
Abstract
People with HIV (PWH) might have a higher risk of adverse coronavirus disease 2019 (COVID-19) outcomes. Several scores were developed to predict COVID-19 progression to critical disease and are often used among PWH. We assessed the performance of two commonly used risk equations among PWH and COVID-19. Participants were identified from a multicenter cohort of 6,361 PWH on regular follow-up at 2 university hospitals. Of 99 HIV-infected individuals with confirmed SARS-CoV-2 infection, 63 had complete data and were included in this analysis. CALL and COVID-GRAM scores were calculated and participants were stratified into low-, intermediate-, and high-risk groups for each. Discrimination was assessed using receiver operating characteristic curves. Calibration was evaluated using observed versus expected (O:E) ratios and the Hosmer–Lemeshow χ2 goodness-of-fit statistic. Scores were adjusted by increasing one category level in individuals with nadir CD4 lymphocyte count <200/μL. Participants had a median nadir and current CD4 counts of 207 [interquartile range (IQR) 119–345] and 440 (IQR 280–719) cells/μL. Ten (15.9%) individuals progressed to critical disease and 4 (6.3%) died. Assessed scores showed acceptable discrimination (area under the curve 0.701–0.771) and were overall calibrated (O:E ratio 1.01). However, both overestimated the risk of progression among individuals in the low- and high-risk categories, whereas they underestimated the risk in the intermediate category (O:E 1.20–1.21). Thus, 50% of critically ill individuals were not identified as high risk. Assigning PWH with low nadir CD4 counts a higher risk of progression reduced the proportion of individuals not identified to 20%. COVID-19 risk scores had lower performance in PWH compared with that described in the general population and failed to adequately identify individuals who progressed to critical disease. Adjustment for nadir CD4 partially improved their accuracy. Risk equations incorporating HIV-related factors are needed.
Introduction
The outbreak of coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 infection has challenged health care systems worldwide. According to a nationwide epidemiological report in Spain, among 101,484 hospitalized patients, 8.6% required admission to an intensive care unit. 1 However, the wide clinical spectrum of COVID-19 and the heterogeneity of clinical course make it difficult to identify which individuals would progress to critical disease and benefit from prompt intensive care. 2 Several scores have been developed to predict COVID-19 progression to critical disease using easily available clinical and analytical variables. 3,4 In the general population, commonly reported risk factors associated with disease progression included older age, lymphocytopenia, comorbidities, and high levels of inflammatory markers. 3 –5
People with HIV (PWH) might have increased adjusted mortality rates due to COVID-19 compared with the general population and the use of these scores in the HIV population is of uncertain accuracy. 6,7 PWH have different demographics compared with the populations for whom COVID-19 progression risk prediction models were developed. 3,6,8 Additionally, there may be an association between HIV infection and COVID-19 severity. 6,7,9 In particular, low CD4 lymphocyte counts have an impact on COVID-19 mortality, which is not captured in the scores. 9 –11
The current study aimed to evaluate the rate of progression to critical disease in a multicenter cohort of PWH and COVID-19 and assess the performance of two web-based COVID-19 risk equations. Secondarily, we investigated whether we could improve the performance of the risk equations by assigning PWH with low nadir CD4 counts an adjusted score value.
Materials and Methods
Study population
This was an observational multicenter study. We used data from 2 cohorts of adult PWH at the Ramón y Cajal University Hospital (HURyC) and Fundación Jiménez Díaz University Hospital (HUFJD), 2 tertiary hospitals with a total of 6,361 adult patients on regular follow-up at the monographic HIV clinics. In the cohort of the HURyC, HIV-infected individuals, aged 18 years or older, with a diagnosis of suspected or confirmed COVID-19 were included prospectively and consecutively as of December 11, 2020. In the cohort of the HUFJD, anonymized data of HIV-infected individuals, aged 18 years or older, with a diagnosis of suspected or confirmed COVID-19 were collected retrospectively as of December 11, 2020. Study follow-up was performed until hospital discharge or recovery for ambulatory patients.
All research was done according to the Declaration of Helsinki and local legislation. The study protocol was approved by the institutional review boards of both centers (EC 110/20 HURyC and EO 091/20 HUFJD). Participants provided oral informed consent to minimize physical contact with study staff at the HURyC, and a waiver of consent was granted at the HUFJD because only deidentified data were extracted from the medical records. All participants received treatment according to local recommendations.
For the current analysis, we included data from all PWH with PCR-confirmed COVID-19 in ambulatory or hospitalized settings. Individuals for whom scores could not be calculated due to missing information were excluded. Critical disease was the primary outcome, defined as respiratory failure that required mechanical ventilation, organ failure with the need of intensive care unit admission, 12 or death due to COVID-19.
Risk prediction equations
We assessed the performance of two risk equations accessible online, which comprise clinical and analytical data easily available at tertiary hospitals: CALL and COVID-GRAM scores.
The CALL score, developed by Ji et al., is accessible as an online calculator and predicts progression to severe COVID-19 [respiratory rate ≥30 breaths/min, resting oxygen saturation ≤93%, partial pressure arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) ≤300 mmHg, requirement of mechanical ventilation, or worsening of lung computed tomography findings] based on data collected from 208 hospitalized patients with confirmed COVID-19 in China. 3 The model includes independent factors associated with progression in a multivariate Cox analysis. Using cutoff values of 6 and 9 points, the equation yielded a sensitivity of 95% and 45% and a specificity of 97% and 78%, respectively, for estimating the risk of progression in the derivation cohort. 3
The scores were classified into three categories of risk according to the probabilities of progression, as follows: 4–6 points (low risk, <10%), 7–9 points (intermediate risk, 10%–40%), and 10–13 points (high risk, >50%).
COVID-GRAM was developed by Liang et al. to estimate the probability of progressing to critical COVID-19 (admission to the intensive care unit, invasive ventilation, or death) using a nationwide cohort of 1,590 hospitalized Chinese patients with confirmed COVID-19. 4 The equation, accessible as an online calculator, was built based on variables consistently associated with the event using least absolute shrinkage and selection operator (LASSO) and logistic regression models. The equation was externally validated, achieving an area under the receiver operating characteristic (AUROC) curve of 0.88–0.98. 4 The scores were stratified into the following categories according to the probability of critical COVID-19: low-risk group 0.7%, intermediate-risk group 7.3%, and high-risk group 59.3%.
Data collection and definitions
Each equation comprises different variables that conferred an increased risk of progression to critical COVID-19. Demographics, comorbidity status, and clinical and radiological manifestations were collected from medical records. HIV-specific variables were extracted from medical records and consisted of the calendar year of HIV infection diagnosis, nadir and most recent (i.e., within previous 6 months) CD4 lymphocyte count, recent CD4/CD8 ratio, recent RNA-HIV plasma viral load, and current antiretroviral therapy. The laboratory parameters, including lactate dehydrogenase, C reactive protein, total and differential leukocyte counts, hemoglobin, platelets, direct bilirubin, creatinine, and sodium, were examined at the first hospital consultation. Oxygen saturation was measured by pulse oxygen saturation at rest state.
Confirmed COVID-19 was defined by positive, qualitative, real-time RT-PCR assay of nasopharyngeal swabs, sputum, or lower respiratory tract aspirates.
Statistical analysis
The data were described using absolute numbers and percentages for categorical variables and mean, range, median, and interquartile ranges (IQRs) for continuous variables. Normally distributed variables were compared by the independent sample t-test, whereas non-normally distributed variables were compared using the Mann–Whitney Wilcoxon test. Comparisons between categorical variables were assessed by χ 2 test. Specifically, Fisher's exact test was applied when more than 20% of cells in the 2 × 2 table had expected frequencies of <5. We used binary logistic regression models to explore the factors associated with critical COVID-19 in our population, adjusting for age, gender, nadir CD4 cell counts, and years of HIV infection.
CALL and COVID-GRAM scores were calculated and participants were stratified into low-, intermediate-, and high-risk groups for each algorithm according to previously reported cutoff values. 3,4 The ability of each score to discriminate the progression to critical disease was assessed using receiver operating characteristic (ROC) curves, and the AUROC curve for our population was determined. AUROC curve values between 0.50 and 0.59 were considered poor, 0.60 and 0.69 moderate, 0.70 and 0.79 acceptable, and 0.80 and 1.00 very good to excellent. 13 The sensitivity, specificity, and predictive values were calculated both according to previously published cutoff values and to the best cutoff values for our cohort. 3,4
Considering the harm associated with overlooking an individual who may progress to severe COVID-19, we selected cutoff values that provided a minimum sensitivity of 90% while having the highest specificity. Calibration was assessed using the mean observed versus expected (O:E) ratio and the Hosmer–Lemeshow χ 2 goodness-of-fit statistic.
We additionally investigated whether the performance of the scores might be improved by considering the nadir CD4 lymphocyte count. The extent to which the nadir CD4 lymphocyte count affects the progression of COVID-19 is still unknown. Therefore, we arbitrarily adjusted the scores by increasing one category level in individuals with nadir CD4 lymphocyte counts <200/μL. Statistical significance was defined as a two-sided p value of <.05. All statistics were done with IBM SPSS Statistics, version 25.0.
Results
During the study period, a total of 99 HIV-infected individuals had a confirmed SARS-CoV-2 infection. Sixty-three had complete data on all variables to calculate the scores and were included in this analysis. Participants were predominantly male (87.3%), Caucasians (73%), and with a mean age of 52 (range 19–77) years. The median nadir and current lymphocyte CD4 counts were 207 (IQR 119–345) and 440 (IQR 280–719) cells/μL. Forty PWH (63.5%) had at least one comorbidity, the most prevalent of which were hypertension (36.5%) and chronic hepatitis (27.0%, Table 1).
Demographics and Clinical Characteristics of the Cohort Stratified by COVID-19 Severity
p Values calculated between individuals with and without critical COVID-19 using a χ 2 test or Fisher's exact test for categorical variables and Mann–Whitney U test for continuous variables.
At first hospital consultation.
Bold values indicate statistical significance with p value <.05.
COVID-19, coronavirus disease 2019; eGFR, estimated glomerular filtration rate; IDU, intravenous drug user; IQR, interquartile range; MSM, men who have sex with men; SpO2/FiO2, pulse oxygen saturation-to-fraction of inspired oxygen; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate.
A total of 10 (15.9%) individuals progressed to critical disease and 4 (6.3%) died over a median of 3.5 (IQR 0.0–17.5) days from COVID-19 diagnosis. Clinical characteristics of the population according to the progression to critical disease were compared (Table 1). Overall, both groups had similar baseline characteristics, except for the lower nadir CD4 lymphocyte count (107 and 225 cells/μL, p = .047), and higher leukocyte–lymphocyte ratio (0.7 and 1.4, p = .055) among individuals who progressed to critical disease. In the adjusted binary logistic regression model, we did not find any factor statistically associated with critical COVID-19 (Table 2).
Binary Logistic Regression Model for Predicting Critical Illness Among a Cohort of People with HIV
Data in rows belong to independent variables in the regression, in relation to the alternative “critical illness” dependent variable.
Statistical significance is considered as a p value <.05. For this model, the null hypothesis needs to be retained.
CI, confidence interval.
The median calculated risk of critical disease was 7 (IQR 5–10; intermediate category) and 91 (IQR 50–134; intermediate category) when using CALL and COVID-GRAM, respectively. Progression rates among low-, intermediate-, and high-risk categories were 4.8%, 17.4%, and 26.3% for the CALL score and 0%, 15.2%, and 35.7% for the COVID-GRAM score, respectively (Fig. 1).

Rate of progression to critical COVID-19 among people with HIV according to CALL (dark gray) and COVID-GRAM (light gray) risk categories. Columns express the percentage of individuals with critical disease within low-, intermediate-, and high-risk categories. COVID-19, coronavirus disease 2019.
The AUROC curve of the COVID-GRAM score was 0.771 [95% confidence interval (CI) 0.627–0.915], higher than the CALL score (area under the curve 0.701, 95% CI 0.560–0.842), yielding acceptable discrimination (Fig. 2). The negative and positive predictive values (NPV and PPV) for critical disease according to published cutoffs are displayed in Table 3. The best cutoff values for our population were 6 points for the CALL score (NPV 95.2% and PPV 21.4%) and 80 points for the COVID-GRAM score (NPV 96.0% and PPV 23.7%).
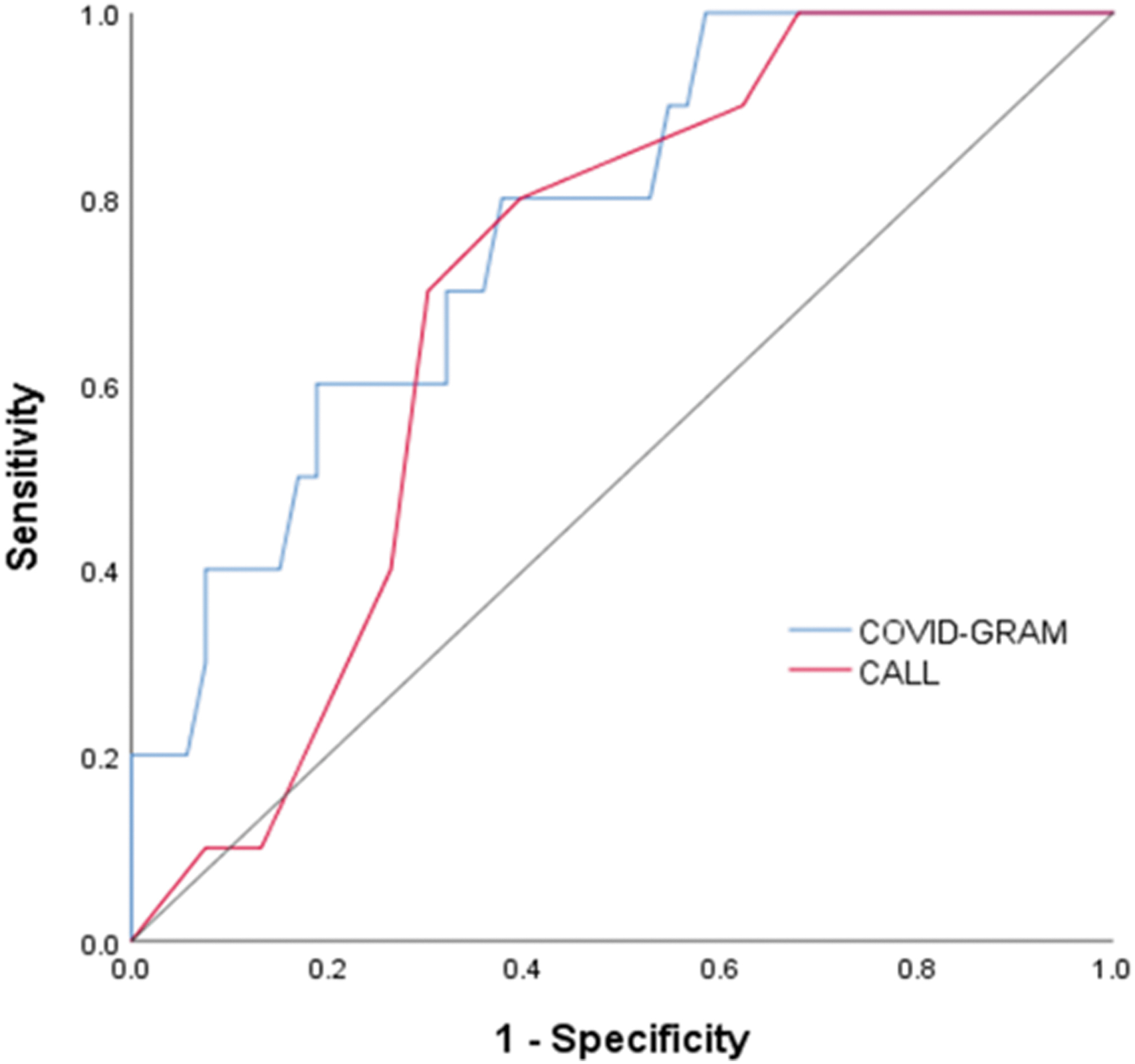
Receiver operating characteristic curves for CALL (red line) and COVID-GRAM (blue line) scores for the risk of progression to critical COVID-19 in people with HIV. The gray line represents the line of equality.
Area Under Receiver Operating Characteristic Curve and Comparison of Predictive Assessment Between CALL and COVID-GRAM Scores for Estimating the Risk of Progression to Critical Disease Among People with HIV
Best cutoff values for the cohort selected to provide the highest specificity within the 90%–100% sensitivity range.
Agreement between previously published and best cutoff values for the cohort.
AUROC curve, area under the receiver operating characteristic curve; NPV, negative predictive value; PPV, positive predictive value.
The equations showed no evidence of lack of fit with our data, as reflected by Hosmer and Lemeshow χ 2 values of 8.62 (p = .196) for the CALL score and 1.973 (p = .982) for the COVID-GRAM score. In the overall cohort, calibration was found to be good (O:E ratio 1.01). Nevertheless, both scores overestimated the risk of progression among individuals in the low- and high-risk categories [O:E ratios: CALL 0.78 (low) and 0.91 (high); COVID-GRAM 0.00 (low), 0.94 (high)]. Conversely, the risk was underestimated in the intermediate-risk category (O:E ratios: CALL 1.20; COVID-GRAM 1.21).
When the scores were arbitrarily adjusted according to the nadir CD4 lymphocyte count, the prediction was more accurate in the high-risk category (O:E ratios: CALL 1.03; COVID-GRAM 0.98) since three of five individuals who progressed to critical disease and had not been identified by the original equation were reclassified as high-risk individuals (Table 4).
Predicted Versus Observed Events for CALL and COVID-GRAM Scores According to the Risk of Progression to Critical Disease Among People with HIV
The Hosmer–Lemeshow goodness-of-fit test showed no significant differences between the observed and predicted values for the overall scores (p > .05).
Scores were adjusted by increasing one category level in individuals with nadir CD4 lymphocyte counts <200/μL.
O:E, observed versus expected.
Discussion
Early identification of individuals with COVID-19 that will progress to critical disease could facilitate decision-making regarding the best management strategy. 2 There is a controversy whether PWH have a higher risk of poor outcomes due to COVID-19. On the one hand, an analysis of the largest HIV cohort of PWH in the United States found no differences in overall mortality among HIV-positive and HIV-negative individuals, 14 but on the other hand, the ISARIC and OpenSAFELY cohorts in the United Kingdom found an increased risk of mortality among PWH, even after adjusting for social conditions. 6,7 Some of these cohorts did not have data on HIV-specific variables and the ultimate cause of the increased risk could not be determined.
In our study, 15.9% of the sample progressed to critical disease, similar to other cohorts of PWH, although higher than the current crude rate of progression in the general population of our region (8.6%). 1,10,14 Moreover, among individuals in the fifth decade of age (the mean age of our cohort), the intensive care unit admission rate in our study was considerably higher than in the general population of Spain (0.7%).
Several scores were proposed to predict critical disease or mortality in the general population, although they had not been evaluated in HIV-positive populations. We assessed the performance of two available web-based risk calculators in a multicenter cohort of PWH with confirmed SARS-CoV-2 infection. Overall, the assessed prediction equations acceptably discriminated individuals who progressed to critical COVID-19 from those who did not. However, both overestimated the risk of progression among PWH in the low- and high-risk categories, whereas they underestimated the risk in the intermediate category. Assigning PWH with nadir CD4 lymphocyte count <200 cells/μL a higher risk of progression partially improved the identification of critically ill individuals, suggesting that other factors determine the risk of progression in PWH.
The accuracy of the scores based on AUROC curves in our population was 23% and 12% lower than that reported in the derivation cohorts of the CALL and COVID-GRAM, respectively. 3,4 Using the best cutoff value for our population did not lead to an improvement of the NPV or PPV. Interestingly, the scores overestimated the risk of progression for the extreme categories, and only 26%–36% of our cohort classified as high risk actually evolved to critical disease.
Conversely, half of the individuals with COVID-19 progression were not identified as high risk, indicating that critically ill PWH are not appropriately assigned across the scoring categories. These may be related to the differences between the populations where the equations were developed and our HIV-positive sample. Indeed, HIV-positive populations tend to have a young age distribution and a high prevalence of comorbidities, which may not be captured by the score derivation cohorts. 6,15
Likewise, some factors that may influence COVID-19 evolution are specific to the HIV-positive population, such as the immune deficiency reflected by low CD4 lymphocyte counts. In this line, low CD4 counts have been identified as factors associated with worse outcomes in some observational studies. Hoffmann et al. found that the only factor associated with mortality was nadir CD4 count. 11 Additionally, current CD4 lymphocyte counts of <200 cells/μL were associated with increased rates of hospitalization, critical disease, and death in a multicenter cohort. 10 In our study, we did not find an association between nadir CD4 lymphocyte count and critical COVID-19, probably due to the small sample size.
Considering previous studies, we hypothesized that adjusting the scores according to nadir CD4 lymphocyte count could enhance the predictive performance of the equations. Indeed, it improved prediction among individuals in the high-risk category by 11% and 3% for the CALL and COVID-GRAM scores, respectively, but it still was not able to identify 20% of individuals who progressed to critical disease.
The reason for this finding may be due to a minor effect of the nadir CD4 lymphocyte count on the probability of progression, while other relevant factors are not taken into account. This underlies the fact that the eventual evolution of COVID-19 in PWH is a complex interaction of age, immune status, inflammation, comorbidities, treatments applied (including antiretrovirals), and potentially other factors. Prediction equations developed specifically for PWH are necessary for early and accurate identification of individuals who will progress to critical disease and, therefore, offer a targeted management strategy. In the meantime, increasing the level of risk to the next category for individuals with low nadir CD4 lymphocyte counts can improve the performance of the scores.
Our results should be interpreted in the context of several limitations. First, the small sample size with a small proportion of female and non-Caucasian participants precluded us to perform any sex- or ethnicity-stratified analyses. Our results might therefore not be generalizable to HIV-positive populations with different demographic composition. However, the sample consisted of PWH, with a wide range of duration of HIV infection and nadir/current CD4 lymphocyte counts. Second, the score adjustment was arbitrary based on previous evidence and the exact effect of nadir CD4 count on progression to critical disease is currently unknown. Third, new scores have been published recently and we were not able to assess their performance on PWH. 16
Finally, we excluded 36% of our original cohort due to a lack of complete data to calculate the scores. All of those individuals recovered without progression to critical disease, a group that was already well represented in the included population. Therefore, it is unlikely that the excluded sample influenced our results.
Conclusions
COVID-19 risk scores had lower performance in PWH compared with that described in the general population and failed to adequately identify individuals who progressed to critical disease. Adjustment for nadir CD4 partially improved their predictive ability. Risk equations incorporating HIV-related factors are needed.
Footnotes
Authors' Contributions
J.L.C., A.C., and P.V. conceived and designed the study. P.V., A.C., A.M., M.J.V., J.L.-B., B.Z., M.G., and J.L.C. were responsible for patient inclusion and clinical follow-up and helped to write the work. J.L.C., A.C., A.M., and P.V. collected the data. J.L.C. and P.V. did the analysis and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors critically revised the manuscript and gave final approval for the final version.
Acknowledgment
The authors would like to thank Ana Abad for her significant contribution to database management.
Author Disclosure Statement
A.C. reports grants and personal fees from ViiV Healthcare, personal fees from Gilead, personal fees from Janssen, and personal fees from Merck, outside the submitted work. M.G. reports grants and personal fees from ViiV Healthcare, personal fees from Gilead, and personal fees from Janssen, outside the submitted work. M.J.V. reports grants and personal fees from Gilead and ViiV, outside the submitted work. For the remaining authors, none was declared. All research was conducted within the guidelines of ethical principles and local legislation.
Funding Information
No funding was received for this article.