
Abstract
A 38-year-old male patient presented to the emergency department with fever and dyspnea. Hospitalization was warranted and soon coronavirus disease 2019 (COVID-19) was diagnosed based on a positive SARS-CoV-2-PCR. Over the following weeks his condition gradually worsened, leading to admission at the intensive care unit. Because of unexplained weight loss before admission, a HIV screening was performed. HIV was confirmed and additional tests showed an undetectable CD4+ T cell count, alongside a number of co-infections. Convalescent plasma therapy, which has been shown to be effective in severe humoral immunodeficiency was tried, but was not effective. One week after the HIV diagnosis, antiretroviral therapy was started and finally, 3 months after the initial positive test and after partial recovery of cellular immunity, the COVID-19 virus was cleared. In the end, the patient made a full recovery. Our case demonstrates a prolonged COVID-19 infection in a patient with undiagnosed HIV with severely impaired cellular immunity.
During the current coronavirus disease 2019 (COVID-19) pandemic the incidence of newly diagnosed HIV infections declined and late presentations were more common than before the pandemic, as described by de Mendoza et al. 1 However, to our knowledge, no data are available on the outcome of patients with severely impaired cellular immunity due to undiagnosed HIV and COVID-19. Furthermore, the importance of early detection of potential immunodeficient patients is becoming more clear.
This is not only vital for the treatment of the patient but also in public health perspective. As lately, more and more is known about the problem of genetic evolution of the SARS-CoV-2 virus in patients with severe immunosuppression. This causes a public health risk as potential more transmissible or more pathogenic variants can arise from this genetic evolution. Early diagnostics for potential immunodeficiencies should, therefore, be performed when indicated. 2 –4 In this light, we would like to demonstrate a case of a prolonged COVID-19 infection in a patient with undiagnosed HIV.
A 38-year-old male patient presented to the emergency department with fever, thoracic pain, and dyspnea. He recently moved to The Netherlands as a migrant worker from Poland. Complaints started a few days before presentation, multiple of personal contacts were already diagnosed with COVID-19. Physical examination showed a high breathing frequency of 30/min and low pulse oxygenation (88%). Blood tests showed a lymphopenia, mildly elevated C-reactive protein (29 mg/L), and ferritin (758 μg/L).
The chest X-ray showed bilateral consolidations. Hospitalization was warranted and soon COVID-19 was diagnosed based on a positive SARS-CoV-2 PCR. Over the following 2 weeks his condition gradually worsened. Because of progressive dyspnea and additional medical information revealing unexplained weight loss of 13 kg before admission, a HIV screening was performed. HIV was confirmed (Centers for Disease Control and Prevention classification stage 3 5 ) and additional blood tests showed an undetectable CD4+ T cell count (<1 × 106/L, ref; 50–170 × 106/L) and HIV RNA of 980,000 copies/mL and a Pneumocystis jiroveci pneumonia (PCP) infection was suspected. He was never tested before for HIV, only had heterosexual contact, and he denied intravenous drugs use.
He was transferred to the intensive care unit (ICU) because of respiratory failure and mechanical ventilation was started. Additional diagnostics were performed and a broad spectrum of co-infections was found besides the ongoing COVID-19 infection, including PCP, hepatitis B (HBvDNA 330,537,000 IE/mL, HbsAg positive, anti-Hbc positive, HbeAg positive), lues latens tarda, Mycoplasma pneumoniae and multiple Kaposi's sarcomas on tongue, oral mucosa, and skin. Treatment for the PCP infection was started (high dose prednisone and co-trimoxazole), alongside broad-spectrum antibiotics.
After initial stabilization and despite the risk of developing immune reconstitution inflammatory syndrome (IRIS), combination antiretroviral therapy (C-ART) (emtricitabine/tenofovir and dolutegravir) was started 1 week after diagnosis. Eventually leading to a slow recovery of the CD4 count (Fig. 1). The patient developed progression of the Kaposi's sarcomas, probably due to IRIS after start of the C-ART. Owing to the ongoing COVID-19 infection in the absence of COVID-19 antibodies, probably caused by the low CD4 count in addition to the high-dose corticosteroids for his PCP infection, treatment with convalescent plasma therapy (CONVP) was initiated.
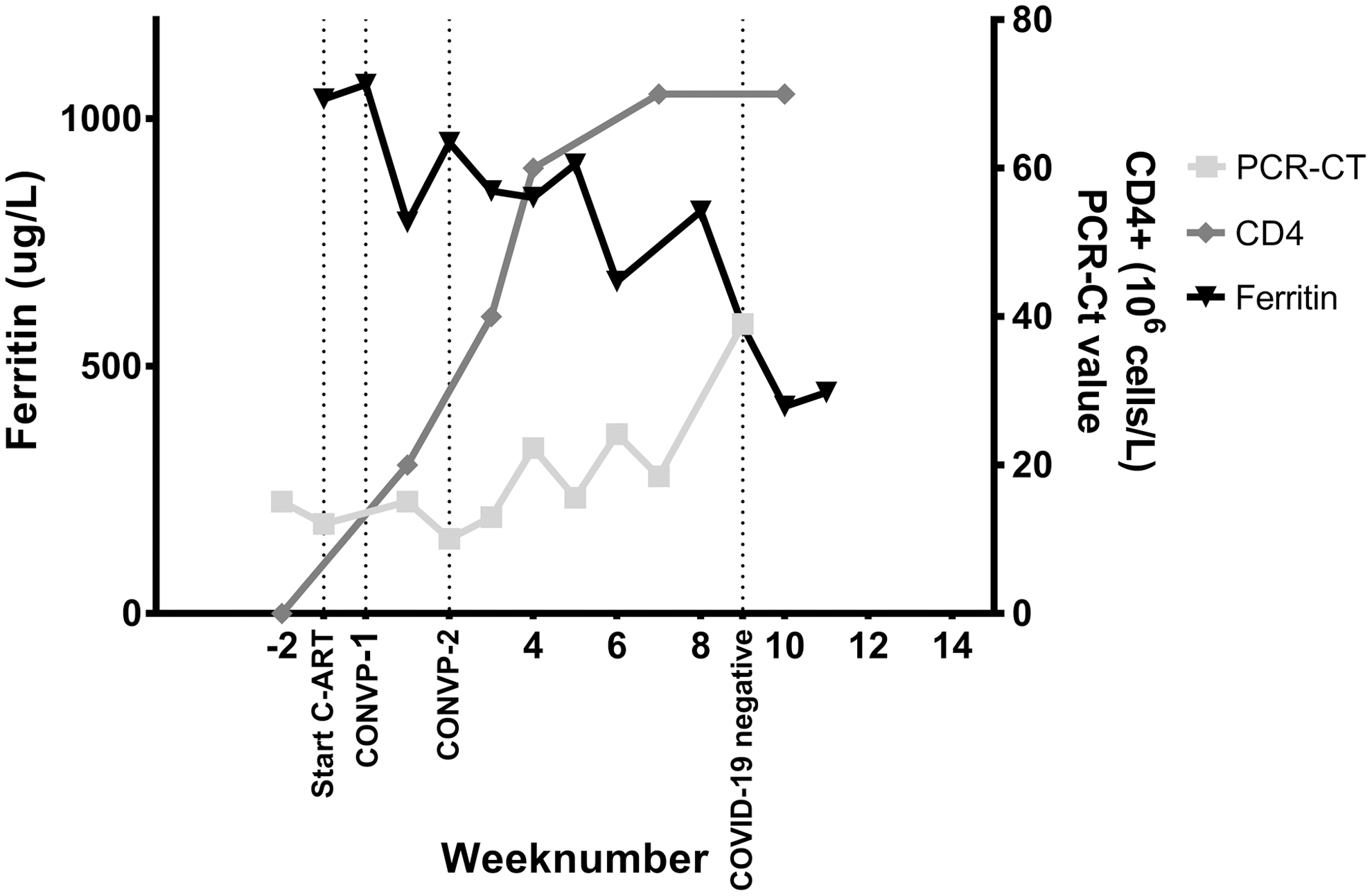
Overview of inflammation, immunity, and COVID-19 in our patient. C-ART, combination antiretroviral therapy; CONVP, convalescent plasma therapy; PCR-CT, cycle threshold PCR.
CONVP was ultimately given twice with an interval of 2 weeks. After 3 months in total and after partial recovery of cellular immunity, the patient finally cleared the COVID-19 virus (Ct-value >35; Fig. 1). After prolonged weaning due to ICU acquired weakness, he was eventually discharged to the regular ward, 11 weeks after being admitted to the hospital. After clearing SARS-CoV-2 and with a partially recovery of the CD4 cell count (CD4 count 70 × 106/L, HIV RNA 42 copies/mL), treatment for the Kaposi's sarcoma (liposomal doxorubicin) was started. Eventually the patient made a full recovery.
Our case demonstrates a prolonged severe COVID-19 infection in a patient with undiagnosed HIV with severely impaired cellular immunity. CONVP, which has been shown to be effective in severe humoral immunodeficiency was tried, but was not effective. 6 In the end, the COVID-19 virus was cleared after partial recovery of cellular immunity.
Furthermore, our case illustrates the importance of a thorough anamnesis and broad diagnostic approach, especially during the current COVID-19 pandemic. In our patient the COVID-19 infection, also often presenting with lymphopenia, mildly elevated inflammation parameters and bilateral consolidations on chest X-ray, masked the PCP infection in a patient with undiagnosed HIV.
Footnotes
Authors' Contributions
Writing original draft and data collection by T.K. Writing review and editing by J.G., M.C., and A.S. Microbiology diagnostics, writing review, and editing by C.S. and E.v.L. Pulmonary diagnostics, writing review, and editing by L.M. Supervision, writing review, and editing by R.-J.H.
Consent for Publication
All authors approved of the article and its submission.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.