
Abstract
Since the introduction of modern antiretroviral treatment for HIV and hepatitis C virus (HCV), the pattern of autoimmune diseases (ADs) in people living with HIV (PWH) might have changed. This is a retrospective study in a cohort of 5,665 PWH at the HIV Clinic of Hospital Universitario La Paz (Spain) to estimate the prevalence of ADs from January 1990 to June 2020. We divided the timeline into four periods: <1996, 1996–2006, 2006–2015, and 2015–2020. In total 369 participants were diagnosed with at least one AD, with a prevalence of 5.3% (95% confidence interval 4.7–5.9). In total, 302 (81%) participants were diagnosed simultaneously or after HIV diagnosis. Most prevalent diseases were immune thrombopenia (IT) (n = 90), cutaneous psoriasis (n = 52), autoimmune thyroid disorders (n = 36), spondylarthritis (n = 24), and inflammatory bowel disease (IBD) (n = 21). There was a significant trend for more ADs in recent periods (p = .037). In recent years, participants with ADs were older, had a long time since HIV diagnosis, and had higher CD4+ T cell count and higher CD4+ T cell nadir (temporal linear trend p < .001). There was a change in the pattern of ADs over time with a decrease in IT and an increase in spondylarthritis, arthritis, IBD, and thyroid disorders. One hundred thirty-nine participants (46%) were coinfected with HCV, with a steady decline throughout the study period. Only cryoglobulinemia was statistically associated with HCV infection. AD increases over time in PWH with reasonable immune virological control. We observed a higher frequency of spondylarthritis, arthritis, autoimmune thyroid disorders, and IBD in recent years.
Introduction
Modern antiretroviral therapy (ART) and universal treatment access have led to a remarkable reduction in morbidity and mortality in people living with HIV (PWH). 1 However, despite the control of viral replication and the recovery of CD4+ T cell count, chronic inflammation and low-level replication contribute to a state of immune dysregulation. 2,3
The relationship between HIV infection and autoimmunity is a well-known phenomenon. In common with other immunodeficiency disorders and viral infections, there is an imbalance of the immune system and the different cellular components that can favor the development of autoimmune diseases (ADs), for example, reactivation of latent infections such as Epstein–Barr virus, variation of T cell populations, inversion of CD4:CD8 ratio, increase of the intestinal barrier permeability, and the persistent viral replication itself. 4,5 It is not uncommon to find high titers of autoantibodies in some PWH, even with CD4+ T cell count >500 cells/mm3 and viral suppression. However, autoantibodies do not correlate with the prevalence of ADs in PWH. 6
In early 2000, Zandman-Goddard and Shoenfeld postulated that depending on the CD4+ T cell count, the viral load, and the clinical stage of HIV infection, the type of autoimmunity occurring might change according to the principal immune disorder: immune complex formation, CD4:CD8 ratio inversion, and immune restoration. 7 Whether this statement is still valid in the current ART era remains to be elucidated.
Previous studies have enormous variability in the prevalence of ADs in PWH, depending on the entities included in the analysis and the study's time frame. Studies reviewing the association of HIV infection and ADs before 2000 estimated a prevalence between 1% and 60%. 7 More recently, several studies have estimated a prevalence of ADs of 5%–10% and a higher incidence of specific AD in PWH than in the general population. 8 –10 Some authors have demonstrated a change in the pattern of AD after the introduction of the modern highly active antiretroviral treatment (HAART), and it has been suggested that some integrase inhibitors might contribute to AD due to a hypothetical higher risk for immune reconstitution inflammatory syndrome (IRIS). 11 –13
Historically, coinfection with hepatitis virus has been common in PWH, and mainly hepatitis C is associated with developing some Ads such as cryoglobulinemia, thyroiditis, or glomerulonephritis. Moreover, historical treatments for hepatitis C virus (HCV) such as interferon and ribavirin are also linked to immune-based disorders. The efficacy of the new antiviral agents could have contributed to a different profile in the AD diagnosed in coinfected patients in recent years.
We hypothesize that the pattern of AD diagnosed in PWH has changed over time concerning the better efficacy and safety of ART and the eradication of HCV infection. Also, in the current era, AD diagnosis is more frequent due to the better control of HIV infection with the restoration of immune function.
This study aims to estimate the prevalence, temporal trend, and different profiles of AD diagnosed in PWH in a large Spanish single-center cohort.
Materials and Methods
Study design and participants
We designed a retrospective cohort study reviewing the clinical records of PWH under routine clinical care in the HIV clinic of La Paz University Hospital in Madrid (Spain) who had ever been diagnosed with an autoimmune disorder from January 1990 to June 2020. Only those participants with at least two clinical visits were included. During the study, 5,665 PWH had at least two annual visits to the clinic and, therefore, were the reference population.
Baseline variables included in the cohort were year of birth, gender, a risk factor for HIV acquisition, race, HIV duration, Centers for Disease Control and Prevention stage at HIV diagnosis, CD4+ T cell count at AD diagnosis, CD4+ T cell nadir count, HIV viral load at AD diagnosis, coinfection with HCV or HBV, and treatment for HCV.
We included the following ADs: immune thrombopenia (IT), autoimmune hemolytic anemia (AIHA), cutaneous psoriasis, arthritis (rheumatoid, reactive, inflammatory), spondylarthritis (reactive, inflammatory, psoriasis, and ankylosing), inflammatory bowel disease (IBD) (ulcerative colitis and Chron disease), autoimmune thyroid disease (ATD), autoimmune hyperthyroidism, autoimmune hypothyroidism, glomerulonephritis, cryoglobulinemia, uveitis, vasculitis, antineutrophil cytoplasmic antibodies vasculitis, IgA vasculitis, panarteritis nodosa, antiphospholipid syndrome, systemic lupus erythematosus, cutaneous lupus, celiac disease, autoimmune hepatitis, Guillain–Barré, myasthenia gravis, optic neuritis, inflammatory myelitis interstitial lymphoid pneumonia, myositis, sarcoidosis, primary biliary cholangitis, Beçhet disease, and Castleman disease.
Owing to the heterogeneity published in the literature referring to the classification of arthritis and spondylarthritis, for this analysis, we classified as “reactive” when the disease was secondary to an immune response to an identified infective agent and “inflammatory” when idiopathic or attributed to HIV.
We divided the study's timeline into the following periods: <1996, 1996–2006, 2006–2015, and 2015–2020. The rationale for these periods was to differentiate the pre-HAART era, the protease inhibitors era, the introduction of the integrase inhibitors, and the current ART dominated by the integrase inhibitors single-tablet regimens and dual therapies.
We differentiate the AD diagnosed simultaneously or immediately after HIV diagnosis (in the previous or the year after HIV enzyme-linked immunosorbent assay positivity) to discriminate the possible role of HIV infection or the inflammatory reconstitution syndrome.
Ethics
This study fulfilled the local legal and ethical requirements and was conducted according to the Declaration of Helsinki. The ethics committee approved the study protocol of Hospital La Paz (PI-4276). Owing to the retrospective design, a written informed consent waiver was obtained.
Statistical methods
Quantitative data were described as median (p25–p75) and qualitative data as number (percentages). Quantitative variables were compared using the Student t or Mann–Whitney U test [or analysis of variance (ANOVA)/Kruskal–Wallis test] as appropriate and qualitative variables using the chi-square or Fisher's exact test. The linear trend test on proportions was tested with the linear-by-linear chi-square and Spearman's rank correlation coefficient. The prevalence of ADs with 95% confidence intervals (CIs) was calculated considering diseases as patients (as most patients had only one AD).
The CIs were estimated with the Exact (Clopper–Pearson) method. Two-sided tests were used, and a p value <.05 was considered statistically significant. All analyses were performed using SAS Enterprise Guide 8.2. (Cary NC, SAS Institute, Inc.).
Results
In this cohort, 369 participants were diagnosed with at least one AD (67 before HIV diagnosis, 93 simultaneous, and 209 after HIV diagnosis). The prevalence of ADs in the whole cohort was 5.3% (95% CI 4.7–5.9). The distribution during the study period was as follows: <1996 (n = 54; 17.8%), 1996–2006 (n = 66; 21.8%), 2006–2015 (n = 126; 41.7%), and 2015–2020 (n = 56; 18.5%). This increase in the frequency of ADs over time was statistically significant (temporal linear trend; p = .037).
In total, 322 autoimmune episodes occurred in the 302 patients diagnosed simultaneously or after HIV diagnosis (Supplementary Table S2). The most frequent ADs found in the whole cohort were IT (n = 90), cutaneous psoriasis (n = 52), spondylarthritis (n = 24), IBD (n = 21), arthritis (n = 18), autoimmune hyperthyroidism (n = 21), and autoimmune hypothyroidism (n = 15), taken together ATD (n = 36).
Baseline characteristics of those with ADs diagnosed simultaneously or after HIV diagnosis are given in Table 1. In brief, most of them were Caucasian (92%), male (n = 212; 70.2%), with a median (p25–p75) age of 39 (31–47) years, and 46% were coinfected with HCV. CD4+ T cell count at AD diagnosis was 438 (221–677) cells/mm3, and the median time from HIV diagnosis to AD was 78.8 (6.9–186.1) months. As expected, due to changes in the epidemiology of HIV infection in our country, sexual HIV acquisition was predominant from 1999 onward.
Baseline and Per Period Characteristics of Patients Diagnosed Simultaneous or After HIV Diagnoses (n = 302)
Data presented as median (p25–p75) or n (%).
The percentage was calculated with the number of patients with HIV viral load performed that was 243 overall and 19, 56, 114, and 47, respectively, for each period.
AD, autoimmune disease; CDC C, CDC stage (Center for Disease Control and Prevention) Stage C; ELISA, enzyme-linked immunosorbent assay; HBV, hepatitis B virus; HCV, hepatitis C virus; IDU, intravenous drug user; MSM, men who have sex with men; MSW, men who have sex with women; NS, not statistically significant.
In recent periods, participants diagnosed with AD had a higher CD4+ T cell nadir, a higher CD4+ T cell count, and fewer participants had a viral load >50 copies/mL (p < .001). The median time from HIV diagnosis to AD diagnosis significantly increased over time from 6.8 (4.8–33.7) months before 1996 to 202 (78.7–298.9) months in the period between 2015 and 2020 (temporal linear trend p < .001).
Every AD episode diagnosed simultaneously or after HIV infection over the study periods is represented in Supplementary Table S1. Globally, IT and cutaneous psoriasis were the most prevalent. The AD profile changed over time, showing a decrease in the frequency of IT, whereas spondylarthritis, IBD, arthritis, and ATD increased (Fig. 1). The correlation between the number of patients and the study periods was the following: IT (rho = −0.95), cutaneous psoriasis (rho = 0.8), IBD (rho = 0.8), spondylarthritis (rho = 0.8), ATD (rho = 0.4), and arthritis (rho = 0.95).
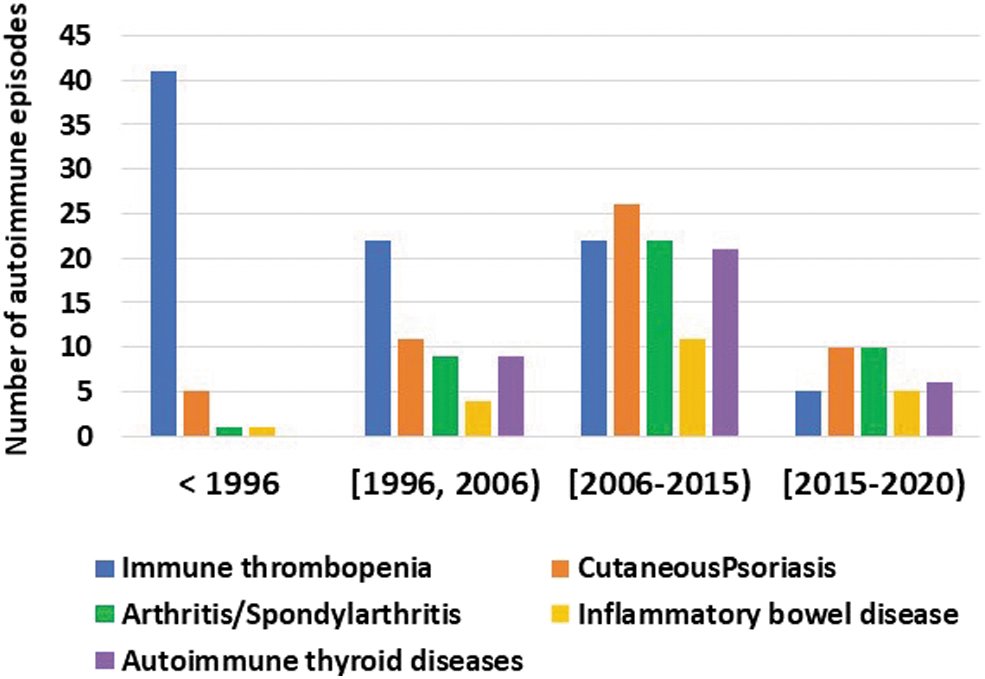
Temporal trend prevalence of the patients diagnosed with ADs simultaneous or after HIV diagnoses (n = 302). ADs, autoimmune diseases.
Although the correlation coefficients are high, these were not statistically significant due to the low number of diseases. However, the research for the temporal trend in the pattern of different AD diagnoses over time was statistically significant (p = .002). The main characteristics of the most prevalent AD diagnosed simultaneously or after HIV diagnosis are given in Table 2.
Characteristics of Autoimmune Disease Episodes Diagnosed Simultaneously or After HIV Diagnosis
Shown only those entities with >15 episodes and subtypes.
Data presented as median (p25–p75) or n (%).
Coinfection with HCV was diagnosed in 139 out of 302 participants (46%). The frequency of coinfection with HCV was higher in the early periods; 70.4% of the participants with an AD diagnosed before 1996 were HCV coinfected, in contrast with 37.5% between 2015 and 2020 (Table 1). HCV-coinfected participants had a lower CD4+ T cell nadir (130 vs. 233 cell/mm3; p < .05), a lower CD4+ T cell count at AD diagnosis (373 vs. 497 cell/mm3; p < .05), and longer time to AD diagnosis (121.8 vs. 66.9 months; p < .05) than HIV monoinfected participants. Only 17 out of 302 (5.6%) patients were coinfected with HBV, and we did not find any association with ADs.
Cryoglobulinemia was the only disorder with a higher frequency in HCV-coinfected participants (0 vs. 10; p < .001). No other AD was found statistically associated with HCV or HBV in comparison with HIV monoinfected participants. We did not find any association between HCV treatment with direct antivirals and the frequency of AD diagnosis. Only two participants were diagnosed with AD in the year after interferon plus ribavirin treatment (one psoriatic spondylarthritis and one AIHA).
Discussion
We present a retrospective cohort of PWH followed for 30 years showing an AD prevalence of 5.3% (95% CI 4.7–5.9). The most prevalent diseases were IT, cutaneous psoriasis, arthritis, spondylarthritis, IBD, and ATD, and globally ADs increased.
Previous studies demonstrated a prevalence of ADs ranging from 3% to 71% in the pre- or early HARRT era. 7,14 This could be mainly explained by the different entities included. Most articles focus on rheumatic manifestations, a broad term covering both immune and nonimmune-related disorders such as musculoskeletal infections or avascular bone necrosis. 15 –17 Moreover, other pre-HAART studies focused mainly on immune-mediated musculoskeletal diseases such as arthritis without including systemic immune-mediated diseases. 15,18,19
The prevalence of ADs in PWH in the studies performed in the post-HAART era is more precise and similar to the results of our analysis, with some exceptions. Lebrun et al found a prevalence of 6% in a 33.403F cohort of PWH followed from 2000 to 2013, 8 and Damba et al reported a prevalence of 9.6% in the Canadian cohort followed from 1996 to 2011. 10 These articles included entities similar to our analysis, but they did not capture AD episodes before 2000, precluding obtaining any conclusion about the temporal trend. Virot et al had 5,186 PWH followed from 2003 to 2013 and showed a prevalence of 0.6%, excluding some of the most prevalent ADs as IBD, cutaneous psoriasis, or spondyloarthropathy. 20
The selection of the diseases included is critical to make comparisons and differences in populations studied due to the different incidence of some ADs among races and geographic location, 21 which may explain some differences between European studies and the study on Taiwanese cohort.
The most frequent reported ADs in the pre-HAART era were those triggered by HIV, such as IT, myositis, and diffuse infiltrative lymphocytosis syndrome (DILS), or those attributed to a great reduction CD4:CD8 ratio, such as psoriatic arthritis or reactive arthritis. 14 Cutaneous psoriasis had classically been associated with an advanced state, given that psoriasis is supposed to be a CD8+ T cell-mediated disease. 7 In the post-HAART era, there has been a change in the pattern of ADs with the increase of some disease such as ATD or sarcoidosis, whereas IT and cutaneous psoriasis remain still prevalent.
Remarkably, most ADs in our cohort were diagnosed after HIV diagnosis. This fact contrasts with the classical theory that AD in PWH was more frequent in advanced states or during the immune reconstitution syndrome and scarce in long-term aviremic patients. 7
In our cohort, we observe a decrease in IT and an increase in IBD and autoimmune thyroid disorders. The change in the spectrum of AD in HIV infection in our cohort over time could be partially explained by the better immune reconstitution associated with the earlier initiation of ART and newer antiretroviral drugs. The scarcity of entities such as SLE, rheumatoid arthritis, or myopathies could be with the low number of females in our cohort, although these ADs are also less frequent in other cohorts. 8 –10
Our results are somewhat different from what is already published regarding arthropathies, represented mainly by inflammatory, psoriatic, and reactive articular arthritis and spondylarthritis. Our study found an increase in the number of arthritis/spondylarthritis over time. Studies in the pre-HAART era, in settings where intravenous drug use was the main HIV risk acquisition factor, found a low number of arthritis/spondylarthritis. 15 In our cohort, arthropathies increased over time. This fact could be related to the increase in HIV infections sexually acquired by men who have sex with men, a subgroup with a high risk for sexually transmitted infections as the predominant group.
Differences in the ethnic background of the populations included are also responsible for these differences in the spectrum of ADs among the studies. For example, the study by Yen et al showed an increased risk of incident Sjögren syndrome, psoriasis, systemic lupus erythematosus, AIHA, and uveitis. Except for psoriasis, the rest of ADs were barely diagnosed in our cohort. More extensive studies with standardized definitions of AD and geographically diverse are needed to characterize better the temporal trend and differences of ADs in PWH.
Interestingly, the increase in life expectancy and aging in PWH could contribute to the increase in autoimmunity. Immunosenescence, chronic inflammation, and chronic viral infections could affect the balance between T cell subpopulations (T-regs, Th-17), and select autoreactive T cells contributing to autoimmunity. 22
The low prevalence of DILS, sarcoidosis, and inflammatory myositis in our cohort is remarkable compared with previous reports. 8,11,23 –25 DILS was probably misdiagnosed as it might require a biopsy or specific diagnostic test. It could be paucisymptomatic and presumably improve after starting ART. However, we did find four cases of interstitial lymphoid pneumonia, all in the context of mother-to-child transmission, which is part of the DILS spectrum. In our study, the earlier ART initiation since 2015 and the diagnosis of ADs with higher CD4+ T cell count could explain the absence of these ADs, typically associated with profound immunodepression and CD8+ T cell activation.
The AD diagnosed in the past decades of this study was primarily organ specific and not related to immune depression or a decrease in CD4+ T cells. Over the past decades in the study, PWH with ADs were older, had a higher CD4+ T cells count, higher CD4+ T cells nadir, more patients were with undetectable viral load, and had a longer time from HIV diagnosis to AD. This could reflect a better immunological situation. The mechanisms underlining autoimmunity in PWH with high CD4+ T cell count and virological control are not entirely understood. Pathogenic ways such as molecular mimicry, epitope spreading, bystander activation, production of extracellular neutrophil traps, or polyclonal activation might play a role. 26
Despite the high percentage of HCV-coinfected participants in the whole cohort, and contrary to a previous report, 10 we did not find any difference in the prevalence of ADs compared with the HIV-monoinfected individuals. We also did not find a relationship between HCV treatment and the development of any AD. This contrasts with previous analysis showing an association between HCV coinfection and cutaneous psoriasis, AIHA, Grave's disease, and IT. 8
The study's limitations are those inherited from an observational retrospective study, especially in an old cohort with some variables missing in the medical records. The AD diagnosis was based on medical history and lacked a standardized definition. We cannot exclude the influence of higher mortality in the earlier periods as a competing risk. We did not perform a competing risk analysis due to the lack of quality data. Sarcoidosis might clinically overlap with IRIS. This term was not included in our study protocol because it might be related to latent infections rather than autoimmune phenomena.
The rarity of these diseases and the low number of some made it difficult to obtain more information about individual risks and entities, such as the possible role of antiretroviral drugs. Finally, the lack of a control group of HIV uninfected individuals impeded us from analyzing any differences with the general population.
Conclusions
This sizeable Spanish cohort shows that the AD in PWH is frequent and increases over time. The AD profile in this cohort has changed depending on the HAART era, with an increase in IBD, ATD, spondylarthritis and arthritis, and a decrease in immune thrombocytopenia.
Footnotes
Acknowledgments
We thank our patients attending the HIV clinic in Hospital La Paz. This study fulfilled the local legal and ethical requirements and was conducted according to the Declaration of Helsinki. The ethics committee approved the study protocol of Hospital La Paz (PI-4276). Owing to the retrospective design, a written informed consent waiver was obtained. No material from other sources was reproduced.
Authors' Contributions
L.R.-R., C.B., J.I.B., and A.R.-M. designed and oversaw the study. L.R.-R., C.B., A.D.-V., A.D.-H., and J.I.B. accessed and verified the data. L.R.-R., C.B., and J.I.B. wrote the first draft of this report. All authors acquired the data, reviewed and amended the draft report, and approved the final version. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.