
Abstract
Functional magnetic resonance imaging (fMRI) studies have demonstrated that HIV-infection affects the fronto-striatal network. It has not been examined what impact efavirenz (EFV), an antiretroviral drug notorious for its neurocognitive effects, has on the reward system: a key subcomponent involved in depressive and apathy symptoms. Therefore, this study aims to investigate the effect of EFV on reward processing using a monetary incentive delay (MID) task. In this multicenter randomized controlled trial, asymptomatic adult participants stable on emtricitabine/tenofovirdisoproxil fumarate (FTC/TDF)/EFV were randomly assigned in a 2:1 ratio to switch to FTC/TDF/rilpivirine (RPV) (n = 30) or continue taking FTC/TDF/EFV (n = 13). At baseline and 12 weeks after therapy switch, both groups performed an MID task. Behavior and functional brain activity related to reward anticipation and reward outcome were assessed with blood-oxygen-level-dependent fMRI. Both groups were matched for age, education level, and time since HIV diagnosis and on EFV. At the behavioral level, both groups had faster response times and better response accuracy during rewarding versus nonrewarding trials, with no improvement resulting from switching FTC/TDF/EFV to FTC/TDF/RPV. No significant change in activation related to reward anticipation in the ventral striatum was found after switching therapy. Both groups had significantly higher activation levels over time, consistent with a potential learning effect. Similar activity related to reward outcome in the orbitofrontal cortex was found. Discontinuing FTC/TDF/EFV was not found to improve activity related to reward anticipation in asymptomatic people living with HIV, with similar cortical functioning during reward outcome processing. It is therefore likely that EFV does not affect motivational control. Further research is needed to determine whether EFV affects motivational control in HIV populations with different characteristics.
Introduction
The introduction of combination antiretroviral therapy (cART) has dramatically increased the life expectancy of people living with HIV (PLWH). 1 As a result of the improved life expectancy, the focus of HIV-related care has shifted to treatment and prevention of comorbidities due to HIV and cART itself. A common but relatively little studied comorbidity, with a major impact on quality of life in PLWH, is the presence of HIV-associated neurocognitive disorders (HAND). 2,3 HAND is characterized by neurocognitive functional impairments in memory, concentration, attention, and motor skills, which are traditionally assessed with a neuropsychological assessment (NPA). 3 Blood-oxygen-level-dependent (BOLD) functional magnetic resonance imaging (fMRI), although not a validated clinical tool such as NPA, is also widely used in the research setting to assess functional impairment. 4
Since BOLD fMRI can detect early changes in the brain in the absence of symptomatic neurocognitive functional impairment, it is considered to be more sensitive in assessing the impact of cART on the brain than NPA alone. 5
Efavirenz (EFV), a non-nucleoside reverse transcriptase inhibitor (NNRTI), is an important and frequently used antiretroviral anchor drug worldwide. It is part of a single tablet regimen composed of emtricitabine/tenofovirdisoproxil fumarate (FTC/TDF)/EFV and was the preferred first-line therapy for more than 15 years until 2018 according to the World Health Organization. 6 Although use has slowly declined since then, EFV is still recommended as an alternative first-line regimen anchor and remains widely used in low- and middle-income countries, with forecast analyses predicting 10 million PLWH (i.e., 25% of the estimated total population) will still be using EFV-based regimens by 2025. 7,8 Moreover, even in high-income countries, EFV continues to be used, as 7% of PLWH in the Netherlands used FTC/TDF/EFV in 2020. 9
EFV is notorious for its neurocognitive side effects such as dizziness or insomnia 10 and is also associated with neurocognitive functional impairment, 11 –14 although this is still debated as it is not confirmed in all studies. 15 –17 In previous work, we showed that discontinuing EFV in asymptomatic PLWH resulted in an improvement in the cognitive domains' attention and speed of information processing, as assessed by NPA. 18 The question is what dysfunction in the neurocognitive network is underlying this.
To date, little is known about exactly which neurocognitive systems are affected by EFV. One possibility is the fronto-striatal reward system: a key subcomponent involved in depressive and apathy symptoms and responsible for reward processing. 19 Reward processing consists of several neurocognitive processes such as processing the outcome of a reward and anticipating future rewards, and is crucial for decision-making and goal-directed behavior. 20 These “reward anticipation” and “reward outcome” processes are modulated by the subcortical ventral striatum and the orbitofrontal cortex (OFC) and are indicators of, respectively, subcortical and cortical functioning. 21 –23 Previous fMRI research has suggested that HIV-infection impairs subcortical functioning, including reward anticipation, but spares cortical functioning. 24,25 In addition, there is evidence that EFV negatively impacts executive functioning and, although in an adolescent population, even cortical functioning. 26,27 It is therefore essential to investigate whether and what part of reward processing is affected by EFV.
The aim of this study is to determine the effect of EFV on reward processing using BOLD fMRI. We conducted a randomized controlled trial (RCT) and randomly assigned asymptomatic PLWH stable on FTC/TDF/EFV to switch to FTC/TDF/rilpivirine (RPV) or continue FTC/TDF/EFV. Since our entire study population used EFV at the onset of the trial, we specifically studied the effect of EFV by discontinuation in one group. We hypothesized that, due to HIV-infection impairing subcortical functioning and potentially rendering it susceptible to neurotoxic damage of EFV, switching from FTC/TDF/EFV to FTC/TDF/RPV would result in relatively improved ventral striatal responses, while cortical functioning would remain stable.
Materials and Methods
Participants
The current study is a subanalysis of the ESCAPE (Effect of SwitChing AtriPla to Eviplera on neurocognitive and emotional functioning) trial, which was conducted from 2015 to 2017 at two large HIV treatment centers in the Netherlands (OLVG, Amsterdam) and the University Medical Centre Utrecht (UMC Utrecht). 18 We chose to create a homogenous study population by way of strict inclusion and exclusion criteria as fMRI can easily be influenced by confounding factors and PLWH already exhibit greater variability with respect to fMRI measurements. 28,29 In short, we included asymptomatic male PLWH aged 25–50 years, stable on FTC/TDF/EFV for at least 6 months.
Potential participants were excluded if they had an active or past central nervous system infection, an active psychiatric or neurologic disorder, a history or evidence of alcohol or drug abuse as assessed by the Drug Abuse Screening Test (DAST-10). 30 During the study, participants with a viral load (VL) of >200 copies/mL were excluded from analysis, as we believed this could confound fMRI results. For the full list of inclusion and exclusion criteria, see the published study. 18
The trial was performed in accordance with the Declaration of Helsinki, was approved by the Medical Research Ethics Committee of the UMC Utrecht and was registered at Clinicaltrials.gov under number NCT02308332. Findings were reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guideline. 31 The trial was funded by Gilead Sciences. The funder had no role in the trial design, data collection or analysis, or drafting of the article. All participants provided written informed consent.
Trial design and procedures
Participants taking FTC/TDF/EFV were randomized (2:1), using computer-generated block randomization with a variable block size (range 3–9), to switch to FTC/TDF/RPV or continue FTC/TDF/EFV. A study nurse, not involved in the trial, generated the random allocation sequence and assigned participants. FTC/TDF/RPV was chosen because it is a single-tablet regimen composed of the same backbone and a similar NNRTI anchor drug as FTC/TDF/EFV. They were instructed to take one tablet daily and, in case of FTC/TDF/RPV, with a substantial amount of food. The NPA was conducted by researchers who were unaware of the participant's allocated treatment. Researchers performing the fMRI scan and participants were not blinded, since we believed that their knowledge of the allocated treatment would not affect our objective outcome of fMRI brain activity.
At baseline and after 12 weeks, participants underwent fMRI scanning. All MRI scans were examined by a radiologist for intracranial pathology. Cognition was assessed using an NPA and it was determined whether the distribution of potentially confounding asymptomatic neurocognitive impairment, as defined according to the Frascati criteria, was similar between groups. 3 Routine safety blood samples were obtained to assess laboratory abnormalities, disease progression, and virologic suppression.
Participants switching to FTC/TDF/RPV had two additional outpatient visits after 2 and 4 weeks to monitor for side effects and obtain blood samples, which was a standard clinical procedure at the time. A follow-up time of 12 weeks was chosen as previous research showed that neurocognitive changes after initiation or therapy switch were observed within this time frame. 32 –34
Monetary incentive delay task
The reward task used in our study is based on the original monetary incentive delay (MID) task by Knutson et al (Fig. 1). 23,35 –38 HIV-associated neuropathological changes mainly occur in subcortical regions, such as the striatum, and in the white matter tracts connecting to the cortex. 39,40 As these regions are presumed more susceptible to possible neurotoxic effects of EFV, we selected the MID task as it reliably activates the ventral striatum during reward anticipation and the OFC during reward outcome. 24,36,37

Schematic representation of the reward task, based on the monetary incentive delay task.
35,49
There were two types of trials: potentially rewarding
The task consists of 60 separate trials, of which 30 are potentially rewarding and 30 nonrewarding. The rewarding trials are indicated with a smiling face as reward cue and the nonrewarding trials with a nonsmiling face, at the onset of each trial. A fixation star, which acts as an anticipation cue, appears after the reward cue. Following the fixation star, a target (exclamation mark) is presented requiring participants to react as fast as possible by pressing a button with their dominant index finger, irrespective of trial type. Participants were instructed they were able to win €1.00 if they responded within the time limit (i.e., duration of the target being presented on the screen) in rewarding trials.
Feedback after each trial notified participants of their performance indicating if they had earned money, as well as their cumulative total at that moment. We told participants that they would receive the cumulative total of the reward won from the actual experiment. During a practice session before the actual task, the participant's quickest response time was recorded to act as a baseline to adjust the task to individual performance levels. In 50% of trials, the target was presented for the duration of the individual's quickest response time plus 200 ms, enabling participants to be successful in these trials.
In the other trials, the time limit was decreased with 150 ms, so that participants could not respond in time. This resulted in sufficient power for analysis of successful versus unsuccessful trials and ensured that all participants received an equal reward amount (target €15.00). The task was designed so that maximum statistical power for the fMRI analyses could be achieved in a relatively short time: only one level of reward was used, and no loss trials were included.
To reduce the collinearity between reward anticipation and reward outcome, the anticipation cue time and the intertrial interval time were varied (mean duration 3,535 ms, range 779–6,729 ms; mean duration 3,535 ms, range 1,029–6,979 ms, respectively). The BOLD signal in response to reward anticipation could in this way be modeled independently of that of the reward outcome. Individual trials had an average duration of 9,571 ms (range 4,946–16,107 ms), resulting in a total task duration of 9 min 35 s.
Behavioral analysis
Repeated-measures analysis of variance (ANOVA) was performed to test for effects of trial (rewarding and nonrewarding trials), group (FTC/TDF/RPV vs. FTC/TDF/EFV), and time (baseline vs. week 12) on the response time, response accuracy, and reward amount. The Cook's distance was used to check for possible influential outliers (>1.0), and homogeneity of variances was tested using Levene's test. 41 A two-sided alpha level of 0.05 was used and statistical analyses were conducted using SPSS version 25.0 (IBM Corp. Armonk, NY).
Functional MRI
For an explanation of the procedures for fMRI image acquisition, preprocessing, and initial individual analyses, see Supplementary Digital Content S1.
Region-of-interest analyses
We performed primary analyses in one region-of-interest (ROI) per contrast: the combined bilateral ventral striatum for reward anticipation and the combined OFC for reward outcome, based on the previous findings. 23,35 These regions were defined using the Automated Anatomical Labeling-Atlas for the OFC and the Oxford-GSK-Imanova Striatal Connectivity Atlas for the ventral striatum. 42,43 For each participant, the mean activation level (expressed as percentage signal change) during the contrasts of interest (reward anticipation, neutral anticipation, reward outcome, and neutral correct outcome) was calculated over all the voxels of each ROI.
These values were used in a repeated-measures ANOVA, testing for main within- and between-subject effects in activation levels between rewarding and nonrewarding trials with respect to reward anticipation and reward outcome.
Confirmatory analysis
In case of a negative finding, to ensure that we did not miss activation over time or between groups in regions neighboring the ventral striatum and known to be active during reward anticipation, we confirmed our findings by repeating the repeated-measures ANOVA on the caudate nucleus.
Multiregion analysis across the reward network
To verify that there were no missed between-group differences in the change in activation levels over time in regions other than the ROI involved in reward processing, we conducted an multivariate analysis of variance (MANOVA). See Supplementary Digital Content S2 for a figure showing the analyzed regions other than the ROI.
Results
Demographics
From July 9, 2015, to May 11, 2017, a total of 59 potential participants were screened, 1 of them not meeting the eligibility criteria (Fig. 2). Of the 58 participants randomized (2:1), 41 were assigned to the intervention group and 17 to the control group. A total of 11 intervention participants were lost to follow-up or excluded from analysis, because they withdrew their consent due to lack of time (4), side effects of FTC/TDF/RPV (1), emigration abroad (1), because the investigator withdrew consent because the participant did not understand the fMRI task sufficiently (1), intracranial pathology was found during the MRI scan (1), the quality of the MRI scan was inadequate (2), or due to a VL of more than 200 copies/mL (1).
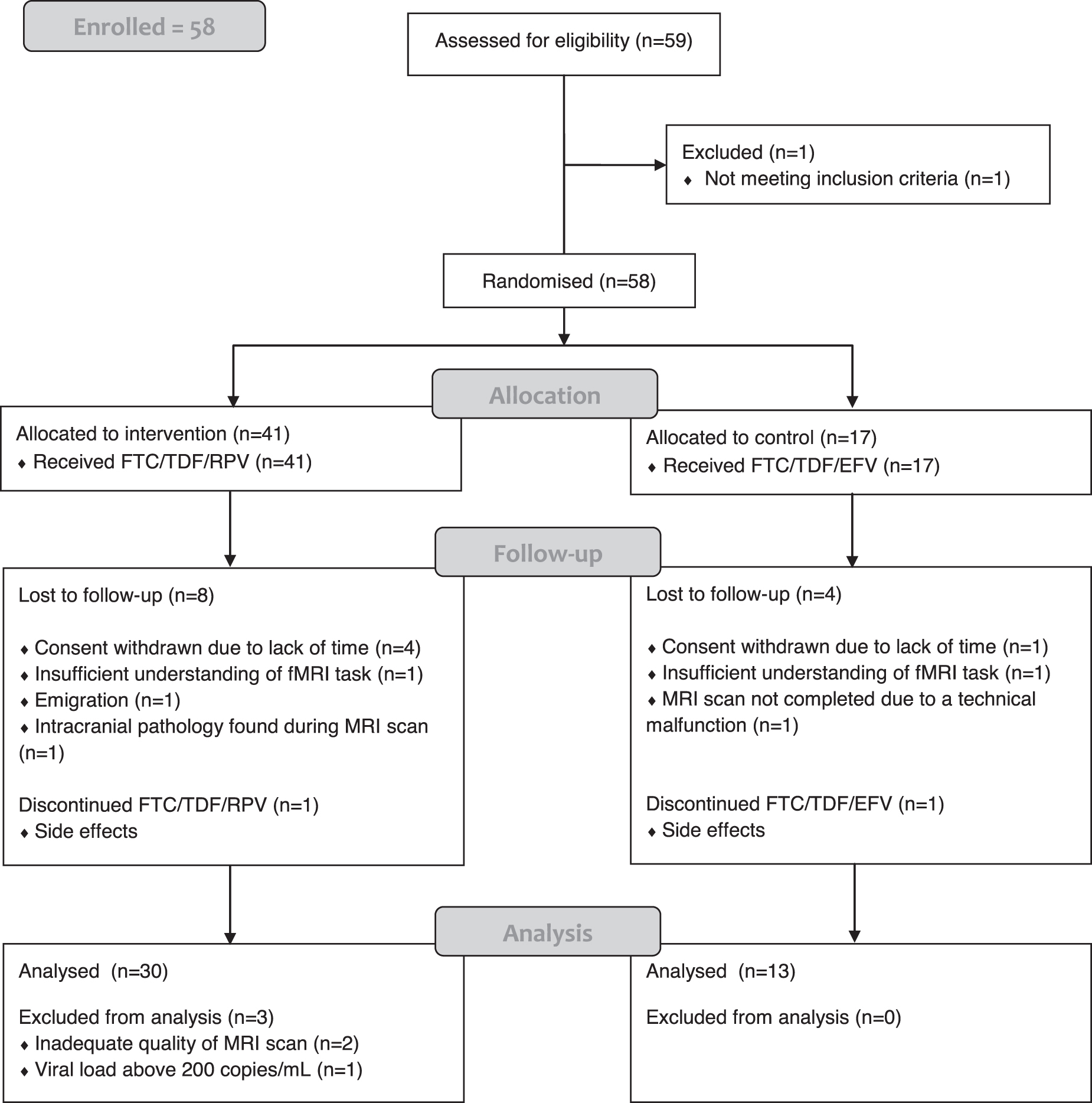
Trial flowchart. Flowchart of participants enrolled and included in our analysis. EFV, efavirenz; fMRI, functional magnetic resonance imaging; FTC, emtricitabine; RPV, rilpivirine; TDF, tenofovirdisoproxil fumarate.
Of the 17 controls who continued FTC/TDF/EFV, 4 participants were lost to follow-up or excluded from analysis because of withdrawal of consent due to lack of time (1), discontinuation of FTC/TDF/EFV during the study due to side effects (1), insufficient understanding of the fMRI task (1), or failure to complete an MRI scan due to technical error (1). This resulted in a total of 30 intervention participants and 13 controls in the final analysis.
The characteristics of these 43 participants were similar (Table 1). At baseline, one intervention participant and one control had a viral blip, with a VL of 96 and 166 copies/mL, respectively. No blips were observed at week 12 and one intervention participant had persistent low-level viremia (VLs of 165 and 168 copies/mL at baseline and week 12).
Characteristics of the Study Participants According to Study Arm
All categorical data are expressed as frequency, percentage, and all continuous data are expressed as median, IQR, unless indicated otherwise.
Missing data: time on EFV [one control (2.3%)], time on cART [one control (2.3%)], nadir CD4 [two intervention participants (4.7%)], CD4 at week 12 [two intervention participants (4.7%)].
ANI, asymptomatic neurocognitive impairment (according to the Frascati criteria 3 ); BMI, body mass index; cART, combination antiretroviral therapy; EFV, efavirenz; FTC, emtricitabine; IQR, interquartile range; RPV, rilpivirine; TDF, tenofovirdisoproxil fumarate; VL, viral load.
Behavioral results
Assumptions
First, we checked assumptions and assessed the Cook's distance on our outcomes of interest. The maximum Cook's distance was <1.0, which indicated no influential outliers. The Levene's tests yielded nonsignificant results, reflecting homogeneity of variances.
Baseline
Next, we evaluated the task performance of participants. At baseline, we found an expected main effect of trial on response time, with both groups reacting significantly faster on potentially rewarding trials than nonrewarding trials [F(1,41) = 25.07, p < .001]. There was no group-by-trial interaction effect during reward task performance [F(1,41) = 0.00, p = .98], indicating that both groups had a similar longer response time in nonrewarding trials. This shows that both groups performed as expected. Similar results were found with regard to response accuracy. Twelve weeks after therapy switch, response time and accuracy were similar to baseline results.
Prospective analysis after 12 weeks
Afterward, the effect of discontinuing EFV on task performance was examined. When comparing the difference in response time of rewarding and nonrewarding trials between baseline and 12 weeks after therapy switch, we found no main effect of time [F(1,41) = 0.22, p = .64], showing that response time differences remained similar over time. In addition, there was no group-by-time interaction effect [F(1,41) = 0.21, p = .65] and no main group effect [F(1,41) = 0.25, p = .62], indicating that both groups had similar response time differences and that switching to FTC/TDF/RPV did not lead to a significant different response time difference compared with continuing FTC/TDF/EFV. We found similar results for the combined response accuracy when comparing baseline and 12 weeks after therapy switch.
Finally, to confirm that the task successfully controlled for the amount of money won, we compared the reward amount between groups and over time. A similar reward amount at baseline versus after 12 weeks [F(1,41) = 0.03, p = .87] was found. There was no group-by-time effect [F(1,41) = 0.18, p = .68] nor main group effect [F(1,41) = 1.03, p = .32], indicating that both groups won a similar amount of money at both time points. This was expected as task difficulty was individually adjusted to ensure an equal reward amount for all participants.
Imaging results
Task validation
First, we started with the validation of the fMRI task. We found significant increases in activation in the ventral striatum during reward anticipation [F(1,41) = 17.20, p < .001; F(1,41) = 41.64, p < .001] and during reward feedback in the OFC for both time points [F(1,41) = 17.20, p < .001; F(1,41) = 41.64, p < .001], demonstrating that the task functioned as expected at both time points.
Reward processing in the ventral striatum
We then investigated the effect of discontinuing EFV on reward anticipation. We found a main effect of time in the combined ventral striatum [F(1,41) = 6.69, p = .01], indicating that the ventral striatal responses of anticipation between rewarding and nonrewarding cues significantly increased in both groups over time (Fig. 3). There was no group-by-time interaction [F(1,41) = 0.57, p = .46] demonstrating that these responses did not differ between the two groups over time. Finally, there was no significant main group effect [F(1,41) = 1.06, p = .31], indicating both groups showing similar responses.
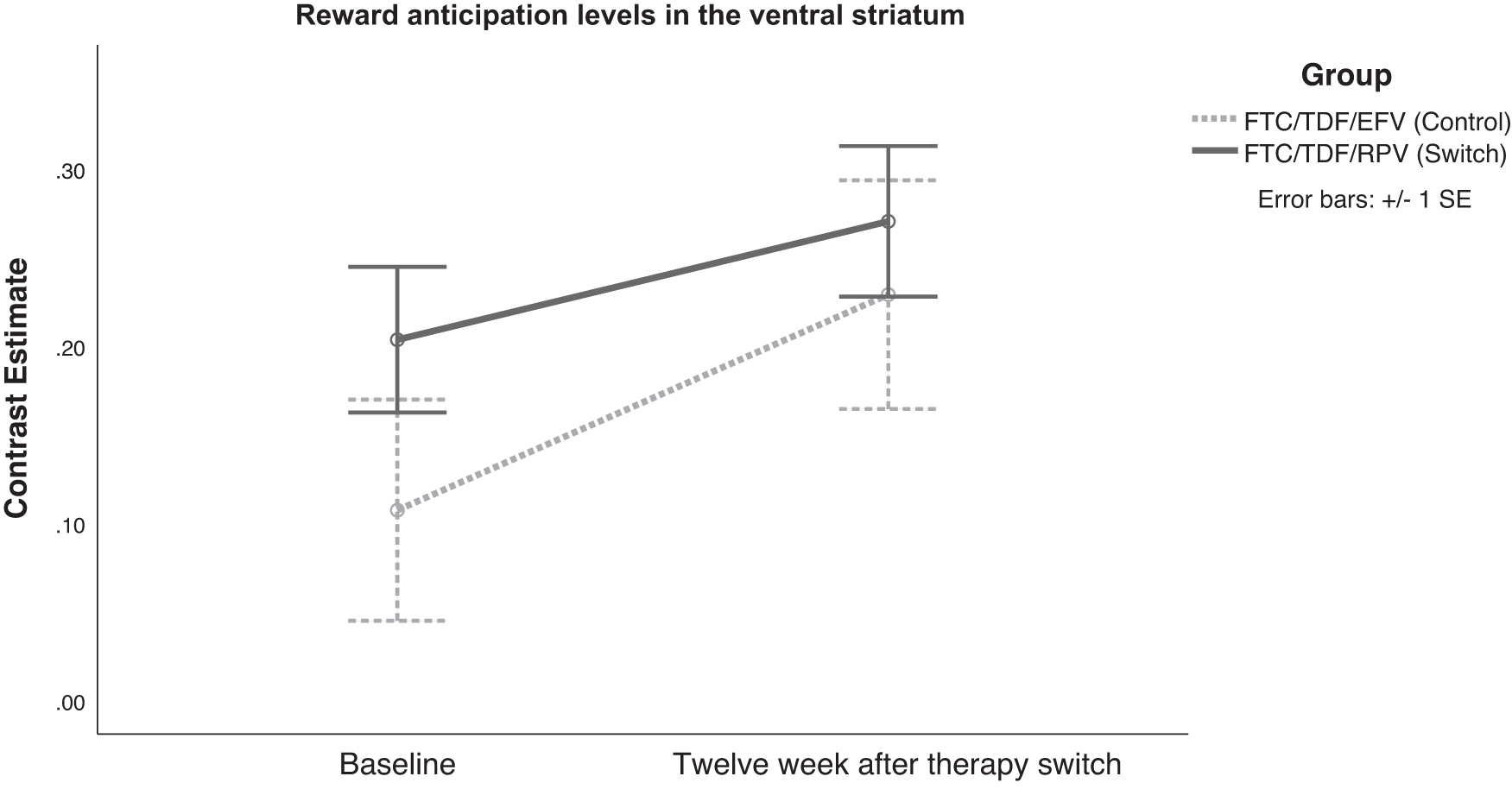
Reward anticipation levels in the ventral striatum. Line graph showing the repeated-measures analysis of activation levels in the ventral striatum at baseline and 12 weeks after therapy switch for the control group (FTC/TDF/EFV) and the intervention group (FTC/TDF/RPV).
Reward processing in the OFC
Subsequently, we assessed the effect of discontinuing EFV on reward outcome processing. We found no significant main effect of time in the combined OFC [F(1,41) = 0.67, p = .42], indicating similar OFC responses in reward outcome over time. As expected, we found no group-by-time interaction [F(1,41) = 0.20, p = .66] nor a significant main group effect [F(1,41) = 0.95, p = .34], showing that OFC responses between groups were similar and remained similar over time.
Confirmatory analysis
Similar to what we did with the ventral striatum during reward anticipation, we proceeded to investigate the caudate nucleus, which neighbors the ROI. We found comparable results, with increased activation levels over time [F(1,41) = 5.57, p = .02] and no significant group-by-time interaction or between-group differences, thus confirming our prior findings.
Multiregion analysis across the reward network
Finally, we assessed whether discontinuing EFV resulted in changes in activation levels in regions other than the ROI involved in reward processing (Supplementary Digital Content S2). No between-group changes were found [F(10,32) = 1.80, p = .10], indicating no additional results. See Supplementary Digital Content S3 for the uncorrected voxelwise whole-brain activation (p < .001) during reward anticipation of all participants at baseline and both study groups 12 weeks after switch.
Discussion
To our knowledge, this multicenter RCT was the first investigating the effect of EFV on reward processing using BOLD fMRI. At the behavioral level, apart from the expected improvement in response time and accuracy between rewarding and nonrewarding trials, no differences were found between groups or over time. Second, we found that discontinuing EFV did not result in improved ventral striatal responses. Both groups did have a similar significant increase in ventral striatal activation at follow-up assessment. Finally, we established that cortical functioning was not affected by discontinuing EFV.
Multiple in vitro studies have demonstrated that EFV is neurotoxic 44,45 and previous BOLD fMRI studies have also reported a negative effect. 26,27 We were therefore surprised that our study found no improvement in behavioral responses after switching from EFV to RPV. Behavioral analyses did show that both groups had faster response times and accuracy during rewarding trials at both assessments. This is consistent with prior studies reporting similar results in both PLWH and healthy controls and ruled out task incomprehension as a possible explanation for this negative result. 21,33,34 One explanation may be that EFV's neurotoxic effect only affects certain PLWH, depending on their specific characteristics. Our study population consisted of a homogeneous group of asymptomatic men with a relatively high level of education and a median age of 42 years, which may have been characteristics protecting them from EFV's neurotoxic effect.
Indeed, the first fMRI study finding a negative effect of EFV was conducted in young adolescents undergoing active neurodevelopment, which may have made them more vulnerable to neurotoxicity. 26 The other was conducted in an older population with longer diagnosed HIV, both factors that may have also made them more susceptible to neurotoxicity. 27 In addition, as age itself has a major influence on fMRI brain function, results might not be entirely comparable. 36,37,46
With respect to functional brain activity, we found a significant increase in activation levels related to reward anticipation in its commonly associated subcortical regions (i.e., the ventral striatum) over time in both groups. As this was observed across groups, we believe this can be attributed to a learning effect due to repetition of the fMRI task. However, contrary to our hypothesis, no effect of discontinuing EFV was found. This again was surprising as the aforementioned fMRI studies did find EFV-related functional differences in the subcortical regions associated with proactive inhibition and with response inhibition, although the results from the second study were not significant after correction for multiple comparisons. 26,27
It may therefore be that EFV affects specific parts of the fronto-striatal network, as these fMRI studies examined executive functioning, rather than reward processing. 26,27 Previous studies have shown that HIV-infection impairs the fronto-striatal-parietal network, which is involved in visual attention, working memory, and motor control. 5,25,47 These areas may thus be susceptible to EFV in contrast to the reward system, which is located in the ventral fronto-striatal network. Nevertheless, not all studies support this hypothesis, as shown by Payne et al who assessed attentional processing, which is located in the fronto-striatal-parietal network, but found no difference in brain activation after discontinuing EFV. 15 Finally, although our sample size was large for an fMRI study, especially compared with other prospective fMRI studies, 15,27 we cannot rule out the possibility that our negative finding was due to too small a sample size.
We found that discontinuing EFV did not affect cortical functioning. This was in line with our hypothesis and previous research showing that HIV-infection primarily affects subcortical functioning. 25,37 Even though chronic antiretroviral therapy has been associated with greater cortical activation, since both study groups had a comparable time on antiretroviral therapy, this should not have confounded our results. 48
The present study has several strengths. The main strength is our design, as conducting an RCT ensured that all known and unknown confounders were similar across groups. Other prospective fMRI studies were single-arm and compared participants before and after therapy switch. 15,27 Our control group and longitudinal design allowed us to distinguish learning effects and thus to properly compare the effect of switching to FTC/TDF/RPV versus continuing FTC/TDF/EFV. Moreover, as mentioned, our sample size was large for a prospective BOLD fMRI study. Lastly, strict inclusion and exclusion criteria meant that known fMRI confounders such as age, gender, drug use, and psychiatric disorders were either homogenous in our population or excluded, enabling us to adequately assess EFV with BOLD fMRI.
Certain limitations apply to our study. First, the power calculation was not performed for this subanalysis, which may have resulted in insufficient power. In addition, a considerable number of participants were lost to follow-up or excluded from analysis. However, except for one participant from each study group withdrawing due to side effects, the reasons for exclusion or lost to follow-up were unrelated to our determinant or outcome. We therefore believe this did not result in bias.
Conclusions
This study showed that discontinuing EFV did not lead to improved activity related to reward anticipation in asymptomatic PLWH. It is therefore likely that EFV does not affect motivational control. Further research is needed to determine whether EFV affects motivational control in HIV populations with different characteristics.
Footnotes
Acknowledgment
The authors would like to thank Matthijs Vink for his help in designing and executing the study.
Authors' Contributions
J.E.A. designed the study. C.S.H. wrote the study protocol under the supervision of J.E.A. C.S.H. and P.P. were responsible for the site work including the recruitment, follow-up, and data collection. All authors had access to data. P.G.A.O. performed the analysis, interpreted results, and drafted the article in close collaboration with S.d.P. and B.J.v.W. All authors contributed to the interpretation of the data, critically reviewed the article, and approved the final article.
Ethics Approval,Patient Consent,and Clinical Trial
Data Availability
The data that support the findings of this study are available from the corresponding author, B.J.v.W., upon reasonable request.
Author Disclosure Statement
J.E.A. has received advisory board fees from ViiV Healthcare. B.J.v.W. has received a research grant and speaker fees from Gilead Health Sciences, has received speaker and advisory board fees from ViiV Healthcare: all fees were paid to the institution. For the remaining authors, none was declared.
Funding Information
This study was funded by Gilead Sciences. The funder had no role in the trial design, data collection or analysis, or drafting of the article.
Supplementary Material
Supplementary Digital Content S1
Supplementary Digital Content S2
Supplementary Digital Content S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.