
Abstract
In 2012, the number of people infected with human T cell lymphotropic virus type 1 (HTLV-1) was estimated to be 10 million worldwide. Prevalence varies according to geographic location, ethnic factors, sex, age, populations exposed to risk factors, income, and education, reaching countries with the worst socioeconomic scenarios. There is a need to determine the current global prevalence of HTLV-1 and examine its association with countries' human development index (HDI) to provide data for global health policy. Systematic review with meta-analysis is according to PRISMA 2020 recommendations. It was registered at PROSPERO, CRD42021223146. Prevalence or cross-sectional studies of HTLV-1 infection with at least 100 participants, screening, and confirmatory serologic testing were included. Studies with incomplete or unavailable results or with duplicate information were excluded. Data were selected by two independent investigators and analyzed using R software, a metapackage that generated the forest plots [95% confidence interval (CI)]. Heterogeneity was assessed using the I 2 statistic, and funnel plot asymmetry was assessed using Egger's test. Countries were compared using an HDI cutoff ≥0.8. Methodological quality was assessed using Joanna Briggs Institute (JBI) criteria. The overall prevalence of HTLV-1 infection was 0.91% (95% CI: 0.80–1.02, p < .0001) and was higher in low HDI countries [1.18% (95% CI: 1.03–1.34)] than in high HDI countries [0.41% (95% CI: 0.27–0.57)]. Prevalence varied according to the populations studied: it was higher in the general population [1.65% (95% CI: 1.08–2.34)] compared to pregnant women [0.34% (95% CI: 0.17–0.57)] and blood donors [0.04% (95% CI: 0.01–0.08)]. Consistently, prevalence for each population group was higher in low HDI countries than in high HDI countries. The worldwide prevalence of HTLV-1 infection is highly heterogeneous, with a global prevalence of 0.91%. In high HDI countries, the observed prevalence is approximately three times lower than in low HDI countries. In the general population, the observed prevalence is about 5 times higher than in pregnant women and 41 times higher than in blood donors.
Introduction
Human T cell lymphotropic virus type 1 (HTLV-1) was described in 1980 as the first retrovirus associated with human disease. The virus is transmitted through unprotected sexual intercourse, contact with infected blood or tissue, and vertically. 1,2 Most of the population is unaware of the virus and it is considered a neglected infection/disease. 3 HTLV-1 is the causative agent of adult human T cell lymphoma/leukemia, 4,5 HTLV-1-associated myelopathy or tropical spastic paraparesis 6 HTLV-1-associated uveitis, 7 and infective dermatitis. 8 In addition, the virus is associated with other neurologic, ophthalmologic, dermatologic, and urologic clinical manifestations. 9,10
It is estimated that at least 10 million people worldwide are infected with HTLV-1. HTLV-1 is endemic in Japan, sub-Saharan Africa, South America, the Caribbean, Iran, and Melanesia. 11,12 Prevalence varies by geographic region, sociodemographic characteristics, ethnicity, and certain at-risk groups such as injection drug users, sex workers, and HIV carriers. 12,13 HTLV-1 prevalence increases with age and is higher among women, people with low income, and low education levels. 11,14 These are the social determinants of health that are considered in the calculation of the human development index (HDI). This index measures and monitors the quality of human life and changes in the socioeconomic patterns of a given society. The HDI is also a reference for measuring the response of countries to public policies such as prevention and health promotion. 15,16 The score ranges from 0 to 1, and the lower a country's score the worse the living conditions of its population. 15
Population-based studies are more accurate in identifying health status indicators. 17 However, most studies assessing the prevalence of HTLV-1 have been conducted in specific groups such as pregnant women, blood donors, or hospitalized patients. 1,12,18 These groups do not reflect the epidemiologic profile of the general population, leaving a gap in the true prevalence of HTLV-1 in the world. 1,18,19 Despite numerous prevalence studies conducted to date, it has not been possible to find a systematic review with meta-analysis that would be able to summarize the known data on worldwide prevalence and determine the accuracy of this estimate. Also, no study was found linking the prevalence of HTLV-1 to the HDI of countries.
Given the heterogeneity of the prevalence of HTLV-1 in the global population and in specific populations, this study aims to estimate the global prevalence of HTLV-1 infection and assess its association with the HDI of countries.
Methods
Study design, protocol, and registry
This is a systematic review with meta-analysis based on the selection of cross-sectional studies that report the prevalence of people infected by HTLV-1. The survey was structured according to PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 20 and registered at the PROSPERO center (International Prospective Register of Systematic Reviews) under the registration number: CRD42021223146.
Criteria eligibility
Studies of the prevalence of HTLV-1 infection, cross-sectional studies with at least 100 participants, and serologic screening tests: enzyme-linked immunosorbent assay, particle agglutination, or chemiluminescence test and confirmatory tests; western blot, immunofluorescence, and/or polymerase chain reaction were included. Articles with incomplete data, duplicate samples, experimental studies in animals, and articles without access to data were excluded after a thorough search.
Sources of information and searches
Before starting the database search, the Cochrane Library database was searched for the presence of a systematic review on the topic of this review, but no entry was found. The electronic data sources consulted were MEDLINE/PubMed, CAPES/Embase Platform, Cochrane Library, LILACS indexed in the Virtual Health Library, Scopus, and Google Scholar. A manual search was then performed by checking the bibliographic references of the studies included in the review.
Descriptor searches were performed in medical subject headings (MeSH), health sciences descriptors, and basic subject headings (Emtree Terms) using the descriptors: human T-lymphotropic virus 1/HTLV-1 infections; prevalence; and cross-sectional studies. Applied to the combination of Boolean operators OR and AND, human studies, with no restriction on language or year of publication.
Defined search strategy
The syntax of the search strategy in each database:
BVS/Lilacs, on March 13, 2022, at 23:04, with 2.718 articles: (Human T-lymphotropic virus 1) OR (HTLV-I Infections) AND (Prevalence) AND (Cross-Sectional Studies).
Embase, on March 13, 2022, at 09:43, with 118 articles: (“human t-lymphotropic virus 1”/exp OR “htlv-1 infection”/exp) AND “prevalence”/exp AND “cross- sectional study”/exp AND [base]/lim.
Scopus, on March 13, 2022, at 10:54, with 233 articles: (TITLE-ABS-KEY (human AND t-lymphotropic AND virus 1) OR TITLE-ABS-KEY (HTLV-I AND infections) AND TITLE-ABS-KEY (prevalence) AND TITLE-ABS-KEY (cross-sectional AND studies)).
Cochrane, on March 13, 2022, at 20:00, with 38 articles: Human T-lymphotropic virus 1 in Title Abstract Keyword OR HTLV-I Infections in Title Abstract Keyword AND Prevalence in Title Abstract Keyword AND Cross-Sectional Studies in Title Abstract Keyword—(Word variations have been searched).
PubMed, on March 13, 2022, at 00:10, with 507 articles:
((“Cross-Sectional Studies”[Mesh]) OR (Cross-Sectional Studies) OR (Cross-Sectional Study) OR (Studies, Cross- Sectional) OR (Study, Cross-Sectional) OR (Cross Sectional Analysis) OR (Analyses, Cross Sectional) OR (Cross Sectional Analyzes) OR (Disease Frequency Surveys) OR (Cross-Sectional Survey) OR (Cross Sectional Survey) OR (Cross-Sectional Surveys OR (Survey, Cross-Sectional) OR (Surveys, Cross-Sectional) OR (Surveys, Disease Frequency) OR (Disease Frequency Survey) OR (Survey, Disease Frequency) OR (Analysis, Cross-Sectional) OR (Analysis, Cross-Sectional) OR (Analysis, Cross Sectional) OR (Cross-Sectional Analysis) OR (Cross-Sectional Analysis) OR (Prevalence Studies) OR (Prevalence Study) OR (Studies, Prevalence) OR (Study, Prevalence)) AND ((prevalence [MeSH])) AND ((“HTLV-I Infections”[Mesh]) OR (Infections, HTLV-I) OR (HTLV-I Infection) OR (Infection, HTLV-I) OR (Infections, HTLV I) OR (Human T-lymphotropic Virus 1 Infections) OR (Human T lymphotropic Virus 1 Infections) OR (Human T-lymphotropic Virus 1 Infection) OR (Human T lymphotropic Virus 1 Infection) OR (“Human T-lymphotropic virus 1”[Mesh]) OR (Human T lymphotropic virus 1) OR (HTLV-I) OR (HTLV-1))
Identification and selection of studies
Electronic searches were performed starting on December 10, 2020 and updated on March 13, 2022 to search for new articles published during this time period. Studies were selected independently and simultaneously by two investigators (G.C.L.S., J.R.R.); disagreements were resolved by consensus in the presence of two additional investigators (K.N.S. and C.M.C.C.D.). Data sets were prescreened after reading the titles and abstracts of each article to identify studies that met the inclusion criteria. Subsequently, the articles were read in full to ensure that the eligibility criteria were met. This completed the phase of including studies in the systematic review. The screening and selection of studies were performed using Rayyan® reference manager software. 21
Data extraction
Data from the selected studies were entered into a Microsoft Excel 2010 spreadsheet. Characteristics extracted from the studies included DOI, author(s) name, year of publication, country/region where the study was conducted, HDI, objective, screening population, sex, skin color, socioeconomic level, education level, coinfections, sample size, serologic test (screening and confirmatory test for HTLV-1), prevalence with 95% confidence interval (95% CI), and conclusion.
Assessment of the quality of articles
The Joanna Briggs Institute (JBI) critical appraisal tool for systematic reviews of studies reporting prevalence data were used to assess the quality of the studies. 22,23 The tool contains 9 questions to be answered “yes,” “no,” “confused,” or “not applicable,” with only “yes” responses being scored. Scores can range from zero to nine. Regardless of the score obtained in the quality assessment, items were not excluded because they are a parameter for analyzing heterogeneity, as there is no set threshold for this instrument.
Synthesis and analysis of the data
Estimation of prevalence
The estimate of global HTLV-1 prevalence was calculated using the population size of countries, according to the prevalence in eligible studies in the general population. To minimize potential barriers to accessing information on the global prevalence of HTLV-1, the authors show the prevalence calculation by country and continent.
Association between HTLV-1 prevalence and HDI
To relate the prevalence of HTLV-1 and the HDI of countries, studies were divided into high HDI (HDI ≥0.8) and low HDI (HDI <0.8) countries according to the United Nations Development Program (UNDP) classification (
Because of the different sample sizes of the studies, the unique proportions model with random effects was applied, we used the Freeman-Tukey double-arcsine transformation (PFT) to stabilize the variance and achieve an approximate normal distribution of the studies, prevalence was globally weighted, and HTLV-1-evaluated populations were calculated. The PFT is defined by the following equation:

xi represents the number of events (infected by HTLV-1) and in the total number of individuals. 25
The I 2 test was used to assess the significance of heterogeneity, which indicates the proportion of variability between studies. 27,28 The variance was calculated by the value of Q, defined as:
Wi is the weight of study i (W i = 1/Viy ), Yi is the measure of the effect of study i, M is the summary effect, and k is the number of studies. 25
Data were represented by a forest plot with the respective 95% confidence intervals (95% CI), and Egger's regression test and funnel asymmetry plot 29 were used to assess the risk of publication bias when the p value <.05.
Results
Selection of studies
Of the total 4.472 articles found by searching the electronic databases, duplicates and irrelevant publications and articles were excluded according to the eligibility criteria. The final selection of 86 publications was included in the systematic review with meta-analysis, Figure 1.
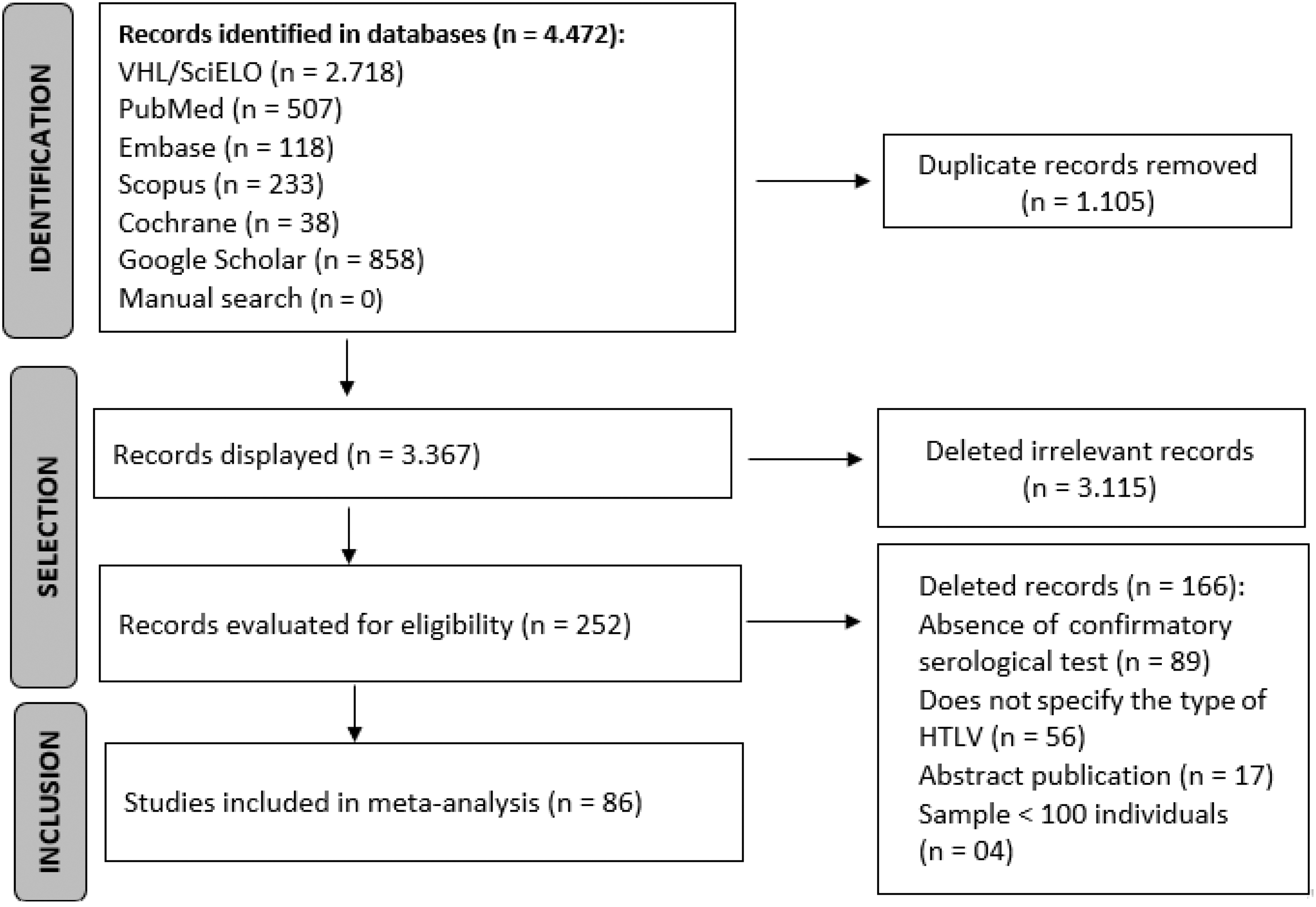
PRISMA 2020 flowchart of studies selected for systematic review with meta-analysis.
Characteristics of the studies
The general characteristics and prevalence of HTLV-1 infection of the studies are listed in alphabetical order of the countries and year of publication of the studies (Table 1). Of the total number of articles: 84 were published in English, one in French, and one in Dutch between 1991 and 2022. The populations studied were 28 in the general population, 15 in blood donors, 13 in pregnant women, and the other 30 studies were found in different populations (illicit drug users, persons with HIV and STIs, sex workers, men who have sex with men, prison inmates, and hospital patients). Study sample sizes ranged from 125 to 4.497.616 persons, and prevalence ranged from 0.0% to 30.3%.
General Characteristics and Prevalence of Human T-Cell Lymphotropic Virus Type 1 Infection of Studies Included in Systematic Review with Meta-Analysis, 1991–2022
Test screening; **Confirmatory test; ***JBI score.
ELISA, enzyme-linked immunosorbent assay; HIV, human immunodeficiency virus; IF, immunofluorescence; PA, particle agglutination; PCR, polymerase chain reaction; JBI, Joanna Briggs Institute/methodological quality assessment score; MSM, men who have sex with men; STI, sexually transmitted infections; WB, western blot.
Figure 2 shows the geographical distribution and the HDI ranking of the selected studies in 27 countries. The studies were published in South America: 27 in Brazil, 11,37 –60,62 5 in Argentina, 30 –34 4 in Peru, 106 –109 4 in Colombia, 65 –68 1 in Guyana French 81 and 1 in Suriname 113 ; followed by Asia: 11 in Iran, 85 –95 3 in Japan, 97 –99 2 in China, 63,64 1 in India, 84 1 in Mongolia 102 and 1 in Taiwan. 114 In Europe: six in Spain, 69 –74 one in Holland, 83 one in Italy, 96 one in the United Kingdom, 110 one in Switzerland, 112 and one in Sweden. 111 In Africa: three in Gabon, 78 –80 one in Benin, 36 one in Guinea, 82 one in Mali, 100 one in Mozambique, 101 and one in Nigeria. 103 To a lesser extent in North America with three studies in the USA 75 –77 and in Oceania with two studies in Papua New Guinea 104,105 and one in Australia. 35
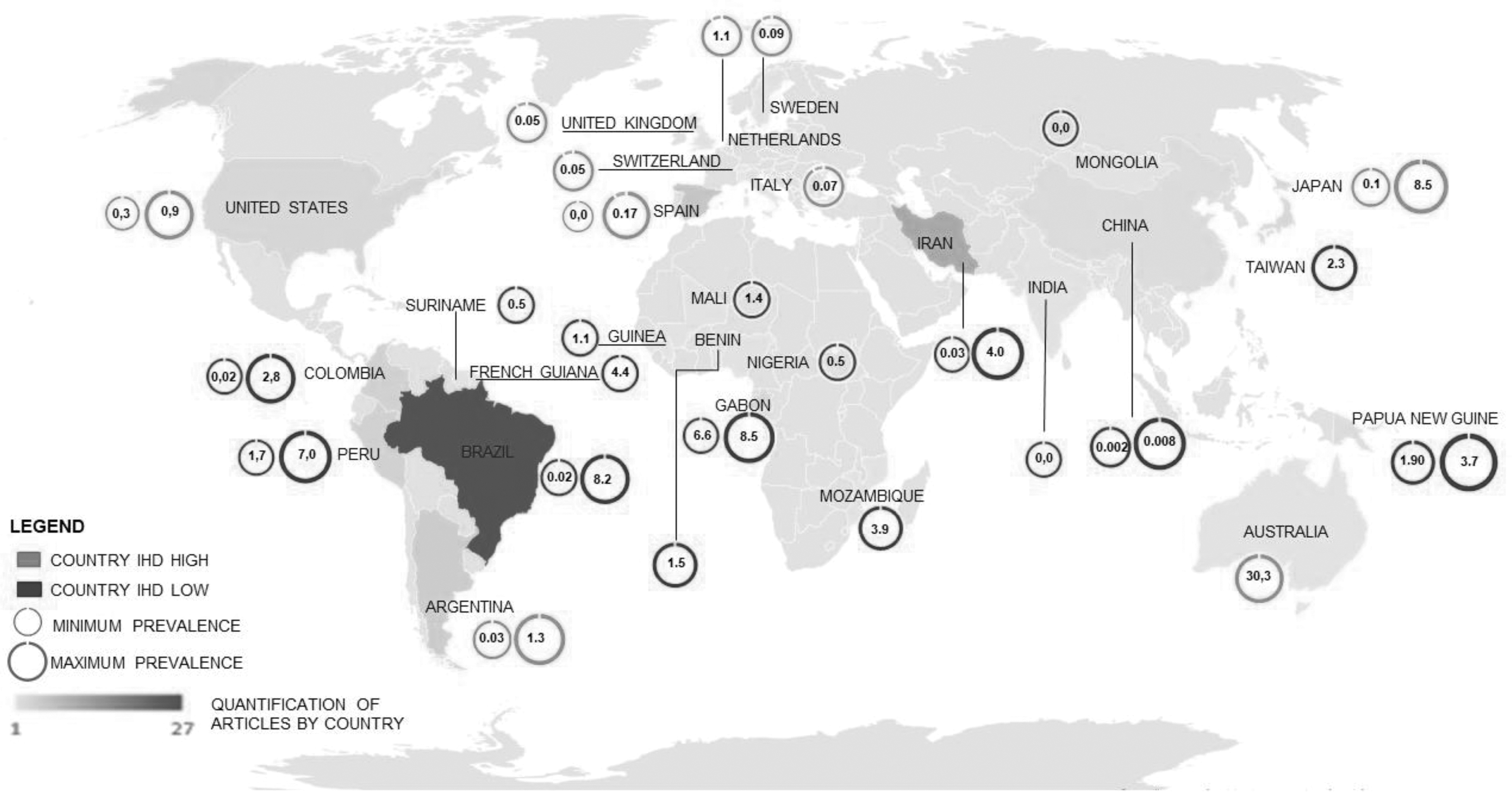
Minimum and maximum prevalence of HTLV-1 in countries according to HDI high ≥0.8 and low <0.8. Image created by authors using Microsoft Office 365 program: Excel and PowerPoint. HDI, human development index; HTLV-1, human T-cell lymphotropic virus type 1.
The HDI of each country was taken from the UNDP 2020, 24,115 except for French Guiana, a single French territory not included in the UNDP report, so the value of 0.739 was included. 116 Studies were divided into high HDI ≥0.8 and low HDI <0.8 countries, with 73% of studies conducted in low HDI countries.
Evaluation of the methodological quality of the study
The methodological rating of the studies ranged from five to nine points. Eighteen percent of the studies achieved the maximum score of nine points and 65% achieved a score between seven and eight. Of the 15 studies that received a score between five and six points, 12 were published before 15 years (≤2006
Overall analysis of the 86 studies included in the meta-analysis, with a sample size of 10.186.638 individuals, 5.776 of whom were infected with HTLV-1, yielded an overall prevalence of 0.91% (95% CI: 0.80–1.02). A large heterogeneity was observed between studies (I 2 = 99%), showing a significant difference in prevalence between study subgroups in countries with a high HDI of 0.41% (95% CI: 0.27–0.57) and in countries with a low HDI of 1.18% (95% CI: 1.03–1.34), Figure 3.

Prevalence of individuals infected with HTLV-1 in the forest plot of the 86 studies included in the meta-analysis according to the classification of countries with high HDI ≥0.8 and low HDI <0.8.
Analysis of HTLV-1 prevalence in specific groups
This analysis included 57 studies, including 15 studies in blood donors 0.04% (95% CI 0.01–0.08; I 2 = 100%), 13 studies in pregnant women 0.34% (95% CI: 0.17–0.57; I 2 = 98%), and 28 studies in the general population 1.65% (95% CI: 1.08–2.34; I 2 = 98%), Figure 4.
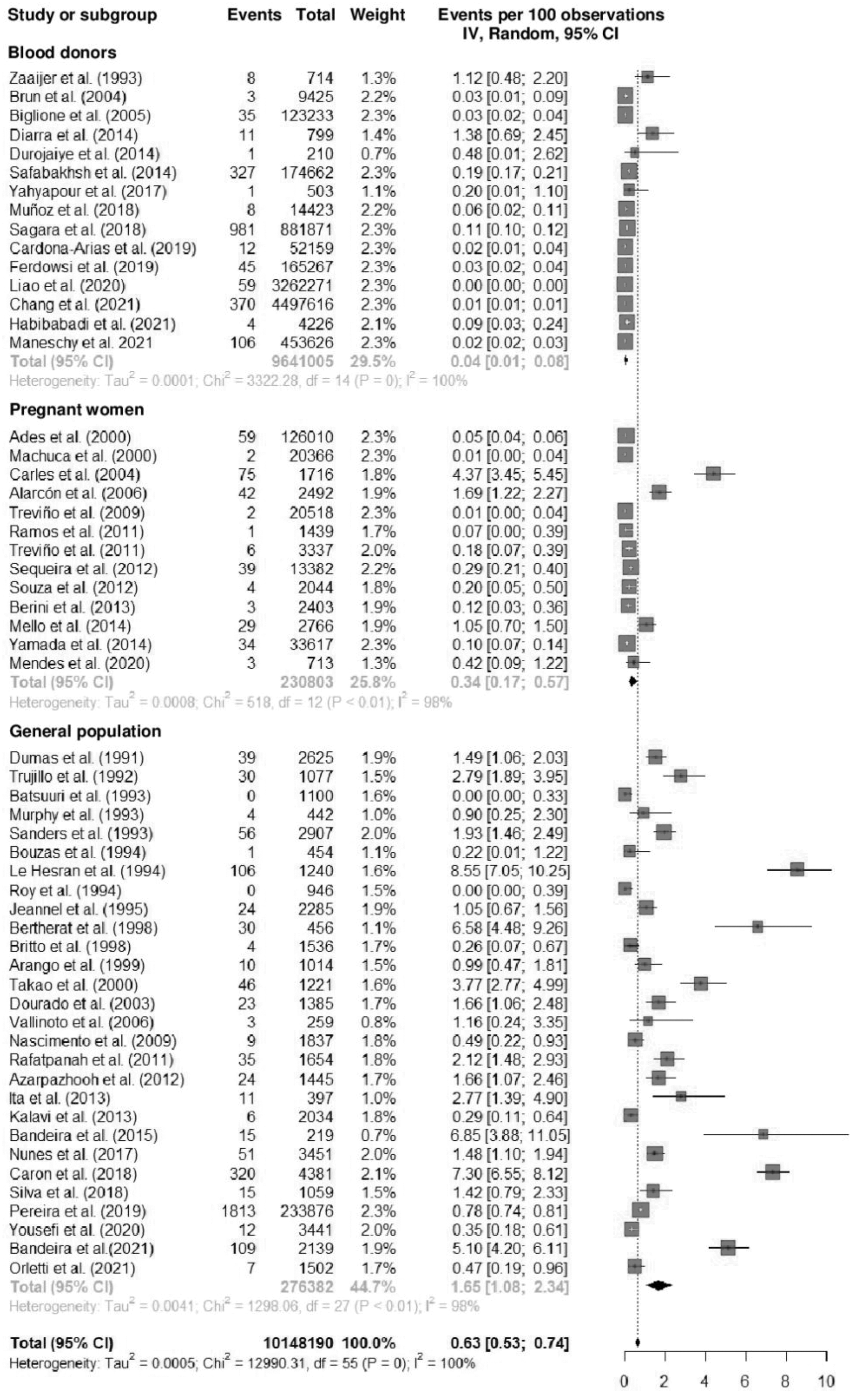
Prevalence of HTLV-1-infected individuals in 57 studies in the specific groups: blood donors, pregnant women, and the general population.
Twenty-eight studies in the general population were distributed among continents (Africa, South America, Asia, North America, and Oceania), 50% of the articles were published in South America, with the prevalence 1.45% (95% CI: 0.89–2.14; I 2 = 95%). The highest prevalence was in the African continent 4.36% (95% CI: 1.55–8.47; I 2 = 99%) and Oceania 2.74% (95% CI: 1.21–4.84; I 2 = 91%), Figure 5.
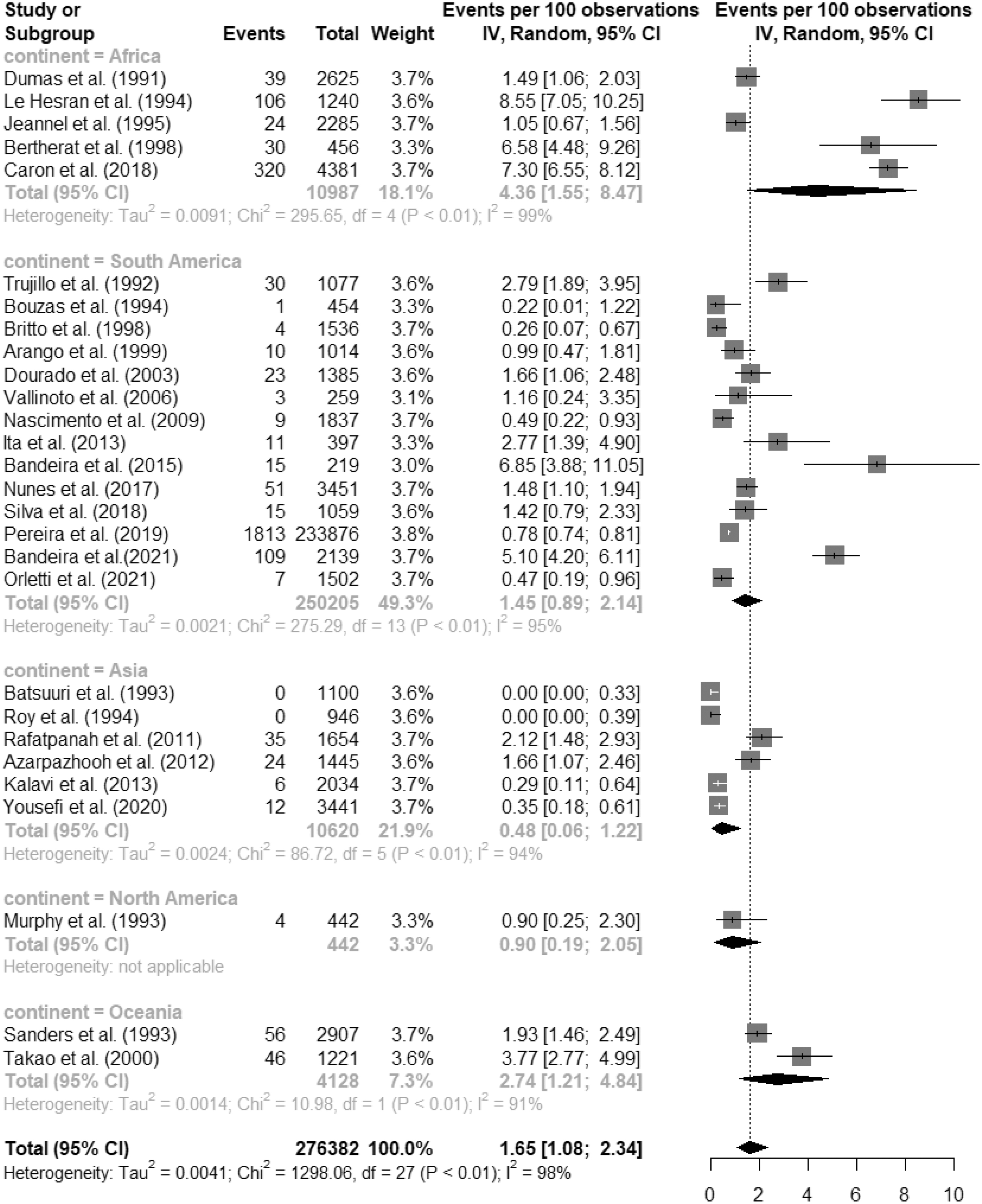
Prevalence of HTLV-1-infected individuals in the general population by continent.
These studies were published in 12 countries, 36% of them in Brazil with a prevalence of 1.44% (95% CI: 0.79–2.28; I 2 = 96%). The highest prevalences were found in Gabon 7.53% (95% CI: 6.67–8.44; I 2 = 25%), Peru 2.77% (95% CI: 1.35–4.65), and Papua New Guinea 2.74% (95% CI: 1.21–4.84; I 2 = 91%), Figure 6.
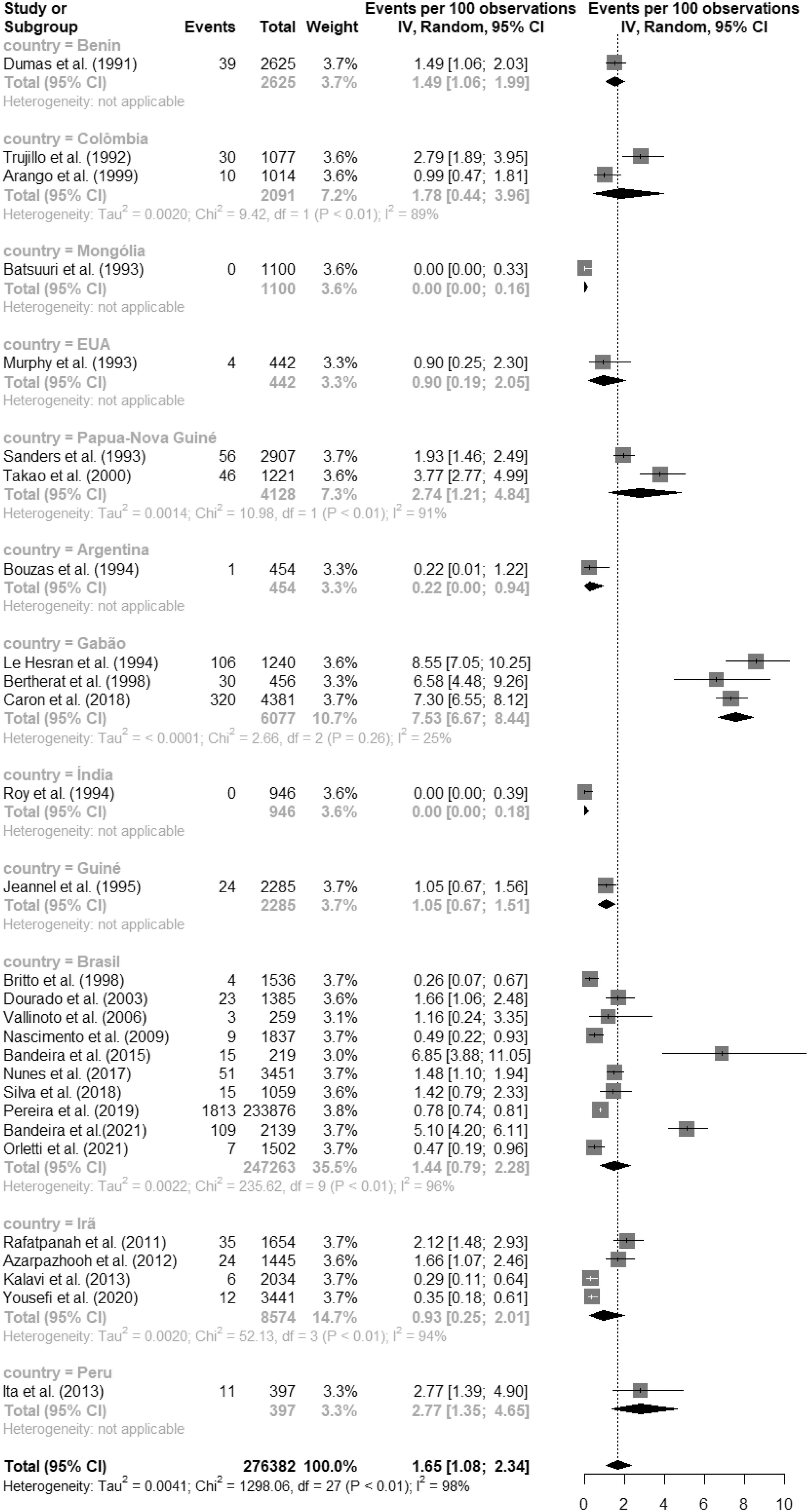
Prevalence of HTLV-1-infected individuals in the general population by country.
Analysis of the prevalence of HTLV-1 in specific groups by high and low HDI countries
In studies of blood donors, the prevalence was 0.08% (95% CI: 0.02–0.18; I 2 = 98%) in high HDI countries and 0.02% (95% CI: 0.00–0.05; I 2 = 99%) in low HDI countries. In studies of pregnant women, the prevalence was 0.05% (95% CI: 0.02–0.09; I 2 = 86%) in high HDI countries and 1.03% (95% CI: 0.29–2.19; I 2 = 97%) in low HDI countries. In studies of the general population in high HDI countries, it was 0.51% (95% CI: 0.04–1.37; I 2 = 43%) and 1.75% (95% CI: 1.14–2.49; I 2 = 98%) in low HDI countries, Figure 7.
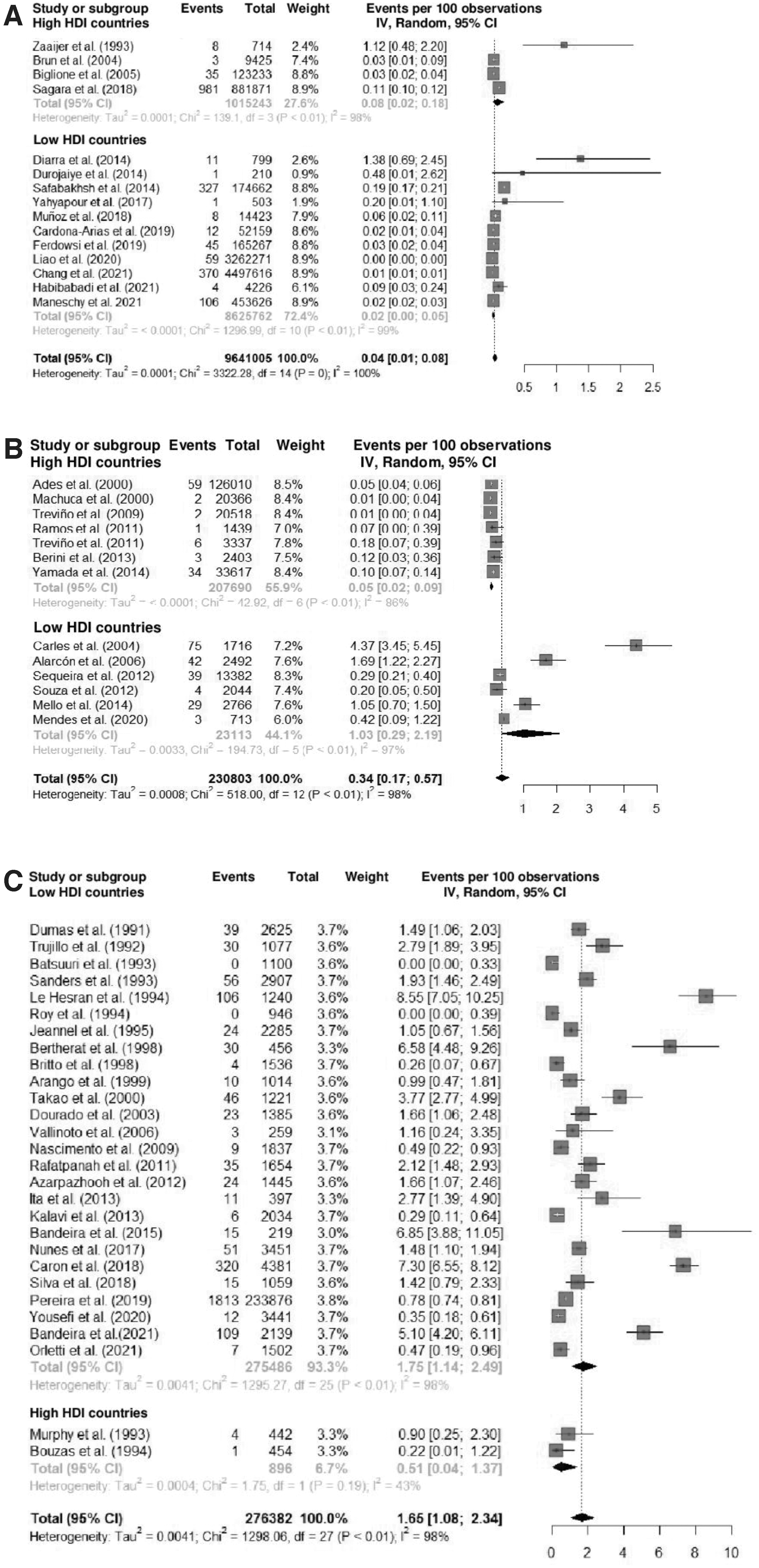
Prevalence of individuals infected by HTLV-1 according to HDI ≥0.8 and HDI <0.8 in population-based screening studies:
Publication bias
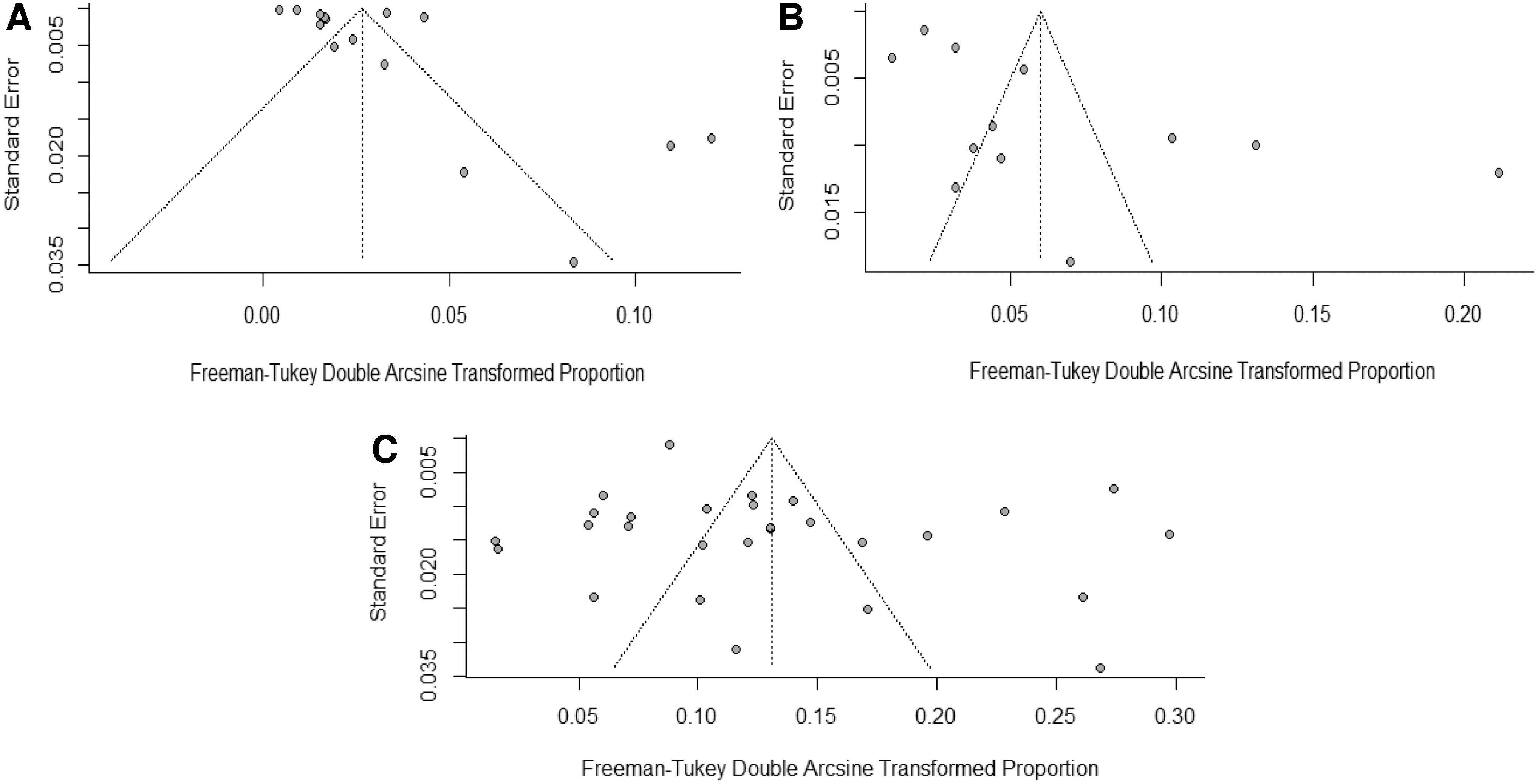
Publication bias was assessed using the funnel plot and Egger's linear test for the studies included in the meta-analysis. The data are distributed in the graph, Figure 8, which has an asymmetric format (p < .0001). To determine the possible cause of the large heterogeneity in the prevalence of HTLV-1, an analysis was performed according to the groups of blood donors (p = .103), pregnant women (p = .019), and the general population (p = .025), Figure 8.
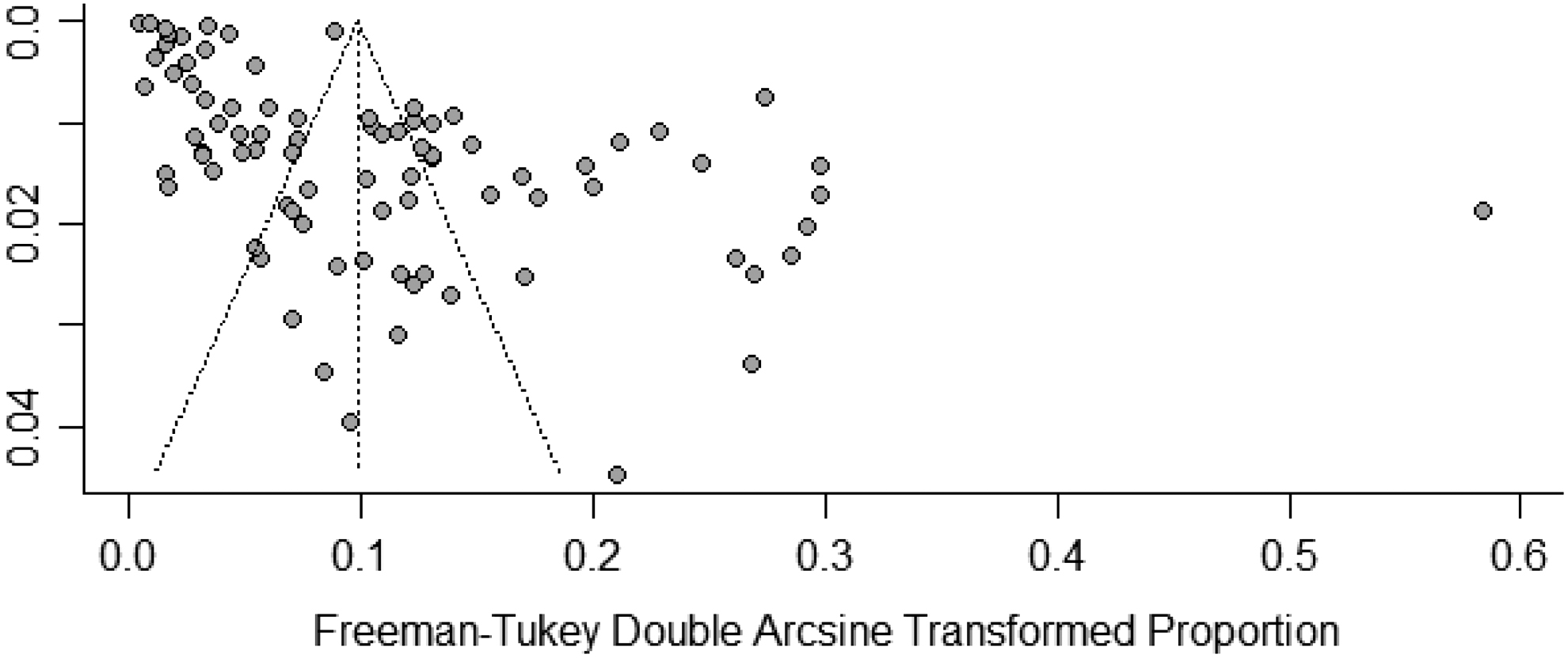
Prevalence of HTLV-1 shown in funnel plot (x-axis) and standard error (y-axis), of the 86 studies included in the meta-analysis.
There is symmetry in the blood donor group and slight asymmetry in the pregnant women and general population groups, resulting in slight publication bias, Figure 9.
Prevalence of HTLV-1 in blood donors
Discussion
In the present meta-analysis, considering 86 eligible studies, the worldwide prevalence of HTLV-1 was estimated to be 0.91%. However, when the 28 studies in the general population were analyzed, the worldwide prevalence of HTLV-1 was estimated to be 1.65%. This calculation was based on a global population of 8 billion in 2022, excluding 36% of the population of China and India 117,118 because there were no studies in China and the prevalence in India was 0%. 84 In this population, the estimated number of people infected with HTLV-1 worldwide is 82.5 million. Based on the methodology used, we estimate the number of people living with HTLV-1 to be higher than that reported in the 2012 study by Gessain and Cassar. 12
The prevalence of HTLV-1 was three times higher in countries with low HDI than in countries with high HDI, consistent with the analysis of groups (blood donors, pregnant women, and the general population). The difference in prevalence may be attributed to the indicators that make up the HDI calculation and supports the findings of studies that associate HTLV-1 seroprevalence with low levels of education, 11,35,48,57,62,85,106,108 low income, 11,35,48,54,57,106 and consequently poorer living conditions. However, two studies that included pregnant women 45,56 found a prevalence of 1.05% and 0.43%, which were not related to education and income, respectively. This divergence confirms that the population studied may bias the results, confirming the need for population-based studies to obtain more accurate prevalence data.
Studies conducted in low HDI countries in South America, 11,37,40,41,45 –48,50,52,54,55,57,58,61,65,66,81,106 –109 Asia, 85,86,90,91,114 Africa, 36,78 –80,82,100,101 and Oceania 104,105 had a prevalence greater than or equal to 1.0% of HTLV-1 infection. However, some studies in Brazil, 38,39,42 –44,49,51,53,56,59,60,62 Colombia, 67,68 Nigeria, 103 Suriname, 113 Iran, 87 –89,92 –95 and China 63,64 revealed a prevalence of <1% of infection by this virus.
In India 84 and Mongolia, 102 the prevalence of HTLV-1 infection was 0.0%, and in China, it ranged from 0.002% to 0.008% in blood donor groups. 63,64 Although China and India are the two most populous countries in the world 118 and belong to an endemic continent, few studies were found. Therefore, considering the lack of studies on the prevalence of HTLV-1 in these countries, the high population density, and the lack of specificity of the confirmatory test, it is essential to conduct large-scale epidemiologic studies in countries with lower socioeconomic conditions before considering the rare prevalence of HTLV-1.
Studies conducted in high HDI countries in North America, 75 –77 and Europe, 69 –74,96,110 –112 as well as in countries such as Japan 98,99 and Argentina found a prevalence of HTLV-1 infection of <1.0%. However, some studies in countries with high HDI have exceptionally found a prevalence of infection >1%. 33,35,83,97 The higher prevalence may be explained by the characteristics of the population studied and the year of the study. The study conducted in Argentina 33 examined five high-risk groups: injecting drug users, sex workers, men who have sex with men, patients with tuberculosis, and people with an STI diagnosis and found a prevalence of 1.3% for HTLV-1 infection.
The first large-scale epidemiologic study conducted in Australia among Australian Aborigines found a high prevalence of HTLV-1, 30.3%. 35 This population accounts for 3.3% of the Australian population and lives in an isolated and marginalized community. The unfavorable socioeconomic situation of this population and the lack of public health strategies to better control HTLV-1 transmission could explain the high prevalence of the virus in this community. 119 Another study conducted in the Netherlands examined immigrants from Suriname and the former Netherlands Antilles, where HTLV-1 is endemic. 120 A 1993 study in the Dutch blood donor population 83 found a high prevalence of HTLV-1 (1.1%). At that time, there was no screening for this virus. As a result, the government of this country ordered that all blood donations be screened for HTLV-1 infection for 1 year.
Based on the results of the tests performed, HTLV-1 screening continued, which may explain the control over the spread of the virus. Finally, in a study conducted in 199897 in the cities of Okayama and Gunma, which are not endemic areas for HTLV-I in Japan, a high prevalence of HTLV-1 was found in leprosy patients from two sanatoria, suggesting that HTLV-I infection occurred after patients entered the sanatoria through sexual contact or reuse of needles. Japan, a country with a high HDI, showed the greatest variability in HTLV-1 prevalence between studies (0.1%–8.5%). As known from the past, the country has the largest proportion of people living with HTLV-1 in the world.
However, prevalence has decreased significantly from 1998 to 2018. This is in response to the country's investment in health and its commitment to eliminating the virus with the implementation of several national health policies aimed at identifying the transmission mechanisms of HTLV-1 infection and providing comprehensive care and treatment for associated diseases. 121
In the current study, the prevalence of HTLV-1 infection was lower (0.04) in blood donors than in the general population and in pregnant women. The lower prevalence in blood donors can be explained by the preselection, age (younger), predominance of males, healthier individuals, and consequently less prone to risk behaviors. 122 In the 15 studies conducted with this population, 31,32,59,63,64,67,68,83,89,92,93,95,99,100,103 prevalence ranged from 0.002% in China 63 to 1.4% in Mali. 100 The possible reasons for the difference in prevalence between these two countries are related to Malian health policies, which have weaknesses in blood transfusion safety, and the lack of antibody screening, which is not routinely performed and consequently increases the transmissibility of the virus. 100
Of the 13 studies evaluated in pregnant women in this meta-analysis, 34,43 –45,56,69,70,72,73,81,98,107,110 the prevalence of HTLV-1 was 0.34%, with a range of variation from 0.01% to 4.4%. In countries with low HDI (<0.8), the highest prevalence was in French Guiana, a developing country of African-American descent with high endemicity for HTLV-1. 81 In Peru, the known prevalence is 1.7%, 107 whereas in Brazil, the average prevalence was 0.5%. 43 –45,56 However, researchers in Salvador-Bahia found a prevalence of 1.05% in the pregnant women group. 45 It is known that this state is an endemic region for HTLV 43 ; moreover, it has had a policy of prenatal screening for about three decades. 123
On the contrary, countries with high HDI (≥0.8) have a lower prevalence of HTLV-1. In the UK, 0.05%, 110 in Spain, 0.07%, 69,70,72,73 in Japan, 0.1%, 98 and in Argentina, 0.12%. 34 This finding supports the hypothesis that high HDI is a protective factor, possibly due to greater investment in health policies in these countries.
The prevalence of HTLV-1 in the general population (165 per 10,000 persons) was higher than in the populations of pregnant women and blood donors. Of the 28 studies 11,30,36,39,40,42,46,48,50,53,58,60,65,66,75,78 –80,82,84 –86,88,94,102,104,105,109 conducted in the general population, the prevalence of HTLV-1 ranged from 0.0% to 8.5%. When prevalence was analyzed by continent, the highest prevalence was found in the African continent (4.36%) and the lowest in Asia (0.48%).
Of these studies, 18 (64%) estimated a prevalence of 1.0% or greater, all of which were conducted in countries with low HDI. The highest prevalence of HTLV-1 was found in the following low HDI countries: Gabon, 7.3%, 6.6%, and 8.5%; 78 –80 Brazil, 1.15%, 1.40%, 1.48%, 1.70%, and 6.80%; 11,40,46,48,50 Papua New Guinea, 1.90% and 3.70%; 104,105 Colombia, 1.0% and 2.8%; 65 Peru, 2.80%; 109 Iran, 1.66% and 2.12%; 85,86 Benin, 1.50%; 36 and Guinea, 1.10%. 82 In most of these countries, there are no effective public health measures to prevent infection of vulnerable groups. 124
Despite the heterogeneous distribution of HTLV-1 prevalence worldwide, the studies analyzed in this meta-analysis had robust sample sizes, a narrow confidence interval, and a slight asymmetry in the risk of publication bias. The p-values of the specific groups analyzed (donor blood samples, pregnant women, and the general population) show the measures of reliable effect, lower statistical uncertainty, greater feasibility, and accuracy of the data. 125 In summary, these results point to the need for public health interventions, especially in endemic countries and countries with low HDI.
The limitations of the present study are related to the lack of accurate epidemiological data to calculate the worldwide prevalence of HTLV-1. The gaps identified were few or no population-based studies in high-population countries (China and India), the absence of variables such as socioeconomic status, education level, and health policy, and the lack of dichotomization of the HDI (high and low HDI countries); it is possible that the absence of these data influenced the prevalence estimate.
The perspectives of this study encourage government agencies to pursue consistent public health policies that focus on high-risk groups, particularly in low-HDI countries in endemic areas. To curb the increase in transmission and virus-related diseases, epidemiologic research in countries such as India and China should be strengthened to determine the true prevalence in these countries. Thus, the current study can contribute to the development and application of clinical protocols and guidelines for the comprehensive treatment of people with HTLV-1, an infection that is a global public health problem.
Conclusion
The worldwide prevalence of HTLV-1 is heterogeneous, with an estimated weighted prevalence of 0.91%. In high HDI countries, the observed prevalence is approximately three times lower than in low HDI countries. The prevalence of HTLV-1 in the general population is 5 times higher than in pregnant women and 41 times higher than in blood donors.
Footnotes
Acknowledgments
The authors thank the staff of the Integrative and Multidisciplinary HTLV Center of the Escola Bahiana de Medicina e Saúde Pública (EBMSP), the Basic Principles of Retrovirology curriculum component of the graduate course, the GEPFIR (Research Group on Cardiovascular and Respiratory Physiotherapy) of the EBMSP. We are also grateful for the support we received from EBMSP through a partial scholarship in the master's course for the author G.C.L.S. Coordination for the Improvement of Higher Education Personnel (CAPES) and Foundation for Research Support of the State of Bahia (FAPESB) through a scholarship in the Master's Degree in Health Technologies—EBMSP for the author J.R.R.
Authors' Contributions
C.M.C.C.D.: designed and supervised the work; K.N.S. cosupervised the work; G.C.L.S. and J.R.R.: acquired the data; G.C.L.S. and C.M.C.C.D.: wrote the first version; G.C.L.S., N.B.-S., B.G.-C., M.F.R.G., K.N.S., C.M.C.C.D., and C.N.d.A.: critical review of the article. All authors read and approved the final version of the article, analyzed and interpreted the data, and wrote the article.
Availability of Data and Material
All data generated or analyzed are included in this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The National Foundation for the Development of Private Higher Education (FUNADESP) granted K.N.S., C.M.C.C.D., M.F.R.G., N.B.-S., and B.G.-C. M.F.R.G. and B.G.-C. also were granted by the Brazilian National Research Council (CNPq) for financial support.
Supplementary Material
Supplementary Annex
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.