
Abstract
As of January 12, 2021, Australia has reported 28,634 COVID-19 cases. Most (20,411) cases are from the state of Victoria. In response to rising infections and community transmission in July 2020, on August 2nd, several restrictions were imposed for the following 111 days, including an 8pm curfew, a travel restriction to 5 km from home, and closure of nonessential services. It is unknown how this affected people living with HIV (PLHIV), who already experience disproportionate levels of mental health issues, comorbidity, and stigma. An online survey was designed with HIV community-based organizations to investigate the impact of the pandemic on Victorian PLHIV. Participants were recruited voluntarily both through social media and Infectious Diseases clinics at participating hospitals. There were 153 respondents. Most were male (77%), aged between 30 and 60 years (77%), and Australian-born (63%). Forty-three percent, 31%, and 25% reported negative impacts upon personal relationships, employment, and income, respectively. HIV care continued with 95% and 98% being able to access their HIV provider and antiretroviral therapy (ART), respectively. Telehealth was used by 92% and was largely well received. PLHIV reported worry about physical health (68%), mental health (66%), finances (50%),z and accommodation (25%). Fifty percent of participants reported weight gain and 27% increased alcohol intake. This study demonstrated the widespread negative effects of the COVID-19 pandemic on PLHIV in Victoria, although provision of HIV care and ART continued uninterrupted. This highlighted the importance of mental health support and social welfare programs during times of health care and societal strain.
Introduction
The COVID-19
In response to the rising mortality and community transmission during this second wave community restrictions were enforced. The strictest of these, labeled “Stage 4 Restrictions,” began on August 2nd and lasted 111 consecutive days. They included a nightly 8pm to 5am curfew, travel restricted to 5 km from home, and closure of all nonessential services. 8 The state border was closed and Victorians were able to leave home only for exercise (1 h/day), buying essential goods, care or care giving, and work or school if it could not be done from home. 8 Outpatient medical care transitioned to telehealth, and elective surgery was postponed or canceled.
The effect this had upon PLHIV, a group that experiences higher than average levels of mental health issues, comorbidity, and stigma than the general population 9 was unknown. This study was conducted to examine the impacts of the COVID-19 pandemic and the associated restrictions upon PLHIV in Victoria, Australia.
Materials and Methods
An online survey was designed in collaboration with community-based organizations representing key HIV advocacy groups in Australia to investigate the impact of the COVID-19 pandemic on PLHIV in Victoria, Australia. Questions were focused on demographics (age, gender, country of birth, and postcode), causes of concern, and impacts (positive, negative, or none) of the pandemic in the following domains: income, employment, accommodation, personal relationships, and access to food. The definition of what constituted a personal relationship was left open to allow for the consideration of the impact of the COVID-19 pandemic on all types of close relationships for PLHIV, including but not limited to relationships with family members, friends, romantic partners, and sexual relationships. Participants were also asked about the changes in their food intake, weight, and substance use, as well as their ability to access HIV-specific care and other medical services. Study data were collected and managed using REDCap®, 10 a secure online survey platform, hosted at Alfred Health. The full list of survey questions is listed in the Supplementary Appendix SA1.
The study protocol received ethics approval by the Alfred Health Human Research Ethics Committee (ref: 65769). Participants were recruited through social media advertising and through the Alfred Health and Monash Health Infectious Diseases clinics. Alfred Health is the state-wide HIV referral center for Victoria and along with Monash Health has a high volume of HIV clinics, which regularly comanage the care of PLHIV in collaboration with community general practitioners. In clinic, participants could access the survey through a QR code or request that a weblink be sent to them after clinic via email or text message. Participation in the survey was anonymous, voluntary, and participants could leave any question unanswered. The survey was conducted between August 26, 2020 and November 26, 2020.
Results
Demographics
During the 3-month study period, 153 participants responded, with 128 (84%) of these completing the entire survey. The majority of participants identified as male (n = 112, 77%), were aged between 30 and 60 years (n = 108, 77%), and were born in Australia (n = 87, 63%). The remaining participants were from 25 other countries. Twenty-six (18%) participants identified as female, three (2%) as nonbinary, and four (3%) as other gender. There were no participants who identified as transgender and no participants younger than 21 years of age. Of the participants who provided their postcode, almost all (n = 137, 99%) had a Victorian postcode. See Table 1 for participant characteristics.
Participant Characteristics
Countries with more than one respondent included Great Britain, Greece, Japan, Malaysia, New Zealand, Philippines, Russia, South Africa, United States of America, and Zimbabwe.
Personal relationships
Participants were asked how the COVID-19 pandemic affected their personal relationships and how well connected they felt with their friends and family. Responses are summarized in Figure 1A. Fifty-five (43%) participants answered that the COVID-19 pandemic had negatively impacted their personal relationships, whereas 17 (13%) reported a positive impact. Forty-five (35%) participants reported that they rarely or did not at all feel well connected to friends and family. Forty (31%) reported that they often felt well connected to their friends and family.
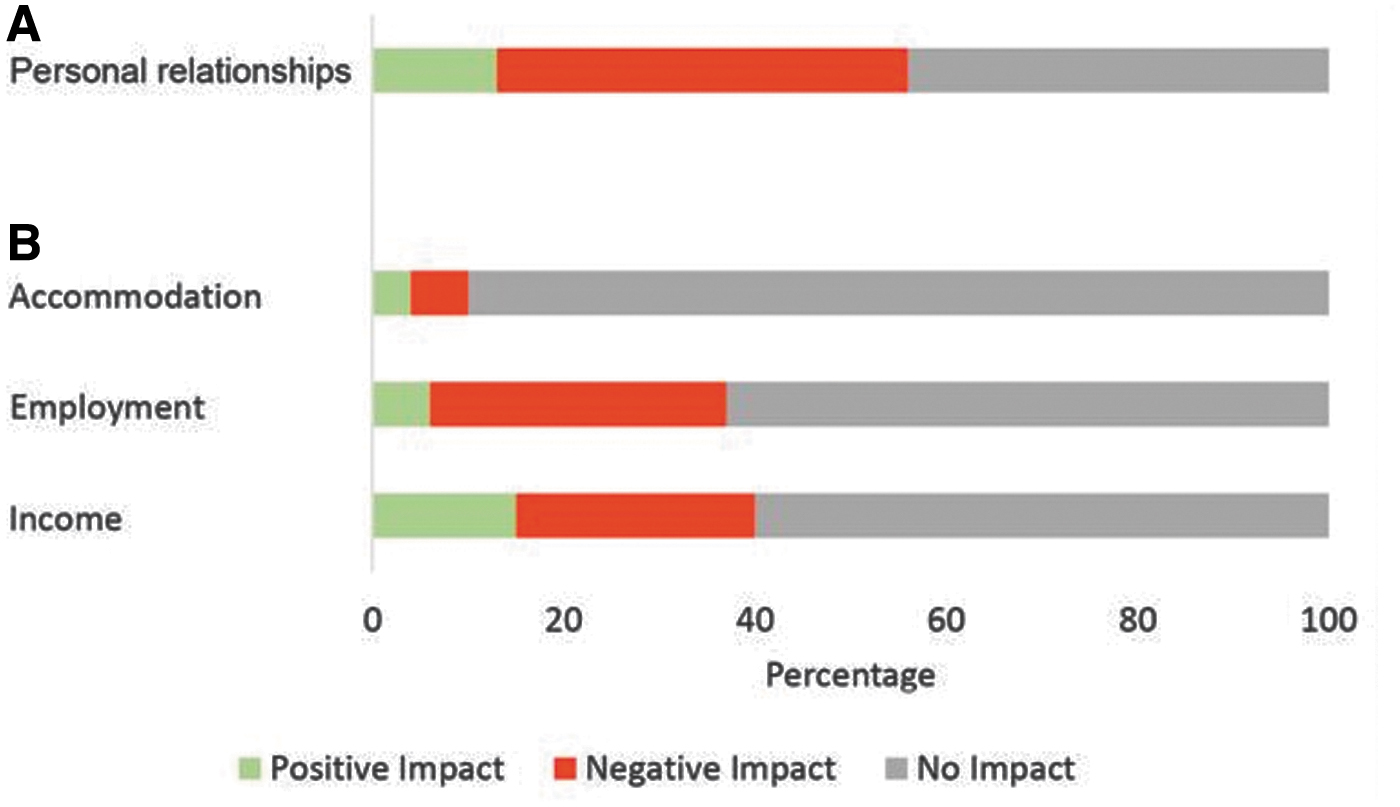
Income, employment, and accommodation
Participants were asked how the COVID-19 pandemic affected their income, employment, and accommodation. The majority of respondents reported no impact upon income (n = 78, 60%), employment (n = 81, 63%), or accommodation (n = 117, 90%). However, 32 (25%) participants reported experiencing a negative impact upon income, and 39 (31%) and 8 (6%) reported negative impacts upon employment and accommodation, respectively. A small proportion reported a positive impact upon these domains (n = 20, 15% income; n = 8, 6% employment; n = 5, 4% accommodation). Responses are summarized in Figure 1B. Participants were also asked about their utilization of government support payments. The survey found a slight increase in the use of government support payments during the pandemic (29% before vs. 34% during) and a slight decrease in those who felt that they needed support but were not eligible (9% before vs. 4% during).
Weight and food security
Sixty-six (50%) participants reported weight gain and 26 (20%) reported weight loss. Most respondents reported that their food intake and ability to access food were unaffected (n = 69, 52% and n = 109, 83%, respectively). Forty-six (35%) participants reported increased food intake, and 17 (13%) reported less intake. Furthermore, 19 (14%) participants said that their ability to access food had been negatively affected. The most common reasons for this were self-isolation (47%), inability to travel (35%), and inability to afford food (24%).
Substance use
The majority of participants stated that they did not use recreational drugs (n = 81, 62%), and 33 (25%) said that they did not consume alcohol. Increased alcohol intake was reported by 35 (27%) participants with a third of these reporting that they were drinking a lot more. Reduced alcohol intake was reported by 27 (21%) participants. Increased utilization of recreational drugs was reported by 19 (15%) participants, and 15 (12%) reported less use.
Access to medical care
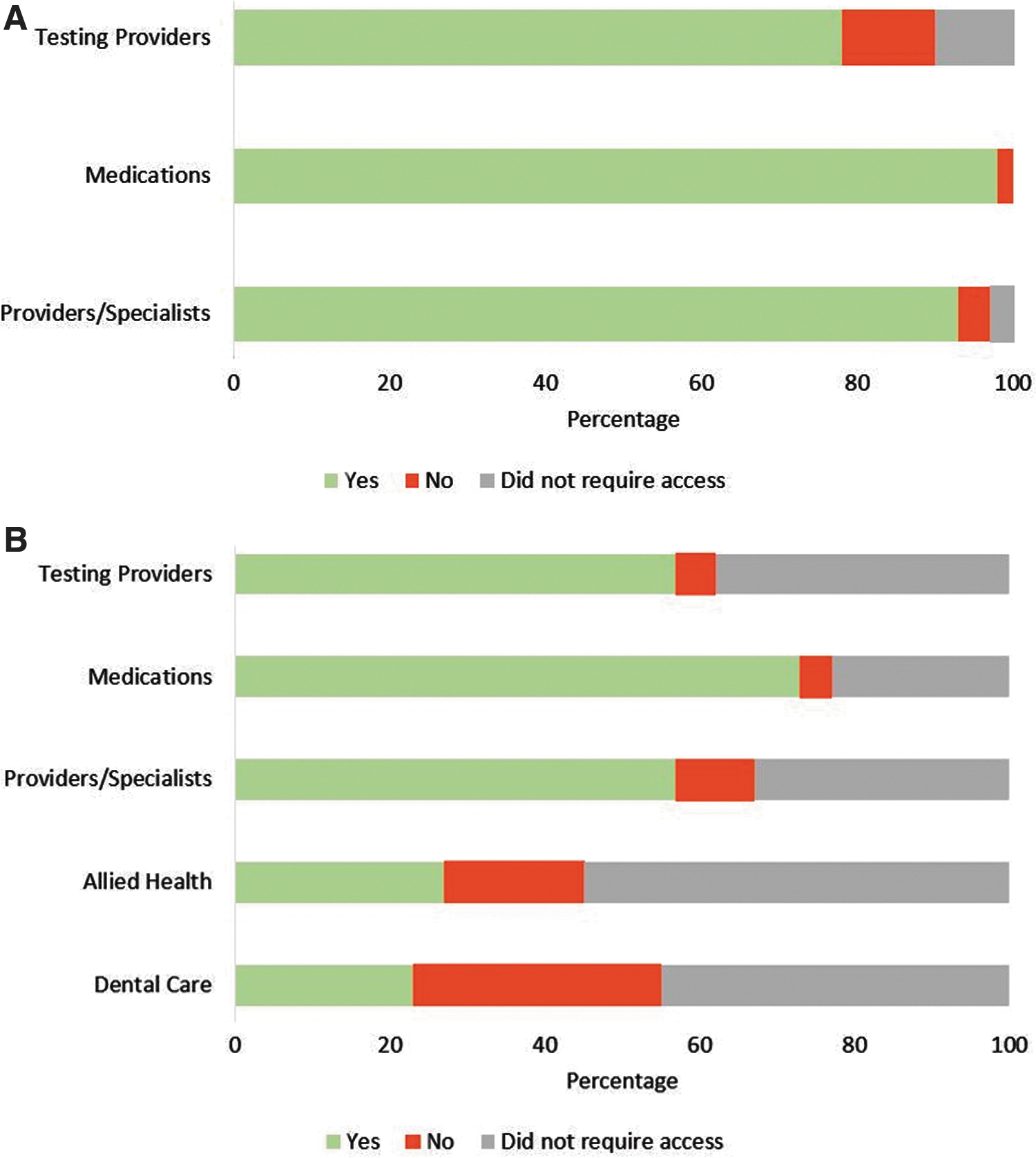
The majority of participants were able to access their HIV-provider during the pandemic (n = 124, 95%). Of the six respondents who were unable to access their HIV-provider, one attributed this to appointment cancellations, one inability to travel, and four did not provide a reason. Almost all (n = 130, 98%) participants were able to access antiretroviral therapy (ART). Of the three participants who were unable to access ART, one reported being unable to afford ART, and two did not provide a reason. One hundred five (87%) participants were able to access HIV-related monitoring tests such as pathology providers. The most common reasons for being unable to access testing providers were self-isolation (30%) and inability to travel (30%). Telehealth was used by 125 (92%) participants with 91 (77%) reporting being satisfied or very satisfied with telehealth appointments.
Participants were asked about their ability to access dental care, allied health services, other medical providers, medications, and monitoring tests. Of the 71 participants who required dental care during the pandemic, 41 (58%) were unable to access a dentist, 18 of these attributed this to appointment cancellations. Of the 59 participants who required an allied health service, 24 (41%) were unable to access it. The most common reason given for this was appointment cancellations, reported by nine (56%) participants who provided a reason. Conversely most participants were able to access non-HIV providers/specialists (n = 75, 85%), non-HIV medications (n = 96, 95%), and non-HIV-related testing providers (n = 75, 93%) when required. Most participants had the annual influenza vaccine in 2020 (n = 108, 80%). Responses regarding access to medical care are summarized in Figure 2.
Apprehension and the future
Participants were asked how often they felt concerned about the COVID-19 pandemic affecting their physical health, mental health, financial situation, and accommodation. These responses are summarized in Figure 3. Eighty-eight (68%) and 86 (66%) reported worrying sometimes or often about their physical health and mental health, respectively. Sixty-five (50%) and 30 (23%) reported worrying sometimes or often about their financial situation and accommodation, respectively. When asked how often they felt optimistic about the future after COVID-19, 45 (35%) answered rarely or not at all, 44 (34%) answered sometimes, and 39 (31%) answered often. Participants were also asked how the COVID-19 pandemic affected their willingness to enroll in clinical research or clinical trials. Most said that their willingness to participate was unchanged (n = 91, 71%), however, 27 (21%) answered that they were more willing to participate.
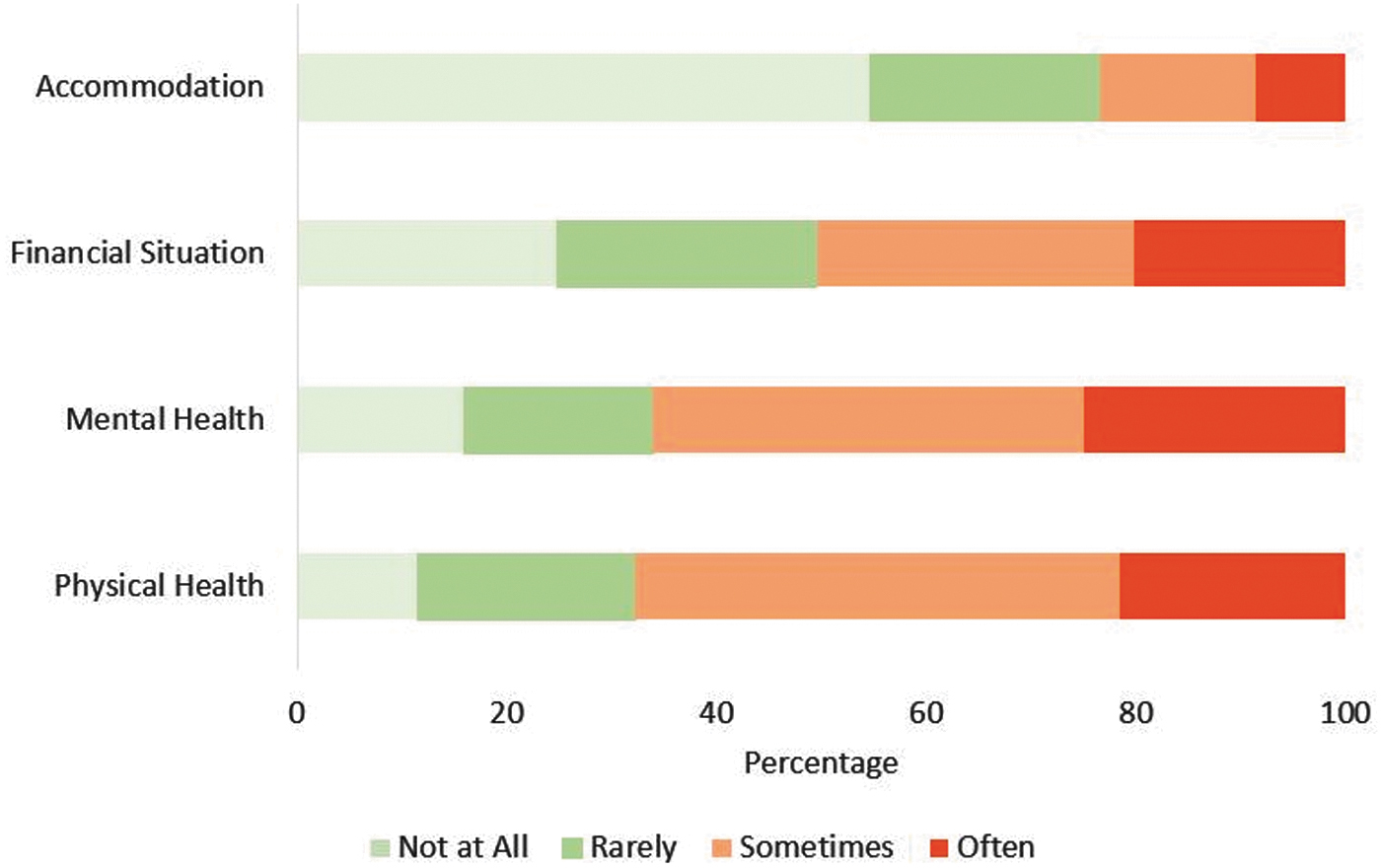
High proportions of PLHIV reported feeling sometimes or often concerned about physical health, mental health, finances, and accommodation.
Discussion
We created and distributed an online survey in collaboration with key HIV community-based organizations to examine the impact of the COVID-19 pandemic upon PLHIV in Victoria, Australia. The 153 responses demonstrated that PLHIV were negatively impacted by the COVID-19 pandemic in multiple ways. The domains most frequently reported as being negatively impacted were personal relationships (reported by 43%), employment (reported by 31%), and income (reported by 25%). A similar level of negative impact upon income and employment by the pandemic was found by a survey conducted by the National Association of People with HIV Australia (NAPWHA) in April 2020, during the first wave of the pandemic. However, our study demonstrated a larger negative impact on personal relationships. The NAPWHA report demonstrated 29% of respondents had experienced loss of income and 32% had experienced employment loss or increased workload, whereas only 18% reported that their relationships had been affected. 11 Our study, having been conducted during the second wave and while stage 4 restrictions were in place, found that the proportion of PLHIV reporting negatively impacted relationships had doubled since the NAPWHA survey (which was conducted earlier in the pandemic and collected responses nationally). Economic strain experienced by PLHIV during the pandemic appears to be ubiquitous globally, a study conducted in Argentina of 1336 PLHIV showed that 41% experienced economic hardship during the pandemic. 12 Our study and these other reports highlight the need for programs promoting economic assistance to PLHIV during the pandemic as well as those which improve social connectedness.
Despite concerns that the COVID-19 pandemic would impair HIV testing and care, 13 an important positive finding was that HIV care in Victoria largely continued uninterrupted. The vast majority of participants were able to access their HIV provider, ART-, and HIV-related testing when required. This is consistent with the international experience of PLHIV, the Argentinian PLHIV survey showed similar results in that 96% were able to access ART. 12 However, a review of the European HIV clinic activity showed that, while no HIV clinics closed or experienced ART shortages since the start of the pandemic, only 30% of clinics were operating at normal capacity. 14 Furthermore, a review of a HIV clinic's activity in San Francisco during a shelter-in-place order showed that while clinic attendance rates did not fall, patients were less likely to maintain virological suppression. 15 Our study and the international literature demonstrate continuity of HIV care during the pandemic and highlight the role of the HIV provider as a safety net during times of health care strain.
In contrast to HIV care provision, our study found that access to other health care services was less consistent. Notably, large proportions of participants were unable to access dental care and allied health services during the pandemic. The reduced access to dental care was due to the closure of all but emergency dental services in Victoria. 16 Similarly, many allied health services had closed, limited their operations, or transitioned to telehealth. 17,18 Other studies have demonstrated dental care being delayed 19 and dental and allied health clinic closures during the COVID-19 pandemic. 20,21 This study demonstrated that access to medical providers, medication, and testing for non-HIV care largely continued with the vast majority able to access these services when required. Telehealth was used by 92% of participants during the pandemic and 77% reported being satisfied or very satisfied with their telehealth appointments. The NAPWHA report showed that only 61% of respondents had used telehealth appointments. 11 This may be due to the NAPWHA survey being conducted earlier in the year when more clinics were still permitted to conduct face-to-face reviews. Furthermore, in the NAPWHA survey, when asked to rate their satisfaction with telehealth on a scale from 0 (not at all) to 5 (extremely satisfied), only 41% of respondents gave a score of 4 or 5. 11 Given our survey was conducted later in the year, technology infrastructure may have improved, and patients may have become more accustomed to telehealth. Our study suggests that telehealth is a viable alternative, which is well received by PLHIV for continuing care during the pandemic.
Another important finding from our study was that a large proportion of PLHIV were concerned about the pandemic negatively impacting their physical health, mental health, and finances. In addition, over a third rarely or did not at all feel optimistic about the future, whereas 31% often felt optimistic about the future. In contrast, the NAPWHA report showed that only 9% of respondents felt optimistic about the future. 11 Several other studies of the general population have shown increased symptoms of anxiety and depression during the COVID-19 pandemic, even in individuals without preexisting mental health concerns. 22 –24 The high proportion of PLHIV worried about their mental health highlights the importance of service providers enquiring about mental health with all patients and having access to clear referral pathways to mental health services if issues are identified.
Half the study population reported weight gain during the pandemic, which is a higher proportion than described in existing Australian data of the general population. An Australia-wide survey showed that 39% of Australians felt that they had gained weight during the COVID-19 pandemic. 25 This survey had similar rates of perceived weight loss and increased food intake to our study. This is cause for concern as PLHIV are already at an increased risk of complications of weight gain such as hypercholesterolemia, diabetes, and cardiovascular disease compared to the general population. 26 –28 Providers should be encouraged to monitor patient weight, and enquire about diet and exercise during routine assessments. Access to dietetic services and advice on exercise programs that are compatible with pandemic restrictions should be made available to PLHIV.
There were several limitations to this study. Notably, a relatively small sample size limited the ability for the results to be generalized to all PLHIV. The study was also subject to selection bias, given it was recruited through infectious diseases clinics during the pandemic and likely selected for PLHIV who were engaged in care. The study also selected for participants who were literate in English and had internet access. This could have been mitigated by translating the survey into other languages and having a paper-based method for responding. For these reasons, it is possible that our study sample was not fully representative of PLHIV in Victoria despite efforts to disseminate the survey widely. It would also have been useful to compare the effects of the pandemic upon people who were not living with HIV to assess if PLHIV were disproportionally affected.
Conclusion
The COVID-19 pandemic has had widespread negative effects on PLHIV in Victoria, Australia, including concerns about mental health and social isolation during the pandemic. It emphasized the importance of providers enquiring about mental health and lifestyle changes during routine assessments and having robust mental health support and social welfare services available. Positively, this study found that HIV care and access to ART were largely uninterrupted, assisted by telehealth, which was overall satisfactory for patients. Further research is required to fully conceptualize the impact of the COVID-19 pandemic on PLHIV to best maintain service provision during and after the pandemic.
Footnotes
Authors' Contributions
All authors contributed to study protocol development, survey design, and participant recruitment. Authors M.W., J.O., C.K., and J.L. were involved in ethics approval and data analysis. All of the listed coauthors have reviewed and approved the article before submission.
Acknowledgments
The authors thank the PLHIV who generously shared their time and experiences by participating in the study survey. They thank the following people: Kirsty Machon from Positive Women Victoria, John Rule and Charlie Tredway from the National Association of People with HIV Australia (NAPHWA), and Miranda Smith from
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.