
Abstract
Effective management of HIV and hepatitis C virus (HCV) coinfection warrants special emphasis on interactions between direct acting antivirals (DAAs) and antiretroviral therapy (ART) along with maintenance of treatment compliance. All HIV-HCV coinfected adult patients (2015–2020) were included in this real-life retrospective study. Prevalence of coinfection, proportion of coinfected patients treated, compliance rate, sustained virological response at week 12 (SVR12) after the end of therapy, and adverse events were assessed. Among 4578 HIV patients, 232 (5.1%) had HCV coinfection. Ninety-two (39.7%) were intravenous drug users. One hundred twenty-eight (55.1%) patients presented to the liver clinic. Seventy-six (32.8%) patients [mean age: 36.6 ± 10.4 years; 65 (85.5%) males; mean CD4 count: 396 ± 246 cells/mL] completed DAA therapy, whereas 52 (22.4%) patients defaulted and 75 (32.3%) were lost to follow-up. Sixty-seven (82.2%) patients had chronic hepatitis and 9 (11.8%) had compensated cirrhosis. Median (range) HCV-RNA was 5.9 × 106 IU/mL (2.4 × 105–9.9 × 105). Among 15 (19.5%) treatment experienced patients, 14 were pegylated interferon experienced and one was NS5A-inhibitor experienced. ART regimens comprised a combination of tenofovir (T), lamivudine (L), efavirenz (E), nevirapine (N), and/or zidovudine (Z) at dosage and modifications as applicable [TLE: 63 (82.9%), ZLN:11 (14.5%), and ZLE: 2 (2.6%)]. Overall, 74 (97.4%) out of 76 patients who completed DAA therapy achieved SVR12. Adverse events were minor and well-tolerated. HIV-HCV-coinfected patients demonstrate excellent SVR12 and tolerability with available DAAs, with no major adverse events.
Introduction
AIDS is a chronic, potentially life-threatening multisystem disease caused by infection with HIV, which leads to progressive CD4+ T cell damage and predisposes to increased risk of infections and malignancies. 1 Timely initiation of lifelong highly active antiretroviral therapy (HAART) remains the only durable way to halt or delay progression at present. 2
High-risk populations such as men who have sex with men (MSM), people who inject drugs (PWID), sex workers, and incarcerated people are at greater risk of both HIV and hepatitis C virus (HCV) coinfection in view of shared modes of transmission. 1,3,4 The overall prevalence of HIV-HCV coinfection is reported to be around 5%–37%, with strikingly higher prevalence (>80%) in PWID. 4
Chronic hepatitis C (CHC) is the leading cause of liver-related morbidity and mortality rate (non-HIV associated) in HIV-HCV-coinfected patients. Cirrhosis and hepatocellular carcinoma may develop a decade earlier in coinfected patients than in HCV monoinfected patients. 3,5 Also, the rate of drug (HAART)-induced liver injury has also been reported to be higher in coinfected patients and needs careful monitoring, especially in patients with advanced fibrosis. 5 –7
Although new direct acting antivirals (DAAs) against CHC have greatly simplified management in this unique patient population with >90% sustained virological response at week 12 (SVR12) rates in clinical trials, real-life data from low- to middle-income countries remain scarce. 3 Patients with decompensated cirrhosis, genotype-3, prior DAA failure, and resistance-associated substitutions (RAS) may still make a small proportion of such patients “hard-to-treat.” Poor liver transplantation prospects in this high-risk population further emphasizes the need of detection and treatment of CHC at an early stage. 3,8 At present, special importance should be directed toward prevention and effective screening of HIV-HCV coinfection. The key to success is ensuring widespread availability, easy access, and compliance to both HAART and DAAs, with carefully curated treatment regimens considering drug–drug interactions and possible adverse events. 3,9
In this single-center retrospective analysis, done at a tertiary care research and teaching institute, we present our real-life experience in patients with HIV-HCV coinfection with respect to the prevalence of HIV-HCV coinfection, treatment compliance, drug regimens used, SVR12 achieved, and treatment-related adverse events.
Materials and Methods
Study participants
A retrospective review of records of all consecutive patients referred from the ART clinic of our tertiary care teaching institute to the liver clinic in view of positive anti-HCV antibodies between 2015 and 2020 was done. All adult patients (>18 years) with indication of CHC treatment 3 were considered for inclusion. Patients with hepatitis B virus coinfection, suspected acute HCV infection, ineligibility for ART, undetectable HCV-RNA levels, decompensated cirrhosis, contraindications for initiation of DAAs such as pregnancy, concomitant antituberculosis therapy, and severe comorbidities with less than a 6-month predicted survival were excluded. Prevalence of HIV-HCV coinfection was calculated by dividing the total number of patients with CHC infection by the total number of patients registered in the ART clinic between 2015 and 2020.
The study was approved by the Institute's Ethics Committee and adhered to the Declaration of Helsinki. Informed consent was not taken due to the retrospective nature of the study and the identities of patients have been kept confidential.
Study definitions
Sustained virological response at week 12
SVR12 was defined as nondetectable quantitative HCV RNA by real-time polymerase chain reaction at 12 weeks after end of DAA therapy. 3
DAA defaulter
Patients who were initiated on DAAs but did not complete treatment or stopped DAAs for more than a week were considered noncompliant/defaulters and excluded from final analysis.
Diagnosis of cirrhosis
The diagnosis of cirrhosis 3 was based on “previous liver biopsy if available, or a combination of clinical (history of ascites, variceal bleed, hepatic encephalopathy, or presence of stigmata of chronic liver disease), imaging (heterogeneous echo texture of liver with irregular outline, volume redistribution, altered liver size, portosystemic collaterals), laboratory (low serum albumin, aspartate aminotransferase/alanine aminotransferase ratio >1), and endoscopic findings (presence of esophageal varices) and/or liver stiffness measurement (LSM) of ≥12.5 kPa”. LSM of ≥12.5 kPa was used to diagnose and differentiate compensated cirrhosis from chronic hepatitis.
Baseline and follow-up assessment
Available demographic variables, clinical history, physical examination, and laboratory and radiological investigations were collected from hospital records. Extensive record search in all eligible patients focused on baseline hemogram, liver function tests, renal function tests, concomitant comorbidities, ART regimen, CD4 cell count, any past treatment for HCV, and abdominal ultrasonography, and transient elastography (TE) was undertaken. Hepatitis C viral load (COBAS “TaqMan” assay 10 with a lower limit of detection of 15 IU/mL) was done at baseline and at the week 12 post-treatment for SVR12. HCV genotype, if available, was recorded. The assessment of liver fibrosis was done using TE (FibroScan, Echosens, Paris). The patients were classified as having no or minimal fibrosis [F0–F1] < 7.1 kPa, moderate fibrosis [F2] = 7.1–9.4 kPa, severe fibrosis [F3] = 9.5–12.4 kPa, or cirrhosis [F4] ≥ 12.5 kPa depending on the liver stiffness. 11
DAA regimens and duration along with a concomitant ART regimen were noted. Noncompliance or default on DAA therapy was also assessed from patient records. Adverse effects and treatment modifications, if any, were recorded.
Management
ART regimens were given free of cost as per the National AIDS Control Organization (NACO) guidelines 2 by the ART clinic. DAA regimens were modified 3 as per reported interactions with concomitant ART. In patients on efavirenz, the dose of daclatasvir was increased to 90 mg/day. All patients either received efavirenz or nevirapine in ART regimen, and hence, velpatasvir was not used in any patient. Ribavirin dose was reduced when zidovudine was part of the ART regimen with close monitoring of hemoglobin.
Statistical analysis
Statistical analysis was done using Statistical Package for Social Sciences (version 22.0 for windows; SPSS, Inc., Chicago, IL) and MedCalc® Statistical Software version 19.6 (MedCalc Software Ltd, Ostend, Belgium). The results of quantitative variables are presented as mean with standard deviation and/or median with 95% confidence interval (CI), depending on the distribution of attributes and as proportions with percentages for qualitative variables. Comparison between groups was made using chi-square and Fisher exact tests for categorical variables, and Student's t-test and Mann–Whitney U test for parametric and nonparametric variables, respectively. p Value of ≤.05 (two-tailed) was considered statistically significant.
Results
Prevalence of HIV-HCV coinfection and compliance to DAAs
Overall, 4578 patients with HIV were registered in the ART clinic of our institute between 2015 and 2020. Out of 4578 patients, 232 (5.1%) had HCV coinfection and were referred to the liver clinic. Ninety-two (39.7%) patients were PWID, whereas 12 (5.2%) were MSM.
One hundred twenty-eight (55.2%) patients physically presented to the liver clinic and were initiated on DAAs for HCV infection, whereas 75 (32.3%) patients were lost to follow-up and 29 (12.5%) died without initiation of DAAs. The exact cause of death could not be ascertained from the available records. Among the 128 (55.2%) patients who were initiated on DAAs, only 76 (59.4%) completed treatment, whereas the remaining 52 (40.6%) defaulted. Among the whole cohort of 232 coinfected patients, only 76 (32.7%) completed treatment, whereas the remaining eligible and alive patients (n = 127, 52.3%) were either noncompliant or lost to follow-up (Fig. 1).
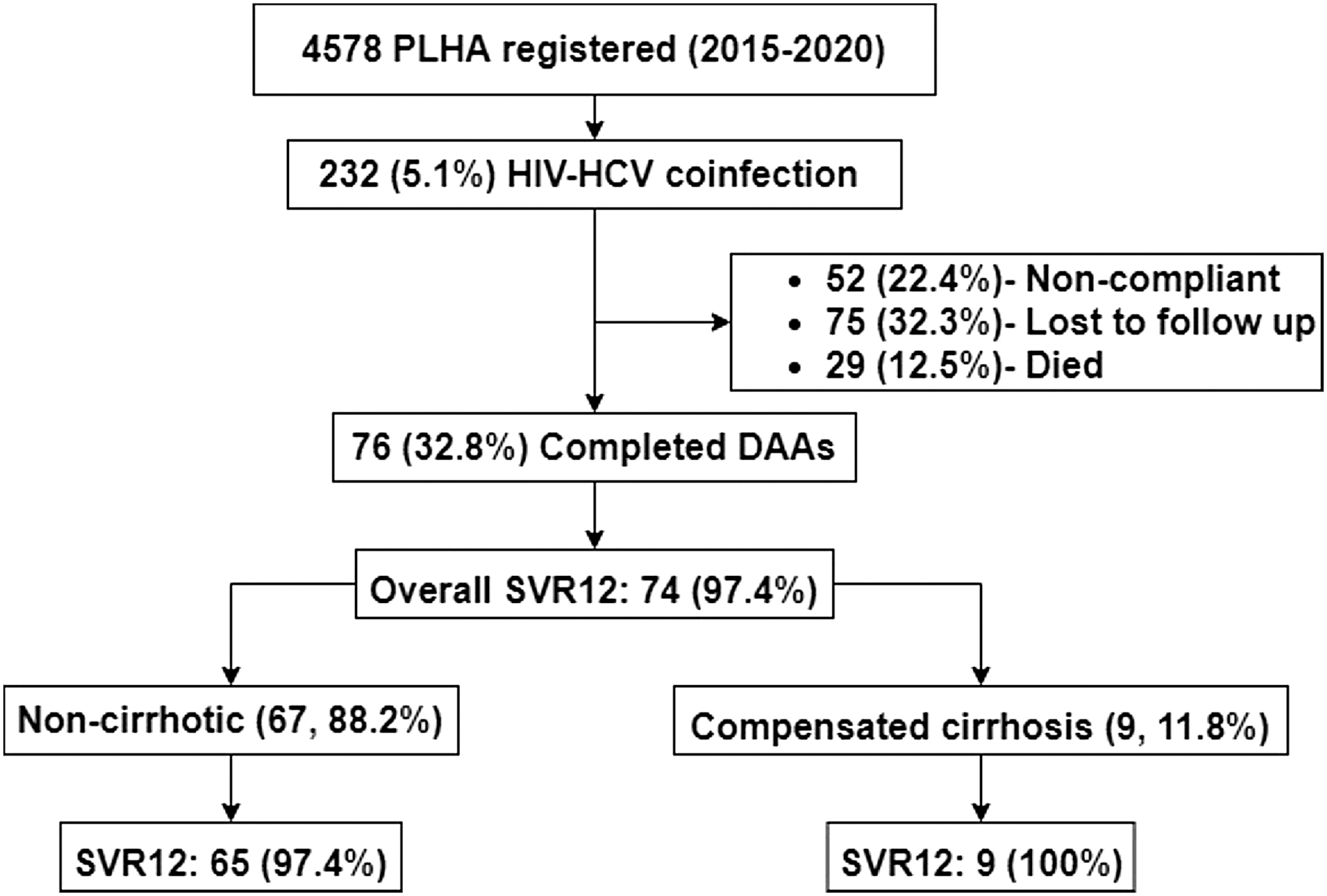
Flow of patients in the study.
Baseline characteristics
Baseline demographic characteristics and laboratory parameters of the study population (n = 76) are given in Table 1. Mean age of the study population was 36.6 ± 10.4 years with 65 (85.5%) males. Sixty-seven (88.2%) patients had chronic hepatitis, whereas 9 (11.8%) had compensated cirrhosis. Genotype 3 was the most common (n = 34, 44.7%) followed by genotype 1 (n = 25, 32.9%). Genotype was not available in 13 (17.1%) patients. Diabetes and obesity were present in 9 (11.8%) and 8 (10.5%) patients, respectively.
Baseline Characteristics of HIV-Hepatitis C Virus-Coinfected Patients
HCV, hepatitis C virus.
ART and DAA regimens
ART regimens were given as per the NACO guidelines. 2 A fixed-dose combination (FDC) of tenofovir (300 mg), lamivudine (300 mg), and efavirenz (600 mg) once a day was the most commonly used ART regimen in 63 (82.9%) patients followed by an FDC of zidovudine (300 mg), lamivudine (300 mg), and nevirapine (200 mg) in 11 (14.5%) patients. Among the DAA regimens, sofosbuvir/daclatasvir combination was most frequently used (n = 41, 53.9%), whereas sofosbuvir/ledipasvir combination was used in 25 (32.9%) patients. Fifteen (19.5%) patients were prior treatment experienced (14-pegylated interferon, 1-NS5A inhibitor) (Table 2).
Antiretroviral Therapy and Direct Acting Antiviral Regimens
T, tenofovir; L, lamivudine; E, efavirenz; N, nevirapine; Z, zidovudine.
SVR12 post-DAA therapy
Overall, SVR12 was seen in 74 (97.4%) patients. There was no significant difference in SVR12 based on degree of fibrosis, presence of cirrhosis, prior treatment experience, HCV genotype, DAA regimen used, and comorbidities (diabetes mellitus, obesity) (Table 3).
Sustained Virological Response at Week 12 Among Various Subgroups
DAA, direct-acting antiviral; SVR12, sustained virological response at week 12.
Adverse events
Adverse events were minor and included fatigue (n = 9, 11.8%), nausea (n = 7, 9.2%), anemia (n = 6, 7.8%), insomnia (n = 6, 7.8%), and headache (n = 5, 6.5%). None of the side effects led to treatment modification or discontinuation during follow-up.
Discussion
This real-life retrospective analysis demonstrates excellent efficacy, tolerability, and safety of DAAs in HIV-HCV coinfected patients with appropriate dose modifications of DAAs depending on the concomitant ART regimen used. The SVR12 was achieved in 97.4% of patients in our study. The efficacy was exceptional in both treatment-naive and pegylated interferon-experienced patients and in patients with and without cirrhosis with only minor side effects in few patients and no treatment-related interruptions. More than 50% patients being either noncompliant to these highly effective, convenient treatment regimens or getting lost to follow-up was a concerning finding of our real-life experience. Treatment default might lead to the development of difficult-to-treat HCV variants 3 and the rapid progression of liver disease to cirrhosis and its complications requiring liver transplantation in the future adding to the enormous financial and social burden. 7,12
One of the major reasons for the same could be the cost of DAA therapy for CHC. While ART is provided free of cost through our national program by the government, there was an out-of-pocket expense for the treatment of HCV coinfection for most patients before the launch of the National Viral Hepatitis Control Eradication Program. Treatment default among patients registered for care at the liver clinic is worrying. This reiterates the need for more stringent follow-up and detailed counseling at the ART center and liver clinic, as well as before treatment initiation in this vulnerable group with involvement of a multidisciplinary team including ART care physicians, hepatologists, deaddiction psychiatrist, and social workers, wherever possible. 7,12
The prevalence of HIV-HCV coinfection in our study cohort was 5.1% similar to a recent worldwide meta-analysis. 4 The overall prevalence of 5%–30% and up to 80% in PWIDs has been reported in various previous studies. 3,4,13,14 In a meta-analysis 15 including 39 studies from 10 countries in the Asia Pacific region comprising more than 89,000 HIV-positive patients, the prevalence of HIV-HCV coinfection was highly variable between countries and at-risk populations. The pooled prevalence (95% CI) of coinfection was 8% (6.4%–9.8%) in Hong Kong and 25.5% (17.5%–34.4%) in China. In India, HIV-HCV coinfection was present in 4.1% (1.7%–7.3%), whereas 42.6% (38.7%–46.5%) were coinfected in Nepal. Up to 5%–6% prevalence was reported from Cambodia, Myanmar, and Thailand.
A relatively lower prevalence in our study compared with other Asian countries can be attributed to a younger age group (36.6 ± 10.4 years), which may signify a shorter duration of IV drug abuse leading to reduced chances of exposure to both HIV and HCV. Also, the data were real life and not from a specific high-risk cohort of PWIDs, deaddiction center, or incarcerated patients. Previously, a higher prevalence of HIV-HCV coinfection has been reported in a subpopulation of PWIDs, former blood donors, and blood transfusion recipients. 15 The younger age group of our study population reiterates the need of early diagnosis and effective treatment to halt further transmission and avoid progression to cirrhosis and its complications. 5,7
Despite the availability of convenient, all oral DAAs, a sizeable proportion of coinfected patients did not seek, take, or complete HCV treatment. More than 50% did not even show up in the liver clinic after referral, whereas among those who were advised DAAs (n = 128), nearly one-third (n = 52) defaulted. Ongoing IV drug use, younger age, associated social stigmas, or being uncomfortable with revisiting “HIV/AIDS clinics” especially in young adults, and inability to understand the long-term consequences may have been the reason for such noncompliance. Ongoing substance abuse especially stimulants such as cocaine/methamphetamines, chaotic lifestyle, poor social support, associated psychiatric disorders, illiteracy, and poverty have been found to be associated with noncompliance in patients on HAART in previous studies. 5,7,9,16 –19
Noncompliance has been attributed more to a “state (ongoing drug use, no social support)” rather than a trait and may be rectified by improving social awareness, providing personal counselors, psychiatrist support, involvement of patient's family/close relatives, and easy and nonstigmatizing access to HAART and DAA to patients.
Grazoprevir/elbasvir, glecaprevir/pibrentasvir, and voxilaprevir are not available in our country, and hence were not used in any patient. Also, government-provided FDC ART regimens 2 in our country, during the period of study, included either nevirapine or efavirenz along with tenofovir/zidovudine and lamivudine, which also prohibited use of sofosbuvir/velpatasvir combination. Sofosbuvir in combination with daclatasvir or ledipasvir was the two most commonly used combinations (Table 2). Weight-based ribavirin was used in combination with sofosbuvir alone when NS5A inhibitors were not available in our country, whereas in later years it was used only in genotype-3 patients with cirrhosis as an add-on to sofosbuvir and NS5A inhibitor regimens as per guidelines. 3
Overall, SVR12 in our study was more than 97%, which is similar to previously reported results from clinical trials 3,14,20 –27 and other real-life studies. 3,20,28 –30 SVR12 was not affected by the presence of cirrhosis, genotype, prior pegylated interferon experience, presence of obesity or diabetes, and DAA/ART regimen used (Table 3). Side effects were minimal and none required dose modification or discontinuation. Nonspecific symptoms such as fatigue and headache were more frequent. Similar good tolerability has been reported before if one uses carefully curated regimens with special emphasis on drug–drug interactions. 3,13,14,20,22 –26,28 –30
Close, frequent personalized follow up in this young, vulnerable population is extremely important to prevent progression of liver disease and avoiding emergence and transmission of RAS-containing HCV variants, which may pose great difficulty in achieving the goal of HCV eradication in near future, leading to tremendous burden on the health care system and also have negative social ramifications. The retrospective nature of the study with a relatively small sample size of “treated” patients, missing data on treatment defaulters, nonavailability of HIV viral load, and no patients on new protease-boosted ART regimens are few limitations of this study.
To summarize, all patients with HIV infection should be screened for HCV coinfection, more so in PWID and MSM. Personalized counseling and an individualized DAA regimen in combination with an appropriate ART regimen can be highly effective in compliant patients. Social outreach programs with involvement of local people and primary health care facilities can greatly help in maintaining adherence and ensure treatment completion. Furthermore, extension of community health care outcome programs utilizing telecommunication tools for remote outreach may help in ensuring abstinence and close monitoring. 31 –33
Conclusion
HIV-HCV-coinfected patients demonstrate excellent SVR12 rates and tolerability with available DAAs; however, a dismal proportion of these patients seek and complete their treatment, outlining the need of better counseling and close follow-up in this high-risk cohort.
Footnotes
Authors' Contributions
S.M.: Conceptualization (supporting); methodology (supporting); formal analysis (lead); writing—original draft preparation (lead), and writing—review and editing (equal). S.T.: Conceptualization (lead); methodology (lead); formal analysis (supporting); and writing—review and editing (equal). A.D.: Writing—review and editing (equal). N.V.: Writing—review and editing (equal). M.P.: Writing—review and editing (equal). G.S.R.S.N.K.N.: Writing—review and editing (equal). A.S.: Methodology (supporting) and writing—review and editing (equal). A.D.: Methodology (supporting) and writing—review and editing (equal). R.K.D.: Writing—review and editing (equal). V.S.: Writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was recieved for this article.