
Abstract
Clinical management and optimal treatment are essential to improving outcomes for people living with HIV (PLWH). We assessed trends and outcomes of chronic kidney disease (CKD) in PLWH in a resource-limited center of central China. All PLWH who were followed up in a tertiary referral center in Wuhan, China, from July 2016 to June 2021 were evaluated. CKD was defined as glomerular filtration rate (GFR) <60 mL/min/1.73 m2 during two consecutive measurements 3 months apart. Baseline characteristics of the participants were extracted from the hospital medical records. The prevalence rate and associated risk factors of CKD were analyzed. A total of 863 PLWH with normal kidney function at baseline were analyzed. The median age was 33 (interquartile ranges: 26–49) years, and 778 (90.2%) were male and 85 (9.8%) were female. Among them, 50 (5.8%) had their GFR falling below 60 mL/min/1.73 m2 after a median of 54 months. Adjusted multivariate logistic regression revealed older age [adjusted odds ratio (aOR) = 1.04, 95% confidence interval (95% CI): 1.01–1.07], female sex (aOR = 3.17, 95% CI: 1.14–8.84), lower body weight (aOR = 0.95, 95% CI: 0.91–1.00), lower hemoglobin (aOR = 3.54, 95% CI: 1.51–8.30), longer duration of antiretroviral therapy exposure (aOR = 1.02, 95% CI: 1.00–1.04), and a baseline GFR between 60 and 90 mL/min/1.73 m2 (aOR = 3.89, 95% CI: 1.21–12.46) were associated with the development of CKD. Our findings showed that CKD is not infrequent in PLWH with a combination of traditional and HIV-specific risk factors for kidney disease, highlighting the suboptimal monitoring and treatment options of CKD in PLWH in resource-limited settings. Scalable monitoring strategy to improve care for this population is warranted.
Introduction
Chronic kidney disease (CKD) is one of the most important noninfectious comorbidities (NICMs) observed in people living with HIV (PLWH), both in developed countries and in resource-limited settings. 1,2 Once established, CKD usually progresses, and may result in end-stage renal disease (ESRD), where a patient's outcomes will depend on the accessibility of dialysis or kidney transplantation. 3 The prevalence of CKD in PLWH continues to increase, despite antiretroviral therapy (ART). 4 While it has long been recognized that HIV infection is a risk factor for CKD, it remains important to consider that the causes of kidney diseases affecting PLWH have changed over time. During the pre-ART era, HIV-associated renal conditions and opportunistic infection-related acute kidney injury were predominate, whereas CKD in the ART era is mainly related to NICMs caused by diabetes and hypertension. 5
The burdens of renal diseases 6 include ART exposure, aging, and being of African descent. 7 These changes have led to new considerations for PLWH, including models of care, access to care in resource-limited settings, polypharmacy, and geriatric-specific considerations. As a consequence of renal disease in PLWH, the need for dialysis and kidney transplantation has increased. However, information on CKD outcomes and management in PLWH in China is lacking, especially in resource-limited region. 8,9 To this end, we assessed the frequency and development of CKD in PLWH of a resource-limited region in China, with a focus on the challenges to deliver optimal care for PLWH.
Materials and Methods
Participants' characteristics and data collection
From July 2016 to June 2021, the medical records of PLWH (≥18 years of age at enrollment) who received care at a single center, Zhongnan Hospital of Wuhan University, one of the largest referral hospitals for HIV/AIDS care in Hubei Province, central China, have been evaluated.
Age, sex, body weight, nadir and current CD4+ T cell counts, HIV plasma viral load (VL), ART history, sulfamethoxazole/trimethoprim (SMZ-TMP) utilization, World Health Organization (WHO) HIV/AIDS clinical stage, creatinine (Cr), total cholesterol, triglycerides, fasting blood glucose, and hemoglobin were collected. Co-infection with hepatitis B virus (HBV) and hepatitis C virus (HCV) was recorded. History of or current diabetes and arterial hypertension were also recorded. Participants were not included in this analysis if their first estimated glomerular filtration rate (eGFR) measure was <60 mL/min/1.73 m2 (Fig. 1). Since data on height were lacking in our cohort, body mass index (BMI) could not be calculated, and as neither urine dipsticks nor standard urine tests were routinely performed at our center, these data were also unavailable.
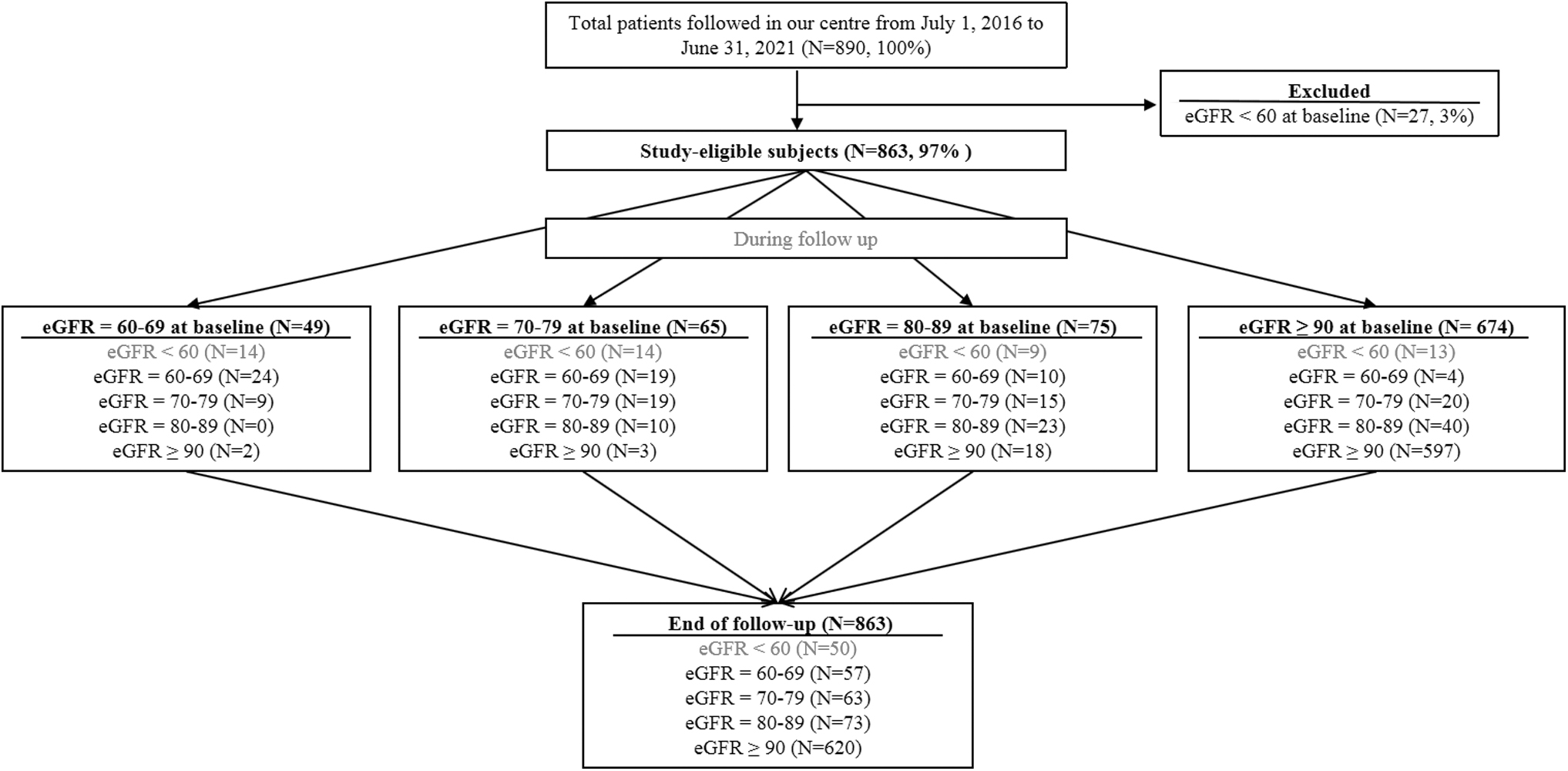
Development of the study cohort.
Ethical consideration
This clinical study was conducted according to the principles expressed in the Declaration of Helsinki. All participants provided signed informed consent when enrolling in the study. The Ethical approval was granted by the Ethics Committee of Zhongnan Hospital of Wuhan University (No. 2021003).
Study definitions
Participants were considered to be in care for each calendar year after enrollment if there was a lack of documented death or loss to follow-up (LTFU, defined as not being seen at the clinic >12 months after their last visit). In case of death or LTFU, participants were considered to be in care for the year of their last clinic visit. Participants were considered on ART as indicated on their clinical chart regardless of the type of antiretroviral drugs. Participants were considered to have been monitored for treatment failure and kidney function if they had received at least one VL test and Cr test during follow-up.
Since the detection threshold for the resistance testing of HIV in China is ≥1,000 copies/mL, we selected VL of ≥1,000 copies/mL as our virologic failure marker. As baseline VL was not a routine clinical test before 2020 in our center, these data were not included in the study. CKD was defined as an eGFR of <60 mL/min/1.73 m2 based on the Modification of Diet and in Renal Disease (MDRD) formula for at least 3 months, as proposed by Barraclough et al, 10 and other studies from mainland China, 8,9 Taiwan, 11 or Hongkong 12 on the preferential use of the MDRD formula in the treated HIV population. Also, the Cr in our center was measured using Jaffe assay, whereas the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula was better validated with enzymatic assays. 13,14
ART drugs that are available free of charge in our province include tenofovir disoproxil fumarate (TDF), zidovudine, abacavir, lamivudine, nevirapine, efavirenz, and lopinavir/ritonavir (LPV/r). To get access to integrase inhibitors (INIs) such as raltegravir, elvitegravir, or dolutegravir, PLWH had to purchase them. Other drugs such as stavudine and indinavir were no longer used in China at the time of the study.
Monitoring for kidney function and GFR calculation
The MDRD formula was used to generate the GFR of all participants. The MDRD formula is as follows: GFR = 186 × serum creatinine (mg/dL)−1.154 × [age (years)]−0.203 × [0.742 if female]. Renal function was evaluated according to the staging system of the Kidney Disease Outcomes Quality Initiative (K/DOQI). 15 Baseline Cr results were obtained before ART initiation. After ART initiation, if participants had multiple documented Cr results, the last test result within the observation period was used.
Statistical analyses
Categorical variables were presented as numbers and percentages, and continuous variables were described using medians and interquartile ranges (IQR). Pearson's chi-squared test and the Wilcoxon test were used for comparison between groups. Risk factors for GFR <60 mL/min/1.73 m2 were assessed by logistic regression models. Statistically significant variables in univariate analysis were included in the multivariate model. All p values were two sided, and p < .05 was considered statistically significant. We used SPSS 23.0 to perform all statistical analyses.
Results
Characteristics of the study population at baseline
Between July 2016 and June 2021, a total of 890 PLWH were followed in our center. Among them, 27 PLWH (3%) had a GFR <60 mL/min/1.73 m2 at baseline and were excluded from the study. The 863 PLWH with baseline GFR >60 mL/min/1.73 m2 were included and their median age was 33 (IQR: 26–49) years, 778 (90.2%) were male and 85 (9.8%) were female. Their median body weight was 64 kg (IQR: 57–73), and the majority (63.7%) of participants had body weight >60 kg. The median CD4+ cell count at baseline was 257 cells/μL (IQR: 121–383), and 61.4% had CD4+ cell count >200 cells/μL. Most participants (58.1%) were classified as WHO clinical stage 3 or 4. Seropositivity for HBV or HCV co-infection was 7.2% and 5.0%, respectively.
The median hemoglobin level was 143 g/L (IQR: 125–153), and 78.8% had hemoglobin >120 g/L, with a sex difference for hemoglobin values (p < .001). The median fasting blood glucose level was 5.1 mmol/L (IQR: 4.7–5.5), with 9.7% of participants >6.1 mmol/L. The median serum triglyceride level was 1.2 mmol/L (IQR: 0.9–1.7), with 24.9% of participants >1.70 mmol/L. The median serum cholesterol level was 3.8 mmol/L (IQR: 3.3–4.4), with 8.7% of participants >5.1 mmol/L (Table 1).
Demographic and Clinical Characteristics of People Living with HIV With and Without Chronic Kidney Disease
The bold values are <0.05.
Parameters at the end of the follow-up.
Including 12 at baseline and 19 at the end of the follow-up.
Including 15 at baseline and 31 at the end of the follow-up.
ART, antiretroviral therapy; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; HBV, hepatitis B virus; HCV, hepatitis C virus; IQR, interquartile ranges; TMP-SMZ, trimethoprim/sulfamethoxazole; WHO, World Health Organization.
Characteristics of the study population during follow-up
Among the 863 participants with baseline GFR >60 mL/min/1.73 m2, 239 (27.7%) had been treated with SMZ-TMP during follow-up. The duration of ART spanned from 3 to 60 months, and 622 (72.1%) had a TDF-based regimen (Fig. 2). At the end of follow-up, 50 (5.8%) of the 863 participants had the GFR <60 mL/min/1.73 m2 after a median of 54 months (IQR: 23–58) of ART. The mean age of these 50 participants was 52 (IQR: 42–67) years, and 50% were older than 50 years. There were 39 (78%) male and 11 (22%) female participants. Their median body weight was 58 kg (IQR: 49–65), and the majority (62%) of participants had body weight ≤60 kg. The median CD4+ cell count at baseline was 133 cells/μL (IQR: 18–208), and only 24% had CD4+ cell count >200 cells/μL.
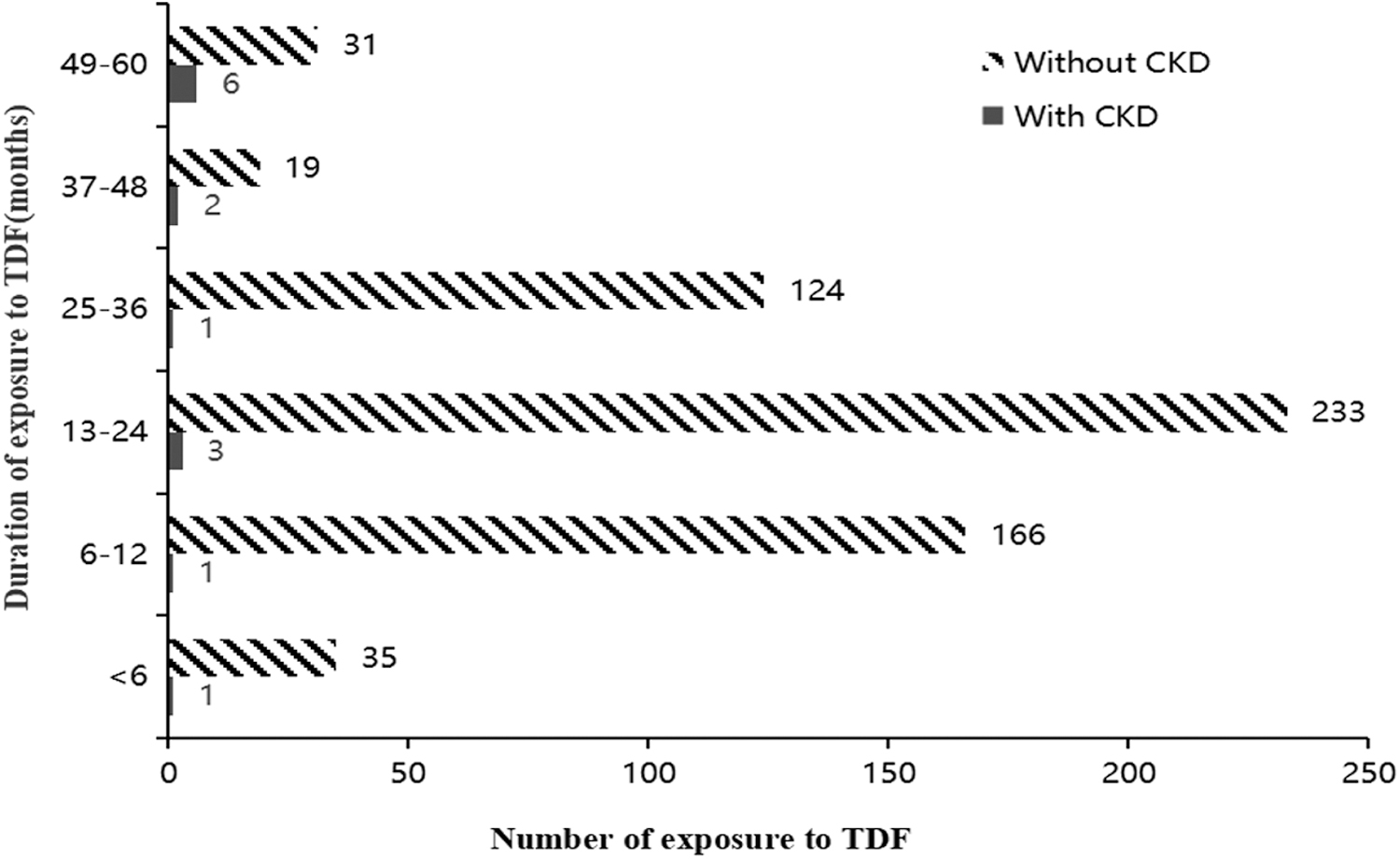
TDF exposure during the follow-up period. TDF, tenofovir disoproxil fumarate.
The median current CD4+ cell count was 294 cells/μL (IQR: 170–448), and 62% had CD4+ cell count >200 cells/μL. Most subjects (76%) were classified as WHO clinical stage 3 or 4. Seropositivity for HBV or HCV co-infection was 10% and 14%, respectively, and 5 (10%) participants had diabetes and 7 (14%) had arterial hypertension. The median hemoglobin level was 107 g/L (IQR: 75–128), and only 32% had hemoglobin >120 g/L. The median fasting blood glucose level was 5.1 mmol/L (IQR: 4.6–5.9), with 22% of participants >6.10 mmol/L. The median serum triglyceride level was 1.5 mmol/L (IQR: 1.1–2.3), with 52% of participants >1.7 mmol/L. The median serum cholesterol level was 3.5 mmol/L (IQR: 3.1–4.5), with 8% of participants >5.1 mmol/L (Table 1).
Risk factors associated with the development of CKD
The results showed that CKD was significantly (p < .05) associated with an older age, female sex, lower body weight, nadir CD4+ T cell count ≤200 cells/μL, baseline eGFR, WHO clinical stage 3 or 4, HCV co-infection, diabetes and arterial hypertension, hemoglobin ≤120 g/L, fasting blood glucose >6.1 mmol/L, serum triglyceride >1.7 mmol/L, history of SMZ-TMP utilization, a TDF or LPV/r contained regimen, and longer duration of ART (Table 1).
Adjusted multivariate logistic regression revealed that older age [adjusted odds ratio (aOR) = 1.04, 95% confidence interval (95% CI): 1.01–1.07], female sex (aOR = 3.17, 95% CI: 1.14–8.84), lower body weight (aOR = 0.95, 95% CI: 0.91–1.00), lower hemoglobin (aOR = 3.54, 95% CI: 1.51–8.30), longer duration of ART exposure (aOR = 1.02, 95% CI: 1.00–1.04), and baseline eGFR between 60 and 90 mL/min/1.73 m2 (aOR = 3.89, 95% CI: 1.21–12.46) were associated with the development of CKD (Table 2).
Risk Factors Associated with the Development of Chronic Kidney Disease in People Living with HIV
95% CI, 95% confidence interval; aOR, adjusted odds ratio.
Discussion
CKD is a comorbidity in PLWH, which is associated with excess morbidity and mortality. On the one hand, the prevalence of CKD appears to be decreasing, possibly due to improved outcomes with ART 16 –18 ; on the other hand, PLWH have a higher risk of developing CKD over time, and a 2- to 20-fold higher chance of developing ESRD, 19,20 compared to the general population. 21 –23 This means that with the transformation of HIV infection from an almost universally fatal illness into a manageable chronic condition in the ART era, with an aging population due to longer life expectancy, the underlying causes of CKD in PLWH have shifted from those driven by HIV itself to those driven by traditional risk factors such as diabetes, hypertension, and ART-related nephrotoxicity such as TDF usage.
CKD is observed in PLWH with variable frequency, depending on geographical location. According to a systematic review of studies from 60 different countries, the global prevalence of CKD was 6.4% in PLWH using the MDRD formula, 4.8% using the CKD-EPI formula, and 12.3% using the Cockcroft-Gault formula. 24 However, the African continent demonstrated the highest prevalence of CKD with 7%–48.5% of PLWH affected according to different studies. 25 Other epidemiological studies have reported a prevalence of CKD of 7%–20% in the Asian region, 26 with 16% in PLWH 8,12 and 10% in the non-HIV-infected population 27,28 in China.
Our results showed a CKD frequency of 5.8% in the PLWH population over a period of 5 years, which is similar to the results of European studies, 29,30 but much lower compared to Chinese studies. Since CKD in PLWH is multifactorial, the discrepancies of these results may be explained by the following factors: (1) time period differences, with different ART regimens used and more renal unfriendly drugs had been used in the earlier period; (2) frequency of comorbidities such as diabetes and hypertension in different populations; (3) frequency of co-infection, that is, HBV, HCV, and other opportunistic infections; (4) definitions of CKD use in different studies (using different formulae, including proteinuria, etc.); (5) ART initiation regardless of CD4+ T cell count in China after July 2016, when early ART was proven to prevent CKD. 16 –18
However, the increased susceptibility to CKD in PLWH is more complex, with contributions from traditional and HIV-specific risk factors for kidney disease, as shown in Table 1, while the adjusted multivariate logistic regression revealed only older age, female sex, lower body weight, hemoglobin ≤120 g/L, longer duration of ART, and baseline eGFR between 60 and 90 mL/min/1.73 m2 were significantly associated with the development of CKD.
After PLWH have started ART, VL testing is considered the gold standard for detecting treatment failure. As such, routine VL monitoring is recommended by WHO and most national HIV treatment guidelines. However, implementation of routine VL monitoring has proven challenging for the majority of participants from resource-limited settings, especially the VL test at the baseline, although the proportion of PLWH undergoing VL monitoring did increase after the national implementation of routine VL monitoring in 2020. This is why we could not estimate the correlation between VL (especially at baseline) and the development of CKD in our study.
According to our data, more than 95% of the PLWH in our center attained a sustainable suppression of the virus during the observation period. Nonetheless, as the kidney may serve as a viral reservoir, 31 and HIV viral replication may persist at low levels even with treatment, it has been argued that the circulating VL level may be a less sensitive indicator of CKD risk. 32 Thus, further studies concerning the correlation between VL and CKD in PLWH should be conducted.
The spectrum of renal pathology in PLWH is diverse, including lesions directly related to intrarenal HIV replication and lesions related to immune dysregulation and co-infections such as HCV. 33,34 Due to the variety of renal pathologies found in HIV infection, a renal biopsy remains the gold standard for accurately defining the pathology, which is often lacked in resource-limited settings, where no patient had kidney biopsy. Anemia is a common complication of CKD 35 ; its prevalence increases with CKD stage, ranging from 8% at stage 1 to 53% at stage 5. 36 Our data showed that lower hemoglobin levels were observed in CKD patients, and there were sex differences for hemoglobin values. As female sex has been shown as one of the predictors for anemia in CKD patients, 37 renal function should be monitored more often for PLWH with anemia, especially in females.
There is a strong relationship between HCV infection and renal insufficiency. As reported, ∼10%–16% of patients with HCV infection develop renal disease, and the prevalence of HCV infection in patients with renal dysfunction is higher compared with the general population (9.5% vs. 1.6%), which is in accordance with our results. 38 In the interferon era, the treatment of HCV infection in CKD patients was hampered due to a significant number of treatment-related adverse events (predominately anemia and infectious complications). Fortunately, the development of direct-acting antivirals has revolutionized the field, allowing viral eradication in these patients. 39 HCV has also been shown by our group to increase Cr 40 ; therefore, rapid treatment for HCV co-infection should be performed. 41
Several studies have reported the beneficial effects of ART on CKD. 4,5 However, the prolonged duration of ART exposure makes long-term toxicity an important issue, and some antiretroviral drugs require dosage adjustment or are contraindicated in advanced CKD stages. The ART drugs usually associated with CKD include tenofovir, abacavir, atazanavir, indinavir, and LPV/r. 21,42 Mechanisms of nephrotoxicity of those drugs are well summarized elsewhere. 43 In general, renal dysfunction is reversible after the withdrawal of the causal drug, although persistent renal damage has been reported. 44
We found that the use of TDF and LPV/r was significantly associated with the development of CKD in univariate analyses, but not in multivariate analyses after being adjusted with the duration of ART, as well as the history of SMZ-TMP utilization. This may be related to the small number of our CKD patients and a relative short duration of follow-up. However, the higher awareness of TDF nephrotoxicity contributed to TDF discontinuation in CKD patients. Recently, other drugs with lower or no renal toxicity such as tenofovir alafenamide and INIs, respectively, have been more readily available in China, and could also become a choice in resource-limited settings. However, even though these new drugs are less nephrotoxic, concerns have been raised about their potential metabolic side effects and weight gain. 45
As our study is observational in nature, kidney function monitoring is conducted according to local standards, and its performance is based on clinician decisions, but those tests have to be paid for by PLWH, which limits testing frequency. Monitoring for kidney function by means of Cr had not occurred on a biannual basis for some of the PLWH in our cohort. According to current recommendations, urinalysis is suggested when PLWH enter into care and during their annual monitoring. Compared to the Cr test, the urine test is less expensive, especially when one uses a low-cost dipstick to quantify the urine.
However, as the follow-up of PLWH is generally conducted by infectious disease physicians, and many of whom do not realize the feasibility and importance of the urine test in detecting early renal impairment, efforts to encourage physicians to screen for proteinuria in PLWH are warranted. Training for Chinese HIV care providers on renal function screening should be strengthened. We also recommend that nephrologists should be integrated earlier in HIV care. More access to tests for kidney function is warranted to early identify patients with stage CKD and rapidly avoid the use of nephrotoxic drugs, as our result has shown that a pre-existing mild renal dysfunction at baseline is associated with the development of CKD.
Standard therapies for CKD applied among the general population are recommended to prevent CKD progression in PLWH, including the appropriate management of diabetes and blood pressure control. Unexpectedly, neither the history nor presence of diabetes or hypertension reached statistical significance in our multivariate analysis. The possible reasons included the following: (1) the participants in our cohort had good compliance and relative control of their glycemia and blood pressure and (2) our participants had a relatively young age and our study had a relatively short observation period, which could not fully demonstrate the impact of long-term hyperglycemia and blood pressure exposure on renal function. Therefore, these parameters should be taken into consideration in the daily management of PLWH.
Avoiding nephrotoxic agents is also recommended to preserve kidney function, especially the Chinese herbal medications commonly used among Chinese patients; these kinds of data were not available in our cohort, and we will pay more attention to prevent renal toxicity. In case of CKD progression to ESRD, for PLWH on ART, survival on dialysis is comparable to that of HIV-negative patients. 46,47 Some observational studies have also demonstrated that the choice of hemodialysis or peritoneal dialysis does not appear to impact the survival. 48 In our center, 10 patients with ESRD received peritoneal dialysis as hemodialysis was not available, and 2 of them died due to severe peritoneal infections. Although the International AIDS Society recommends that selected PLWH with ESRD should be the recipients of kidney transplants if the eligibility criteria are met, 49 this is not commonly practiced in China.
Our study had certain limitations. First, as a single-center study, our results are less representative, so larger multicentric studies should be further conducted in resource-limited regions. Second, as our monitoring means were limited to serum Cr without the evaluation of urine protein, and the choice of using MDRD formula to calculate eGFR in Chinese PLWH, which may both be among the reasons for our relatively low prevalence of CKD patients compare with other Asian studies. Further studies should be conducted based on more accurate monitoring methods of renal function, including both serum creatine and proteinuria, and more adapted formulae 50 may be required for use in Chinese PLWH. Third, since data on height were lacking in our cohort, BMI could not be calculated. In our future research, height data will be added to reduce sex bias.
In summary, CKD is not infrequent in PLWH with a combination of traditional and HIV-specific risk factors. An improved understanding of these complex interactions will allow the development of novel tools for kidney health monitoring and the early diagnosis of kidney dysfunction. Our findings highlight the suboptimal monitoring of CKD in PLWH in our resource-limited center. There is a need for affordable and scalable monitoring options to improve care for this population. As therapy for HIV continues to evolve, multidisciplinary specialists, including infectious disease physicians and nephrologists, must keep abreast of current developments to provide the optimal care to PLWH.
Footnotes
Authors' Contributions
Q.C. and J.-P.R.: conceptualization; writing—original draft; formal analysis; and writing—review and editing (equal). L.F. and T.-L.C.: software; methodology; and writing—review and editing (equal). J.Z., Q.W., and J.L.: writing—original draft, review, and editing (supporting). X.-E.G.: conceptualization and writing—review and editing (supporting).
Acknowledgments
J.-P.R. is the holder of the Louis Lowenstein Chair in Hematology and Oncology, McGill University, and received support from Fonds de la Recherche Québec-Santé (FRQ-S): Réseau SIDA/Maladies infectieuses and Thérapie cellulaire.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Discipline Cultivation Project of Zhongnan Hospital of Wuhan University (ZNXKPY2021022). The funding body did not play any role in the study design and collection, analysis, and interpretation of data and in writing of this article.