of Jothikumar for HEV ORF3 (forward 5′-GGT GGT TTC TGG GGT GAC-3′; reverse 5′-AGG GGT TGG TTG GAT GAA-3′; and HEV degenerate probe 5′-/56-FAM/TGA TTC YCA GCC CTT YGC/3IABkFQ/-3′ for HEV ORF2/3, and primers and TAMRA-labeled probe for the extraction control, and 10uL of RNA sample. 15 Amplification was performed on the ABI QuantStudio 3 real-time thermal cycler, with the following cycling conditions: 50° for 15 min; 95° for 2 min; and 45 cycles of 95° for 15 s, 55° for 60 s.
A synthetic quantitative HEV RNA standard was amplified with each run to generate a standard curve to determine virus concentration. Positive, negative, and no-template controls were included with each run. The assay successfully amplifies the international standard consistently to 250 IU/mL, with a 30% detection rate at 25 IU/mL. 16
Statistical analysis
Parametric and nonparametric data were analyzed as appropriate for data type using Statistix 10.0 (Analytical Software, Tallahassee, FL, USA). Two-tailed tests with a significance level of 0.05 were utilized.
Results
Overall, 379 individuals were evaluated at baseline. Of these, 196 were HCV monoinfected and 183 were HCV/HIV coinfected. The median age at baseline was 56 (range 21–82) and 76% were male. The majority (78%) were black, non-Hispanic. A higher proportion of black and male participants was observed in the coinfected subgroup. Median CD4 was 714 cells/mm3 (range 62–2,328 cells/mm3). As expected, CD4 count was lower in those with HIV (median 540 cells/mm3; range 62–1,531 cells/mm3) versus HCV monoinfected (907 cells/mm3, range 346–2,328 cells/mm3). The median serum alanine aminotransferase (ALT) level was 43 IU/mL. The baseline median HCV viral loads were 1.14 × 106 (range 0–1.37 × 108 copies/mL) and 1.43 × 106 (range 0–1.43 × 108 copies/mL) for the HCV and HCV/HIV patients, respectively. The predominant HCV genotype was 1a in both HCV and HCV/HIV groups (64.7% and 67.8% respectively.)
Among those patients with available biopsy data, 90% had no or mild fibrosis and 10% had advanced fibrosis/cirrhosis. Demographic characteristics are summarized in Table 1. HIV viral load was not correlated with HEV antibody measurement (HEV IgG OD/control).
Demographic Characteristics of Hepatitis C Virus and Hepatitis C Virus or HIV Participants
ALT, alanine transaminase; bDNA, branched DNA; HCV, hepatitis C virus.
Baseline anti-HEV IgG was detected and confirmed in 18.7% of the cohort. None of these were anti-HEV IgM positive. Though antibody positive rates were numerically higher in the HCV monoinfected group (21.4%) versus the coinfected subset (15.8%), this difference failed to reach statistical significance (p = .16). In univariate analysis, HEV IgG prevalence was not associated with sex, race, or ethnicity.
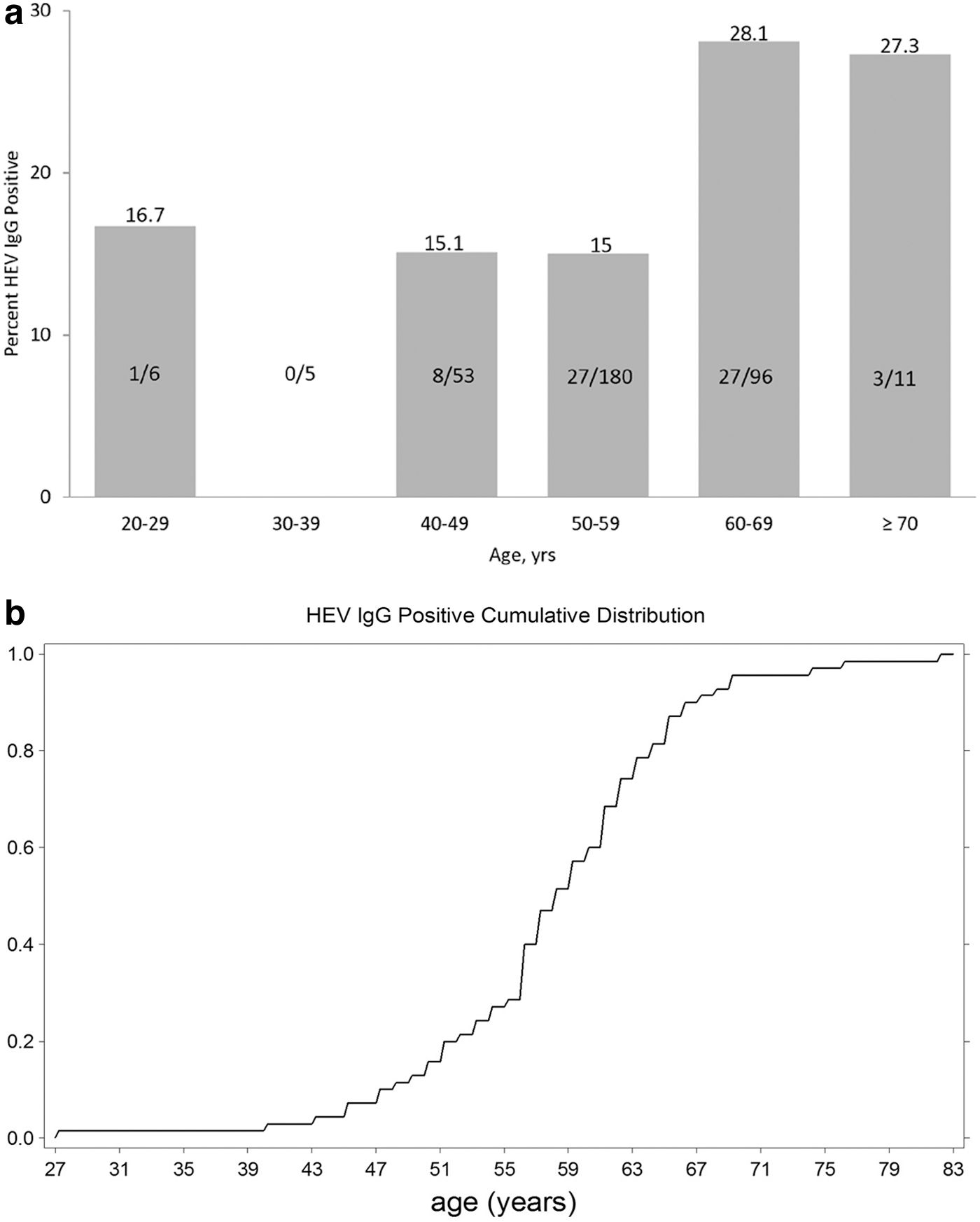
Place of birth information was collected for 126 individuals, with 94% born in the United States, however, there was no difference in HEV IgG prevalence based on birthplace. Age was a significant factor, with older (>60 years) subjects having higher prevalence than those younger (p = .0097). Older participants were not more common among those with HCV/HIV versus HCV monoinfected (27.3% vs. 33.6%; p = .18). The age-specific prevalence and the cumulative anti-HEV IgG positivity rates are graphically demonstrated in Figure 1a and b. There was a modest correlation between CD4 percent and HEV IgG OD/cutoff ratio (r = 0.32). Among the 140 subjects with biopsy scoring available, F0–3 versus F4–6 (no or mild fibrosis vs. advanced fibrosis/cirrhosis) did not correlate with positive IgG serology (p = n.s.).
Longitudinal follow-up samples were available for 226 individuals, including 92 HCV monoinfected and 134 HCV/HIV coinfected persons. The mean follow-up time was 24 months (range 6–81 months), with 221 having 1 follow-up sample, and 5 subjects having multiple timepoints. All follow-up samples were tested for HEV IgG. Overall, 98% of subjects had no change from baseline in HEV IgG serological status. However, 4/226 individuals (1.8%) experienced seroreversion (loss of anti-HEV IgG antibody), or 17.7/1,000 persons. Three seroreverters were HCV/HIV coinfected and one had HCV monoinfection. There was not an apparent association with CD4 or change in CD4 associated with seroreversion.
One subject (1/134; 0.7%) with HCV/HIV coinfection seroconverted to positive antibody at 80 months after baseline sample collection. An increased level of ALT was not noted compared to the prior sampling; however, there was a 6-year gap in samples available for testing, suggesting conversion occurred in this window between sample collections. This participant had CD4 levels over 500 cells/mm3 at all timepoints collected. Anti-HEV IgM was negative in this subject and the avidity was less than 50, suggesting more recent infection (see avidity discussion below). No subjects in the cohort demonstrated viremia, including the seroconverter participant.
The avidity of the anti-HEV antibodies was assessed in all of the baseline IgG positive subjects. The association between avidity and the IgG OD/control ratio is shown in Figure 2 (Pearson r = −0.23). Avidity did not correlate with CD4 count or CD4 percent. High avidity was found to be present in 9/71 (12.7%) baseline samples. This parameter was negatively associated with anti-HEV IgG levels as measured by the OD/control ratio (p = .007) supporting the concept that the low avidity group had either more recent HEV infection as suggested by previous studies, 12,17,18 or very old infection. The percentage of lower avidity was 100%, 75%, 83%, 93%, and 100% in the 20–29, 40–49, 50–59, 60–69, and 70+ year-old age groups, respectively.

Scatterplot of avidity versus HEV IgG OD/Control. The association between HEV avidity and the IgG OD/control ratio is shown (Pearson r = -0.23.). OD, optical density.
A randomly selected subset of HCV monoinfected (n = 27) and HCV/HIV coinfected (n = 43) individuals were evaluated by ELISPOT. For HEV-specific immune responses, there was a highly significant correlation (r = 0.6, 95% confidence interval [CI] 0.38–0.75, and p ≤ .0001) between the anti-HEV IgG S/C ratio and HEV-ORF2-specific IFN-γ secreting cells. The average anti-HEV IgG S/C ratio in HCV mono-infection was not significantly different from that in HCV/HIV coinfection (1.48 ± 3.67 and 0.55 ± 1.5, respectively, p = .14). However, there was a significant increase (p = .009) in the number of HEV-ORF2-specific IFN-γ stimulated spots/million cells in HCV monoinfection compared with HCV/HIV coinfection (Fig. 3).

HEV ELISPOT response comparing HCV to HCV/HIV coinfected subjects. There is a significant increase in HEV-ORF2-specific IFN-γ stimulated spots/million cells in HCV mono-infection compared with those with HCV/HIV coinfection (p = .009). ELISPOT, enzyme-linked immune absorbent spot; HCV, hepatitis C virus; IFN-γ, interferon gamma.
Furthermore, 11 subjects with HEV-specific ELISPOT responses greater than 55 spots had HEV IgG OD/Control ratios less than 1, indicating a negative test. Interestingly, these false-negative results were more likely to occur in HCV monoinfected (8/11; 73%) versus HCV/HIV coinfected (3/11; 27%) patients with an odds ratio of 2.7. There was no history of ribavirin treatment listed for any of the 11 false-negative IgG antibody results by ELISA. In those that tested negative by ELISPOT using the conservative cutoff of 55 spot forming units (SFU), 7 subjects tested positive for HEV IgG by ELISA. However, 5/7 had HEV antigen-specific responses of 20 SFU or greater suggesting that the ELISA was concordant with the T cell responses. The discordant cases using the more liberal definition were both HIV positive (Figs. 4–6).

Correlation between the anti-HEV IgG S/C ratio and HEV-ORF2-specific ISCs. 1 = ELISPOT positive, ELISA negative; 2 = ELISPOT negative, ELISA positive; 3 = ELISPOT and ELISA positive; 4 = ELISPOT and ELISA negative. ELISA, enzyme-linked immunosorbent assay; ISCs, IFN-γ secreting cells.
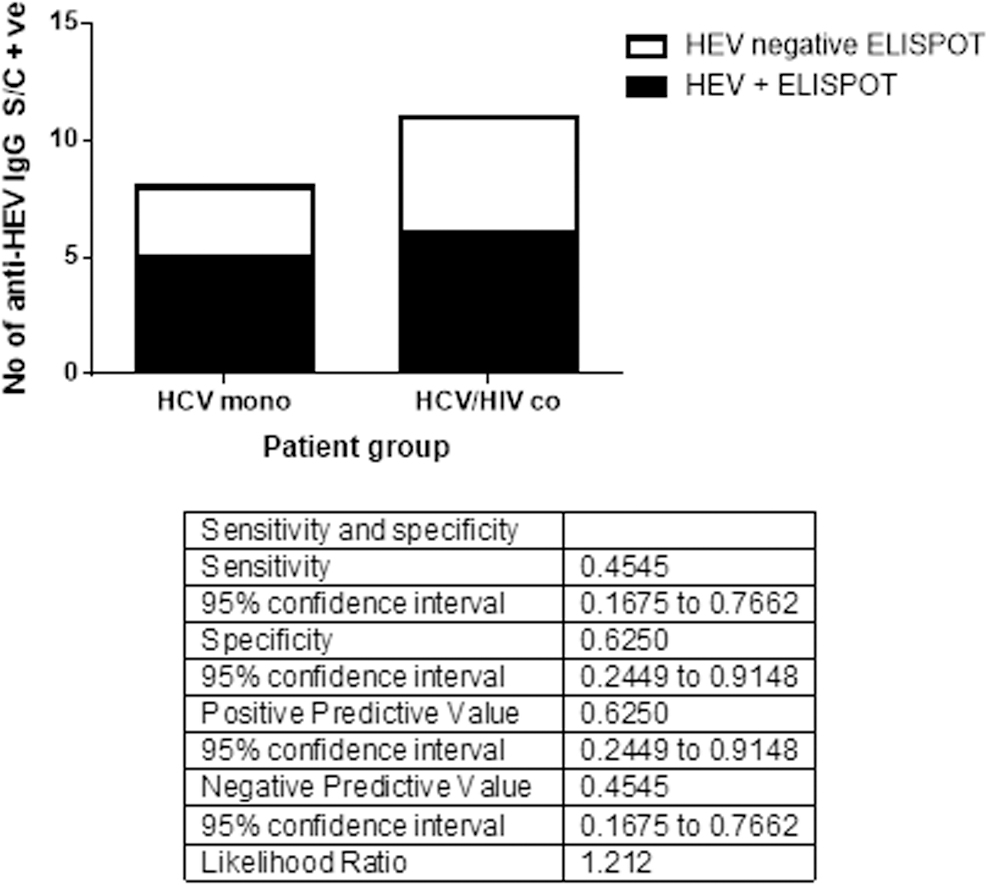
Sensitivity and specificity of HEV ELISA in comparison to ELISPOT.
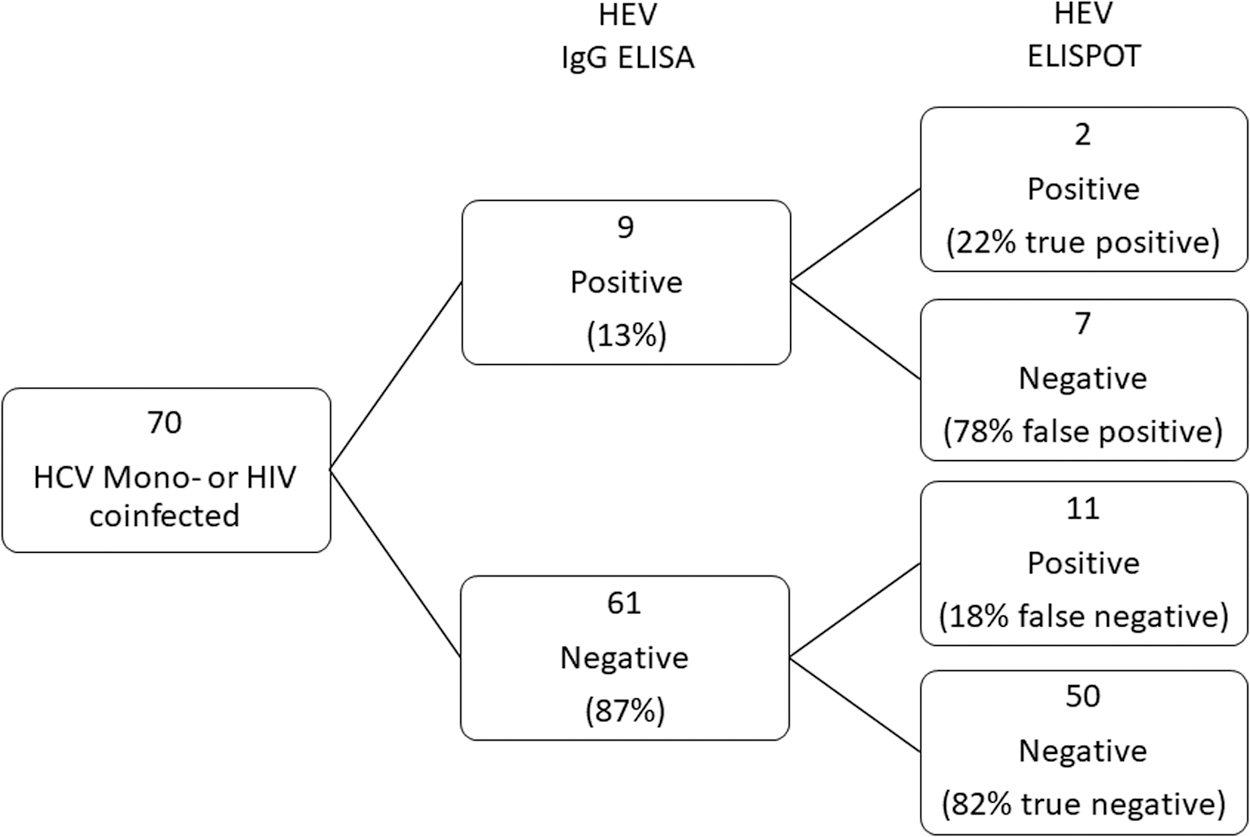
Relationship between HEV IgG ELISA results with subsequent ELISPOT results. Percentages represent ratio of ELISPOT data compared to ELISA.
Application of the Mikrogen assay did not significantly alter these findings. All subjects thought to be false negative reactions with the Wantai assay were also negative with the Mikrogen assay. Four of seven (57.1%) of the putative false positive Wantai results were also positive using the Mikrogen assay, but Mikrogen did not provide a positive result in the two subjects who had five or less SFU after antigen stimulation. There was no association with the age of the participant. Among the five subjects that changed antibody status in the longitudinal follow-up, four had baseline cell samples available for ELISPOT analysis. However, PBMCs were not available for longitudinal testing of these subjects.
HEV RNA was not detected in any sample, including those who demonstrated seroconversion.
Discussion
HEV infection is a significant worldwide disease process that is most commonly associated with development of acute hepatitis in resource-limited setting. However, a zoonotic form of the virus with man serving as a terminal or near-terminal host is increasingly recognized in more developed regions of the world. In Europe, increasing rates of HEV are being reported, associated with consumption of swine products, venison, rabbits, and other mammalian species that may harbor HEV. 19 Acute infections are particularly troublesome in immunocompromised patients because failure to clear the virus leads to a chronic inflammatory hepatitis that can rapidly progress to cirrhosis and liver failure. 20,21
In the United States, HEV serosurveys suggest that HEV was quite common in the past, as evidenced by high rates of HEV antibody among older adults and decreasing rates in younger age cohorts. In selected groups such as those with HIV or HCV, HEV rates of exposure appear to be higher in some, but not all reported cohorts. 5,6,22 This includes HIV infected persons with end-stage liver disease or end-stage renal disease. 8 This study was designed to focus on HEV infection among those with HCV, with or without concurrent HIV infection to better understand the use and limitations of current diagnostic methods. To this end, we evaluated HEV IgG reactivity and evaluated those findings in terms of antibody avidity (binding strength) and to T cell-mediated responses to HEV antigenic stimulation. We also examined HEV IgM levels and HEV viremia.
The overall rate of HEV IgG prevalence was 18.7% across the cohort with numerically higher (but not statistically significant) rates observed in those with HCV alone. Kuniholm et al. reported that presence of HCV antibody was associated with an increased odds ratio of having HEV antibody of 1.71 in the third NHANES survey. 5 As has been observed in other studies in the United States, age was a factor in antibody prevalence with older persons (>60 years) having higher rates of exposure versus younger participants.
Analysis of the most recent NHANES data suggested that age is no longer the most important factor in HEV seropositivity, as race/ethnicity (non-Hispanic Asian) was identified as having a stronger association than age. 2,23 However, the overall rate in the general population survey was 8.1% (95% CI = 6.5–9.7). In persons age 50–59 the weighted IgG positive rate was 8.9% (95% CI = 5.7–12.3) while in our 50–59-year-old group 15% were HEV IgG positive. Seroreversion of HEV IgG was observed at a rate of 8.8 per 1,000 persons per year, which is higher than the rate observed in a non-HIV infected cohort in Germany, which reported seroreversion rates of 2.9 per 1,000 persons per year. 24
Antibody avidity is thought to be a surrogate indicator for duration of infection and protection. 11,12,17 In a study of HEV-infected rhesus monkeys, animals with anti-HEV IgG antibody were re-exposed to HEV. Re-infected animals had lower HEV-IgG avidity than those who were protected from infection after re-exposure.
In a large series, Bigaillon et al. provided evidence that acute HEV (<6 months) can be separated from older infections using avidity, due to slow maturation of the IgG response. 17 In the study done by our lab for an HEV outbreak in Egypt, we found asymptomatic HEV seroconverters had significantly higher levels of epitope-specific neutralizing and high avidity anti-HEV antibodies than the corresponding cases with acute hepatitis. 12 In our cohort, 12.7% of the participants had low avidity suggesting more recent infection. Avidity was not associated with seroreversion and low avidity was observed in the seroconverter participant.
The reliability of HEV antibody tests remains a serious clinical dilemma. 25 In the setting of the immunocompromised host, this concern may be exacerbated. We utilized a unique ELISPOT assay initially developed by our laboratory to assess T cell-derived IFN-γ responses after exposure to HEV ORF-2 specific epitopes that correlated strongly and significantly with anti-HEV ELISA positive/negative results. 14 ELISPOT assay is highly sensitive compared with other methods for detection of Ag-specific T cells. 26 The specificity of the ELISPOT assay depends on the background response of the negative control and the cutoff value. In our assay we used >55 SFUs as the cutoff value for positivity. However, Alexander et al. notes that a threshold value of at least 11 SFU/106 PBMC has biological significance. 27 In the ELISPOT assay we used ORF-2, which is a recombinant protein since ORF2 is the most immunogenic protein of HEV. 13
We identified quantitative differences in T cell responses between HCV monoinfected and HCV/HIV coinfected subjects, consistent with a defective immune response in those with HIV infection. Using this assay as the “gold standard” 11 HEV ELISA negative subjects had positive ELISPOT responses suggesting under-reporting of HEV prevalence by both the Wantai assay and the Mikrogen assay. Both the manufacturer and external validation panels have suggested high sensitivity and specificity for both assays. A compilation of prior reports by Al-Sadeq et al., suggests that the Wantai assay sensitivity ranged from 72.5% to 93.2% with a specificity of 97.8%. 28 This was as good as or better than most other tested HEV IgG assays.
It is possible that the ELISPOT itself underestimates the false negative rate among coinfected individuals, since we do see an overall decrement in IFN-γ spot production in the setting of coinfection. Therefore, true rates of HEV exposure among HCV/HIV coinfected individuals may indeed be higher than reported in our study and others.
In addition, of the nine samples that tested positive by the Wantai HEV ELISA, seven of those were found to be negative by ELISPOT. Five of these 7 had HEV antigen-specific responses of 20 SFU or greater suggesting that the other two were below the sensitivity of the ELISA assay. Four of the false positives were also negative by the Mikrogen assay. False positive reactions may occur due to nonspecific binding of immunoglobulin and also reflect the trade-off of sensitivity versus specificity that is selected by the test manufacturer. In terms of the ELISPOT assay, the cutoff for positive was selected for high specificity and less stringent criteria may lead to greater concordance with the ELISA results.
The absence of detectable virus RNA in the HIV-infected population is not surprising due to the low and short levels of viremia in HEV infection. Prior reports from the Women's Interagency HIV Study (WIHS) and Multicenter AIDS Cohort Study (MACS) cohorts identified only one case of chronic HEV among 2,919 plasma samples derived from HIV-infected persons. 9 Overall rates of prior exposure appear to be highly variable by country and within regions of countries. In a summary by Debes et al., ranges of HEV IgG in more than 25 studies of HIV-infected persons was noted. At the low end, some cohorts reported rates of 1%–2% and at the high end, prevalence rates of over 45% were observed. 29 The question is whether these rates reflect local risk exposures from consumption of swine products or other sources, or do they represent increased risk from other sources (e.g., MSM sexual contact or injection drug use).
Since HEV diagnostic testing is not routinely available in the United States at this time, the disease remains largely unrecognized as a potential cause of acute (if not chronic) infection among those with HIV. With prevalence rates approaching 20% it is likely that HEV is a relatively common source of acute elevations of liver enzymes, and that it should be considered in the diagnosis of clinical and subclinical hepatitis when testing discloses serum transaminase abnormalities. It is likely that a small proportion of cases will result in chronic infection, though we failed to identify such infections in our cohort. However, our power to do so was low if the true rate of chronicity is ∼1 in 1,000 as suggested in the analysis of the WIHS/MACS cohorts. 9 Though chronicity occurs in the setting of HIV infection, rates of chronicity appear to be much higher among solid organ transplant recipients, exceeding 65% of acute infections. 30 Since treatment with ribavirin is effective in a high proportion of patients with chronic HEV, consideration of HEV as an etiology of liver disease in all immunocompromised persons appears warranted. 31
In summary, HEV infection with resolution appears to be a relatively frequent occurrence among persons infected with HCV and HCV/HIV coinfection. Seroconversion and seroreversion occur, and the latter observation complicates epidemiologic analyses. ELISPOT may be an important tool to identify HEV antibody negative infections, but its application may have limitations in those with HIV due to decreased IFN-γ responses to stimulation of T cells by HEV specific epitopes. In HIV-infected persons in the United States HEV chronicity appears to be uncommon, but HEV exposure, as highlighted by prevalence data, is frequent enough that HEV should be considered in the differential diagnosis of acute hepatitis.
Footnotes
Authors' Contributions
K.E.S.: study concept and design; obtained funding; analysis and interpretation of data; statistical analysis; drafting of the article; critical revision of the article; study supervision; S.K.: site PI, study concept and design; obtained funding; analysis and interpretation of data; statistical analysis; critical revision of the article; study supervision; S.D.R.: acquisition of data; analysis and interpretation of data; critical revision of the article; technical and administrative support; E.A.A.-h.: acquisition of data; analysis and interpretation of data; critical revision of the article; C.L.B., H.L.M., and M.T.S.: acquisition of data; analysis and interpretation of data; critical revision of the article; N.T.: site PI; study concept and design; analysis and interpretation of data; critical revision of the article. All authors read and approved the final article.
Author Disclosure Statement
All authors report no conflicting financial arrangements relevant to this article. Unrelated disclosures include: K.E.S.: Grants/Contracts (paid to institution) from AbbVie, Gilead, Merck, Intercept; Advisory Board/Consulting from Uniqure, and Data Safety Board from Watermark, and MedPace. S.K.: Grants and other funding from Gilead Sciences, grants from Merck, Inc., and American Gene Technology. N.T.: Institutional grant support from Gilead Sciences; advisory board Intercept. S.D.R., E.A.A.-h., C.L.B., H.L.M., and M.T.S.: nothing to disclose.
Funding Information
This work supported in part by a grant from NIH NIDDK (1R01 DK108362) to K.E.S.