
Abstract
The polymorphisms in host genes such as CCR5, CCR2, stromal derived factor (SDF), and MBL (mannose-binding lectin) as well as the viral nef gene have been shown to influence human immunodeficiency virus (HIV) infection, followed by the development of HIV-associated neurocognitive disorder (HAND). In this preliminary study with a limited number of samples, we have tried to associate the genetic polymorphism from the host and viral genetic factors with the neurocognitive status along with immuno-virological parameters. The total RNA was isolated from 10 unlinked plasma samples containing 5 samples from each group with and without HAND based on the International HIV Dementia Scale (IHDS) score <9.5 and >9.5, respectively. The CCR5, CCR2, SDF, MBL, and HIV nef genes were amplified and digested with restriction enzymes, except for the nef gene amplicon. Restrictions fragment length polymorphism (RFLP) was used to determine whether allelic variations were present in the digested host gene products, while sequencing was done for HIV nef amplicons without digestion. CCR5 delta 32 heterozygous variants were present in two samples from the HAND group. Three samples with HAND showed SDF-1 3′ heterozygous allelic variant, while the MBL-2 gene presented with a homozygous mutant allele (D/D) in codon 52, heterozygous mutant allele (A/B) in codon 54, and codon 57 (A/C) for all samples except IHDS-2 irrespective of dementia status. Furthermore, amino acid alignment of Nef sequences confirmed the heterogeneity, while prediction of the human leukocyte antigen binding epitopes further explored its effect on functional motifs with variable binding efficiency such as epitopes GAFDLSFFL (aa 83) and LTFGWCFKL (aa 138) binding with HLA molecules at 60% and 80%, respectively. Thus, host genetics evidently influence predisposition to HIV infection and HAND. The genetic variability in the nef gene from both groups resulted in altering the functionality of specific domains and showing its impact on the progression of the disease, which needs to be explored.
Introduction
The human immunodeficiency virus (HIV) epidemic is a global public health problem, especially in developing nations. 1 In the absence of antiretroviral therapy (ART), HIV infection aggravates to the development of AIDS and damages the brain cells causing HIV-associated neurocognitive disorder (HAND). Hence, significant neurological complications developing milder forms of HAND and HIV-associated dementia have been reported. India has a prevalence of 33%–45% for HAND while 60% in other countries. 2,3 In the combination ART era, the prevalence of HAND needs to be explored to understand the role of polymorphisms in the host genes such as CCR5, CCR2b, stromal derived factor (SDF), mannose-binding lectin (MBL), and certain viral proteins. The association between them needs to be explored to improve existing therapeutic strategies.
The role of various chemokines and chemokine receptors in HIV pathogenesis, transmission, and related cognitive impairment is very well reported. 4,5 However, the uncertainty in the measurement of disease outcome, its severity, and genetic polymorphism in various host factors results in the irregular presentation of HAND. CCR5 co-receptor is one of the most critical co-receptors modifying the progression of the disease to AIDS. 6,7 The occurrence of the homozygous CCR5-Δ32/Δ32 allele provides complete protection against HIV infection leading to the production of an aberrant CCR5 protein, whereas CCR5-wt/Δ32 forms a heterozygous allele providing limited protection with a reduction in the rate of disease progression. 8,9 The expression of chemokines and their receptors has been reported from the central nervous system responsible for modulating the inflammatory response facilitating neurocognitive impairment. 10
Like CCR5, CCR2 and its ligand, monocyte chemoattractant protein-1 (MCP-1), are also involved in neuropathogenesis. 11 The substitution of isoleucine by valine at the 64 amino acid position is linked with the slow progression of the disease in HIV-positive individuals. 12,13 SDF gene is also associated with altered HIV disease course with guanine/adenine (G/A) transition in the 3′ untranslated region and is a unique ligand of CXCR4 co-receptor. This mutation has been associated with delayed progression to AIDS in homozygous individuals, particularly in the late stage of the disease. 4,14 Additionally, MBL binds to the carbohydrate moiety of surface protein gp120 of HIV.
The occurrence of variations in the genetic makeup of MBL2, considering codon 52 (rs5030737A/D), codon 54 (rs1800450 A/B), and codon 57 (rs1800451 A/C) from individuals with HAND, has a severe impact on the progression of the disease. 15 However, the effect of the polymorphism from various such receptors in neurocognitive impairment needs to be explored in detail along with genetic variability in the HIV-1 nef viral gene. Hence, apart from host genetic factors, we have amplified the full-length HIV nef gene from all the samples to understand genetic variability in the nef gene and prediction of human leukocyte antigen (HLA) binding epitopes to estimate binding or non-binding scores of various domains of the nef gene to explore its association with neurocognitive impairment.
Materials and Methods
Ethical approval and details of study subjects
Institutional ethics committee approval (IEA) was taken before starting the proposed study. The ethics committee protocol number is NARI-EC/2015-12 Version 1.0, 25/04/2015. The samples were considered after delinking the patient's identities. Demographic information was recorded for all HIV-positive individuals. A battery of neurological parameters such as memory recall, motor speed, and psychomotor speed responsible for identifying neurocognitive status is noted along with the history of antitubercular treatment and ART.
Assessment criteria for calculation of the International HIV Dementia Scale score
Assessment of the International HIV Dementia Scale (IHDS) score was used to understand the presence of dementia in study participants. This commonly used screening technique is significant since it is simple to use and culturally and linguistically neutral. The three tasks that make up the IHDS instrument are each scored on a scale from 0 to 4. The patients were given four words to recall, saying them out one at a time, to measure memory registration. The words were asked to be repeated by the patient. The examiner repeated the words if the patient did not immediately remember all of them. After the motor activities were finished, the patient was asked to recall the words. Semantic hints were provided for terms that were forgotten. Every word the patient remembered was worth one point, each accurate response of their own was worth one point, and each accurate response they received prompting for received 0.5 points.
The patient was instructed to tap as swiftly and broadly as they could on the first two fingers of the nondominant hand to measure their motor speed. The results were as follows: 4 = 15 in 5 s; 3 = 11 in 5 s; 2 = 7 in 10 in 5 s; 1 = 3 in 6 in 5 s; and 0 = 0 in 2 in 5 s. The patient was asked to swiftly do the following actions with their nondominant hand to measure their psychomotor speed. Placing the dominant hand flat on the work surface with the palm down, squeezing it into a fist, and placing the hand perpendicular to the flat surface on the side of the fifth digit are all examples of flat surface poses. The patient was instructed to complete the exercise twice for practice once it was demonstrated to them.
The exercise was evaluated as follows: 4 for completing 4 sequences in 10 s; 3 for completing 3 sequences in 10 s; 2 for completing 2 sequences in 10 s; 1 for completing 1 sequence in 10 s; and 0 for failing to complete. The IHDS score overall was calculated based on the highest score points limited to 12 points. Additionally, the neuropsychological status was assessed based on testing various domains for fluency, speed processing, attention, executive functioning, learning, memory, and motor performance. As this study is focused on viral and host polymorphism, providing detailed information about the study participants on neuropsychological status becomes a limitation.
Amplification of host and nef genes
Viral RNA isolation was performed from 10 plasma samples with and without neurocognitive disorder using the Viral RNA Mini Kit (Qiagen, Studio City, CA). Approximately 500 ng of RNA was used to synthesize cDNA using either gene-specific reverse primers or random hexamers available in the kit (Applied Biosystems, Foster City, CA). The cDNA was considered for amplification of CCR5, CCR2b, SDF, and MBL genes using the primers covering the polymorphism site reported earlier, 16 whereas the HIV full-length nef gene (8797-9414, HXB2) was amplified as per the list of the primers depicted in Table 1. The reaction volume and thermal cycling conditions for amplification of the CCR5 (189 bp), CCR2 (128 bp), SDF (320 bp), and MBL (119 bp) genes were optimized by following the published literature with minor modifications. 17
List of Primers Used for Amplification
MBL, mannose-binding lectin; SDF, stromal derived factor.
Briefly, the PCR conditions for amplification of various genes for this study samples were carried out following initial denaturation at 94°C for 2 min, cycling condition was set to 30 cycles at 94°C for 30 s for denaturation, 55°C for 30 s for annealing, and 72°C for 45 s for extension, followed by final extension at 72°C for 10 min. In all the PCR amplifications, 1.5 mM Mg2+ concentration was kept constant in all PCR master mixes. To confirm the amplicon size, the PCR products were tested by agarose gel electrophoresis using either 1.2% or 4% gel and confirmed the size of the amplicon along with DNA ladder. All these amplicons were digested and resolved on 10% polyacrylamide gel electrophoresis to understand polymorphism. 18
Simultaneously, HIV nef gene was amplified and purified by a gel extraction kit (Qiagen Studio City, CA), followed by quantification using Nanodrop 1000 spectrophotometer. The automated Sanger dideoxy chain termination method was used for sequencing. End products were cleaned by 80 μL of 80% isopropanol to eliminate surplus dye terminators and resuspended in Hi-Di formamide to perform sequencing on 96 capillary genetic analyzer (ABI 3730XL; Applied Biosystems).
Genetic analysis of HIV nef gene sequences
Each base was confirmed from the electropherogram generated in the sequencer (3730XL; Applied Biosystems). The comparison and multiple alignments were carried out using SeqScape software (Version 2.7) using nef gene sequences reported in the database. 19 A consensus of amino acid residues was attained by translating nucleotide sequences, checking codon positions with the correct reading frame using the ExPaSy tool from SIB Bioinformatics Resource Portal as well as MEGA software (Version X), 20 followed by manual checking of the alignment using Bio Edit software, 21 HIV-1 subtyping was performed for the generated nef gene sequences of study samples using HIV Blast tool available online from HIV DATABASE.
Prediction of HLA motif
To identify specific regions of the HLA-1 binding motif from the amino acid sequences of the nef gene, we used the online available link for predicting binding and non-binding epitopes. 22 Predominantly observed HLA motifs in high frequency in the Indian population were included for the prediction of specific epitopes, which are binding to the consensus sequence of the nef gene obtained from the study samples. 23
Results
Detailed demographic information with IHDS score is mentioned in Table 2, while the neurological parameters such as memory recall, motor speed, and psychomotor speed were assessed to get IHDS score (Table 3). It was observed that the viral load for neurocognitive individuals was in multiples of thousands while for those without neurocognition were in only thousands indicating the impact of HIV viral copies on neurocognitive status. Similar was the scenario with CD4 cell counts, although we could not conclude based on a small number of samples from this study.
Demographic and Clinical Information of the Individuals from the Current Study
F, female; IHDS, International HIV Dementia Scale; M, male.
Details of the International HIV Dementia Scale Score Calculated Based on Neurological Parameters
The polymorphism in the four host genetic factors was explored to understand its association with the immunological factors and the score of neurocognitive impairment. Additionally, the nef gene amplicons were analyzed for the genetic variability from individuals with and without HAND. The analysis was directed to understand their genotype, genetic heterogeneity, and association with different HLA motifs responsible for modulating several functional aspects. HIV-1 subtype was determined using the HIV-1 blast tool from HIV Database, and subtype C was the most predominant subtype noted for all the samples except one showing BC recombination (IHDS-9). The prevalence of this subtype is consistent with the previously published epidemiological studies from India. 24
Polymorphism of CCR5
CCR5 delta 32 heterozygous variants were present in two samples with an IHDS score <9.5 with a low viral load, whereas one CCR5 wild-type sample presented with a high viral load (2,290,000 copies/mL). The samples with IHDS score >9.5 had a wild-type CCR5 allele without leading to neurocognitive impairment and moderate viral load (Fig. 1). The heterozygous allelic variant might be responsible for developing resistance to replicating the virus affecting disease progression. Many other parameters might be responsible for the development of HAND and the increase in viral load in the first group. On the contrary, the samples from the non-HAND group with an IHDS score >9.5 are showing CCR5 Wt/Wt with viral load in thousands depicting the normal progression of the disease.
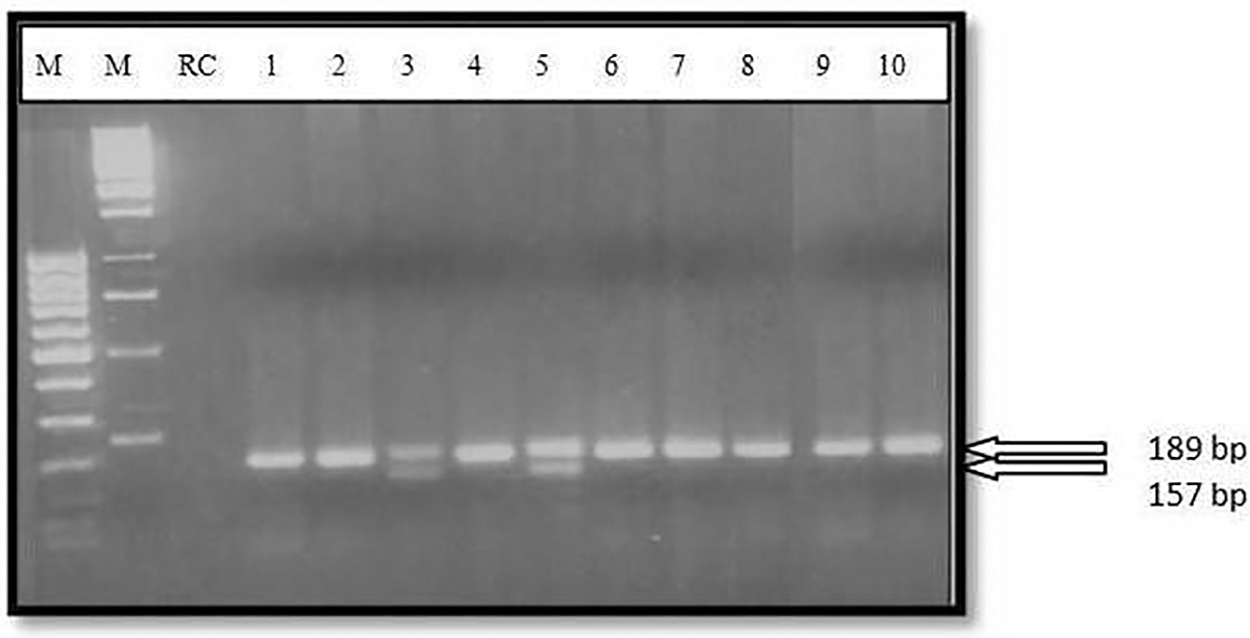
Four percent agarose gel electrophoresis of CCR5 gene amplicons. M1: 100 bp ladder; M2: 1 kb ladder; 1–10: IHDS 1–10 clinical samples. IHDS, International HIV Dementia Scale; RC, reagent control.
Polymorphism of CCR2
Analysis of CCR2 gene polymorphism on polyacrylamide gel electrophoresis did not show the presence of 110 and 18 bp allelic variants, whereas only wild-type allele (128 bp) was seen irrespective of their neurocognitive score (Fig. 2). No significant associations of CCR2 gene polymorphism from both the groups with immunological and virological markers of disease progression status or neurocognitive score were observed.
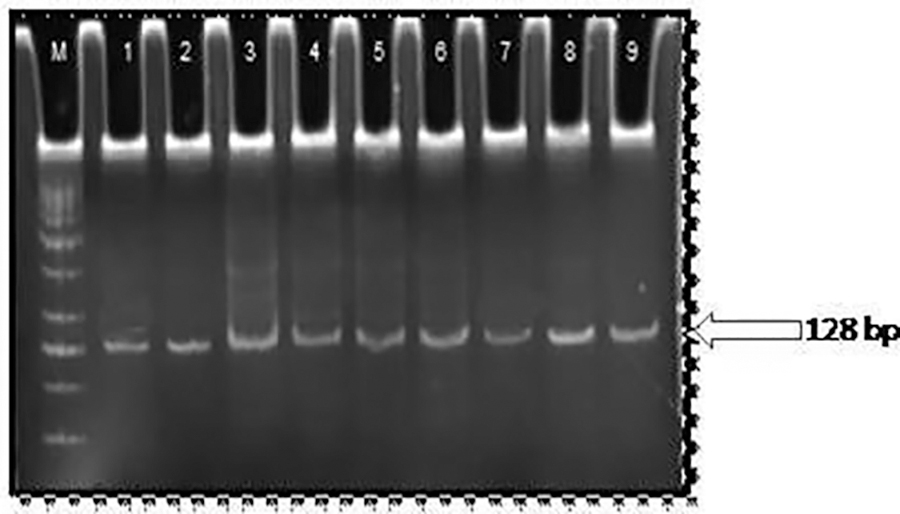
RFLP image of CCR2 gene amplicons. M: 20 bp ladder; 1–9: IHDS 1–9 clinical samples. RFLP, restriction fragment length polymorphism.
Polymorphism of SDF
Analysis of SDF gene polymorphism results indicated the presence of wild type (SDF-1 3′ G/G) with 320 bp amplicon in IHDS-3, IHDS-5, and IHDS-10, indicating the normal progression of the disease irrespective of the neurocognitive score, while IHDS-1, IHDS-2, and IHDS-4 indicated the presence of SDF-1 3′ G/A heterozygous allelic variant from the first group with neurocognitive score <9.5 and showing association with increased viral load (Table 1 and Fig. 3). The presence of a heterozygous allelic variant in the IHDS-2 sample confirmed the involvement of this polymorphism in the development of neurocognitive impairment.
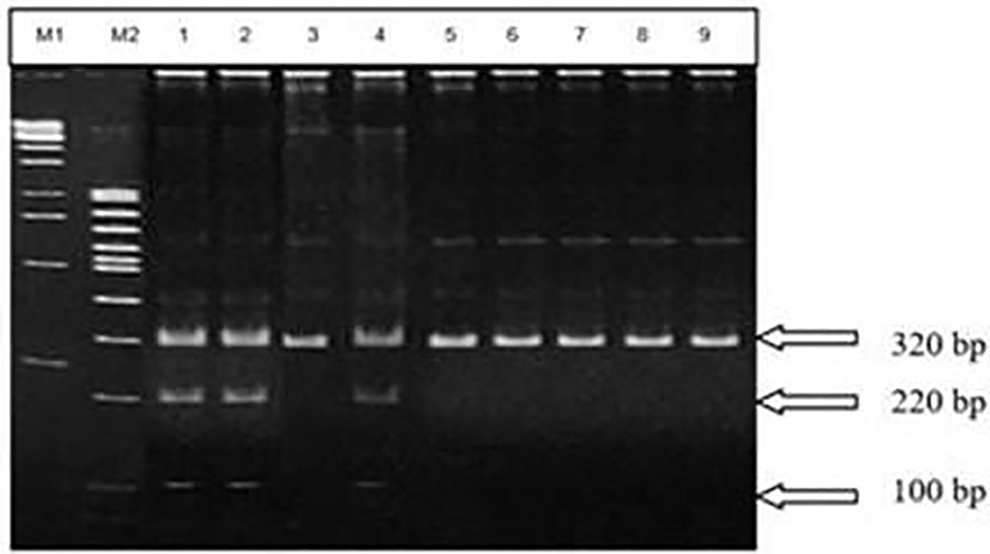
RFLP image of SDF gene amplicons. M1: 1 kb ladder; M2: 100 bp ladder; 1–9: IHDS 1–9 clinical samples. SDF, stromal derived factor.
Polymorphism of MBL
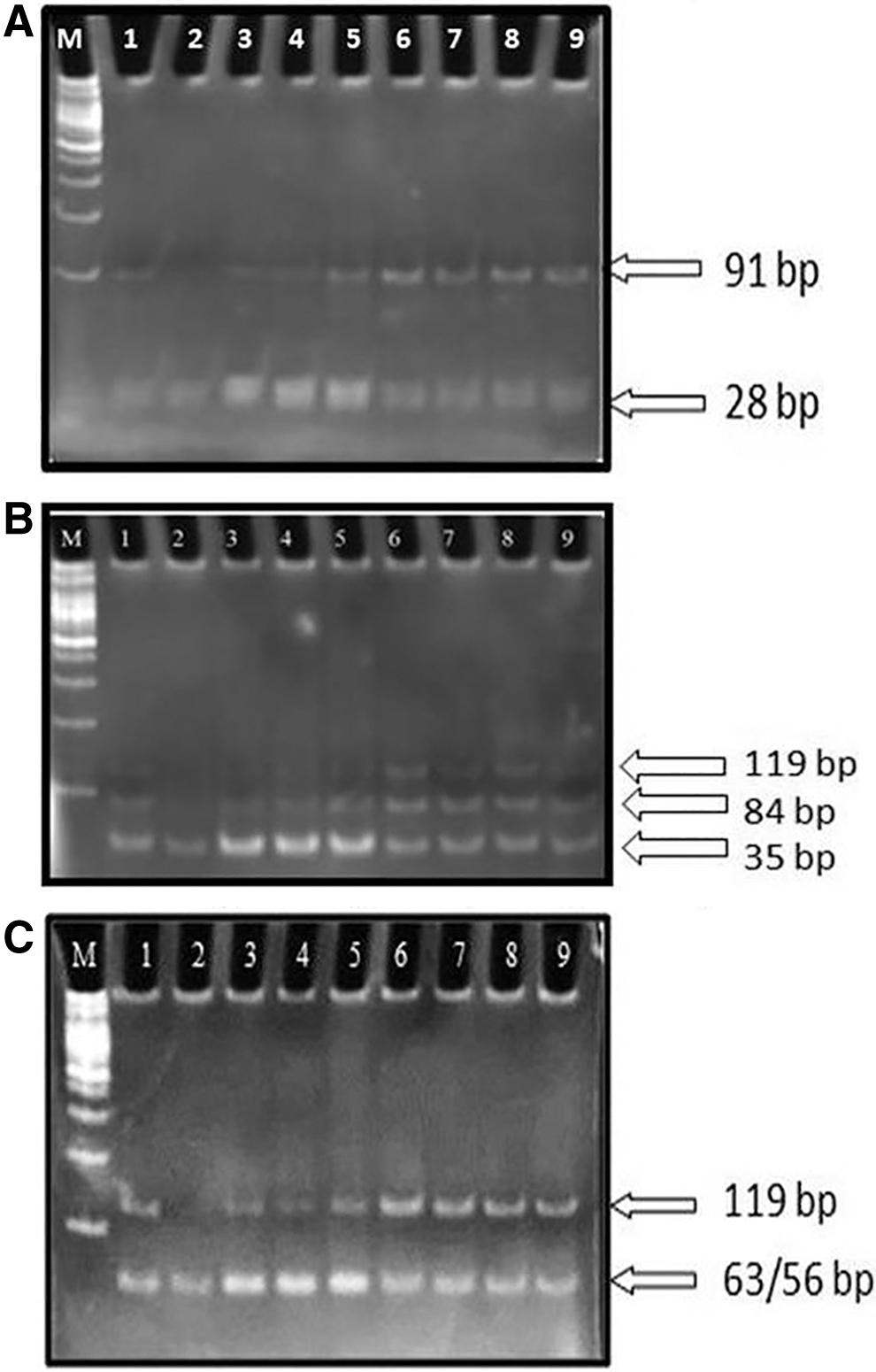
As a result of polymorphism analysis of MBL data depicted in Figure 4A–C that in MBL codons 52, 54, and 57, all samples were showing a variable pattern of polymorphism. In MBL 52 codon-specific amplicon, digestion with HhaI restriction enzyme showed 91 and 28 bp fragments representing homozygous allelic variants in all samples except IHDS-2. In MBL 54 codon-specific amplification, digestion with BanI restriction enzyme showed the 119, 84, and 35 bp fragments representing heterozygous allelic variants in all samples, except IHDS-2, while in MBL 57 codon-specific amplicon, digestion with MBOII restriction enzyme showed the 119, 63, and 56 bp fragments representing heterozygous allelic variants in all samples, except IHDS-2. Due to the limitation of the wells in the polyacrylamide gel electrophoresis (PAGE) gel, only nine samples were considered at a time for electrophoresis, whereas one sample was considered in the independent gel for CCR2, SDF, MBL 52, 54, and 57 codons, and its polymorphism result follows the majority of polymorphism results observed in respective genes (data not shown).
Amplification and genetic analysis of nef gene
Nef gene from clinical samples was amplified by PCR and resulted in an amplicon of ∼620 bp (Fig. 5). The purified nef amplicon was sequenced in 3730XL genetic analyzer, and the generated sequences that were analyzed using SeqScape software and online tools from the HIV database were used for generating the alignment with a consensus sequence of HIV subtype C.

1.2% Agarose gel electrophoresis of HIV-1 nef gene amplicons. M: 1 kb DNA ladder; 1–10 = IHDS 1–10 clinical samples, 11 = negative control.
Amino acid alignment of Nef sequence
The N-myristoylation motif (MGGKWSK), especially G2 of this motif, is an essential region for N-myristoylation and also essential for anchorage to the cell membrane, which is very much conserved in both the groups indicating the essentiality of docking of this amino acid portion to the cell membrane for viral entry. Thus, being a conserved sequence of this motif from both the groups, it neither affects the rate of disease progression nor is responsible for a change in the status of neurocognition. Functional analysis of these findings needs to be performed in future studies.
Furthermore, a cluster formed due to the presence of amino acid arginine at four locations, namely R17, R19, R21, and R22, is associated with the membrane and responsible for the downregulation of CD4, and this is conserved at all four places of the cluster in the HAND group except R21 that is replaced by K21 in IHDS-N1 indicating either the Nef-mediated endocytosis or use of other receptors for viral entry as seen in an increased number of viral copies, while in another group, the replacement of arginine at R17 by K17, R22 by G22, and R22 by Q22 in IHDS-N6, IHDS-N7, and IHDS-N10, respectively, affects the motif required for downregulation of CD4.
Although partial replacement of one glutamate residue from this motif forming KEEE or EKEE motifs indicates brain-specific signature sequences and is considered responsible for weaker MHC-1 downregulation while mutation of EEEEE62-66 to RK(R)KKE62-66 is responsible for reducing the rate of disease progression by reducing the downregulation of MHC-I molecules. 25 However, the current study samples do not show such substitution patterns and hence could not be correlated with the rate of disease progression or reduced MHC-1 downregulation. Subsequently, one of the smallest consensuses tetraproline motif (PxxP) is imperative for refereeing the pathogenic roles of Nef-like enhancement of the rate of replication and potential of infectivity. Precisely, the first and last proline from this motif is crucial for Src homology domain (SH3) binding and is conserved in all our study samples. This particular SH3 binding motif in Nef is known to be required for Nef binding to Hck (Fig. 6). 26
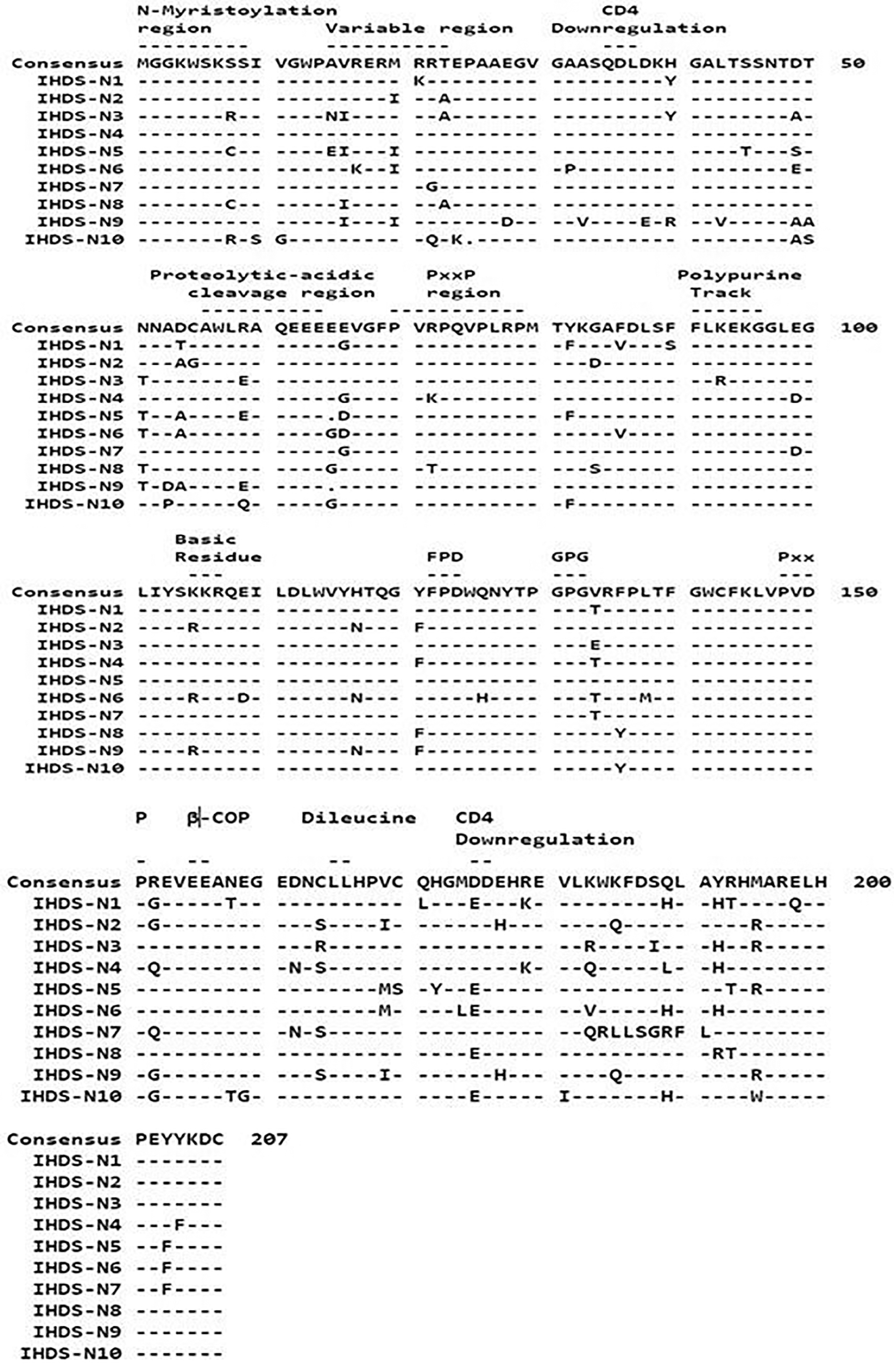
Multiple amino acid sequence alignment of Nef with consensus subtype C sequence. Identification of the study samples is indicated on the left side of the figure. The conserved motifs with their functional significance are shown with the dashed line above the sequence. Dashes are added to indicate the conservation of the amino acids in the alignment. A ruler with a block of 10 amino acid residues is shown in the figure.
Prediction of HLA binding epitopes
Human leukocyte antigens predominantly found in the Indian population and studied by Kumar et al. in 2006 were selected to forecast the same from the consensus of study samples. The presence of specific HLA supertypes from conserved regions of HIV-1 Nef protein could potentially serve as a source of vaccine. Altogether 128 epitopes were predicted for selected HLA alleles, as shown in Figure 7. Fifteen epitopes from A2, A*0201, A*2702, A*2705, B7, and A*0401 were showing a very high-affinity binding score of >100. Additionally, epitopes from each of the Nef sequences from study samples along with the binding score may show variations concerning changed motif sequence due to mutation, insertion, or deletion in that region (data not shown). Most of the motifs are clustered around conserved regions of the sequence.
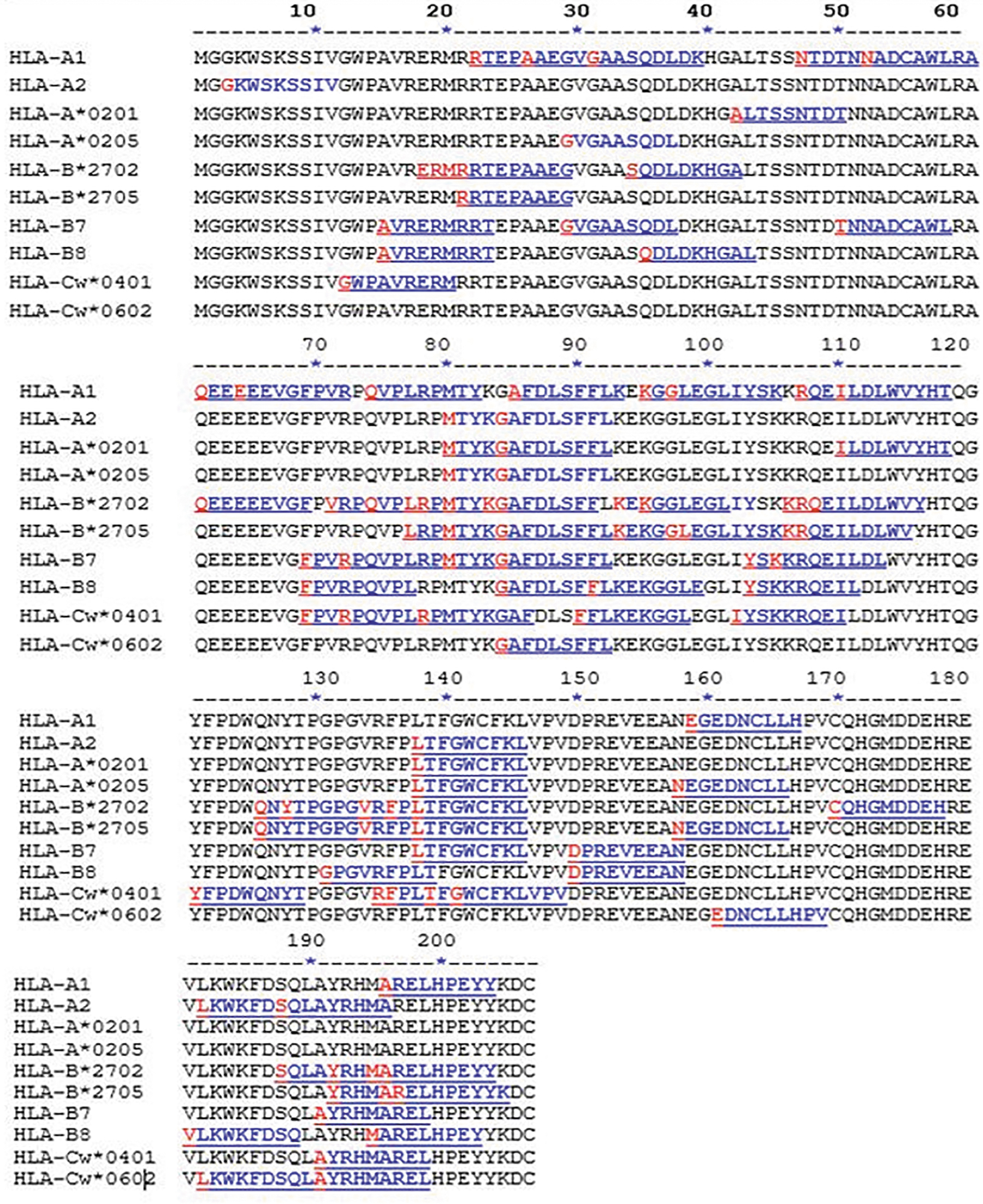
Deduced HLA binding epitopes for the Nef sequence, predicted HLA binding epitopes for consensus Nef sequence of study strains of HIV-1. The 10 most common high-frequency HLA motifs predominate in the Indian population were included for prediction using ProPred-I HLAs Binding Prediction software. HIV, human immunodeficiency virus; HLA, human leukocyte antigen.
It is observed that epitopes LTFGWCFKL (aa 134) and GAFDLSFFL (aa 83) were binding with HLA molecules at 80% and 60%, respectively, among study sample sequences screened for subtype C study sequences, and both these motifs were extremely well conserved in our study samples. There were a few interesting amino acid motifs such as RTEPAAEGV (aa position − 22) that was a binding epitope for HLA-A1 (aa position 21) while it was a non-binding epitope for the HLA-A2 allele. Furthermore, MARELHPEY (aa position − 195) was a binding epitope for HLA-B8 and HLA-cw*0602 (aa position 14), while it was a non-binding epitope for the HLA-B7 allele. Four more such motifs were showing predicted binding and non-binding epitopes simultaneously. Thus, an epitope-based vaccine can be designed considering genetic variations and predicted epitopes within the HLA system.
Discussion
Detecting the contribution of host genetic factors acting either as neurotrophic and/or neurovirulent factors provides us information in understanding the impact of these factors in the neurological system leading to the development of HAND. In the present study, we have observed an association of polymorphism from CCR5, SDF, and MBL except for the CCR2 gene on the progression of HAND. Due to increasing prevalence, it is necessary to study the impact of polymorphisms on the progression of neurocognitive impairment. However, the outcome related to the polymorphism in CCR5, SDF, and MBL2 genes proved that the presence of a heterozygous type of allele is not the only reason responsible for indicating the different rate of development of neurocognitive impairment. There might be the presence of several other factors enhancing their cumulative effect on neurocognitive impairment. These findings need to be explored on a large scale to understand the dropping, leading, or co-dominant type of impact of this polymorphism.
Several population-based studies carried out globally have shown that genetic variants CCR5-Δ32 (deletion of 32-bp), CCR2-V64I (V → I), and SDF1-3′A (G801A) slower the rate of disease progression consequently leading to delayed onset and/or reduced severity of AIDS as well as HAND. 27 In the current study, we have seen two samples with neurocognitive scores <9.5 showing CCR5 heterozygous allelic variants (Fig. 1) and reduced viral load compared with other samples from the same group, whereas viral load in the same range was observed for another group with neurocognitive score >9.5.
There is less prevalence of CCR5 polymorphism in India and completely absent in the non-Caucasian population, while 13%–20% of the heterozygous form (CCR5Wt/CCR5Δ32) was detected in a normal unrelated Caucasian population of European heritage. 28 Apart from the CCR5-Δ32 allele, 12 different point mutations are reported from the CCR5 coding sequence, and hence, it cannot be a surrogate marker for disease progression. 29 Polymorphisms in the CXCR4 and CCR5 coding sequences other than CCR5-Δ32 do not appear to play a dominant mechanistic role in nonprogression among HIV-infected individuals. 30 It has been shown that the CCR5Δ32 allele was observed only in three populations (Yamani, Pathan, and Kamma), all in low frequencies (1%–3%). 31
The presence of a wild-type allele for CCR2 from all samples of the current study did not show any impact on the neurocognitive impairment. However, there might be an association of the heterozygous type of polymorphism with other genes responsible for neurocognitive impairment from the study samples. There is an absence of CCR2-V64I polymorphism in study samples (Fig. 2), and hence, we could not assess its association with disease progression, plasma viral load, as well as CD4 count indicating its absence of association with viral neuropathogenesis. 32 The only reported ligand of this CCR2 is MCP-1, and disparity in expression levels of MCP-1 probably restricts the role of CCR2 in persons with the CCR2-64-I allele.
Furthermore, Lee et al. and Mariani et al. reported that polymorphism in CCR2 did not affect the expression levels of other co-receptors such as CCR5 or CXCR4, and the presence of polymorphic CCR2 does not affect the entry of the R5 or X4 tropic strains of the virus in the cells demonstrating the effect of its polymorphism to be different in both the compartment. 33,34 However, we have neither studied the polymorphism in the MCP1 gene to correlate its association with the development of neurocognitive impairment nor understood the mechanisms involved in the effects of CCR2-V64I polymorphism in the progression of the disease as we could not observe any polymorphism in CCR2 gene. Additionally, these findings could not be confirmed due to the small sample size.
SDF-1 is an important co-receptor for infection of HIV to T cells as well as neurons, microglia, and astrocytes as SDF-1 binds to CXCR4, which is a vital chemokine receptor expressed on these cells. 35 The binding of this co-receptor to CXCR4 prevents the entry of HIV by competing or downregulating the expression of CXCR4, 36 but at the same time, it is responsible for developing neurotoxicity directly. A polymorphism in SDF (G to A) leads to disease progression in HIV-infected adults and is of major concern; however, SDF1-3′ -A/A polymorphism, rs1801157, stimulates the production of SDF and decreases the progression of the disease. 37
In contrast, the presence of homozygous SDF1-3′ -A/A genotype in children indicated a faster rate of disease progression and neurocognitive impairment compared with wild-type SDF1-3′ -G/G genotype. One of the studies, however, reported the upregulated expression of the SDF gene in astrocytes in HIV-positive patients and probably that was the concern for the development of HAND. 38 Thus, homozygous SDF1-3′A/3′A and SDF-1-3′G/G increase the production of SDF and delay the disease progression, while heterozygous polymorphism leads to the progression of the disease.
The current study demonstrated the association of polymorphism with disease progression from the first group with IHDS score <9.5, wherein IHDS-1, IHDS-2, and IHDS-4 indicated the presence of SDF-1 3′ G/A heterozygous allelic variant and high viral load while there was a presence of wild type (SDF-1 3′ G/G) with 320 bp amplicon in IHDS-3, IHDS-5, and IHDS-10 demonstrating the normal progression of the disease irrespective of the neurocognitive score while heterozygous allelic variant in IHDS-2 confirmed its association with neurocognitive impairment with the present high viral copies as well as low IHDS score (Fig. 3).
In concordance with the published literature, this study also reports the association between MBL-2 polymorphisms with viral load leading to the progression of the disease. MBL has the main function in innate immunity by attracting carbohydrate and mannose moiety present on the surface of the pathogens. The polymorphism in the MBL-2 gene affects the synthesis of nonfunctional proteins, thereby increasing the risk of various infections. The three missense mutations present in the codon of MBL at 52, 54, and 57 located in the exon 1 reduce the expression levels of serum MBL and prevent the oligomerization of collagen, 39 thereby the presence of homozygous B, C, and D alleles of MBL (rs1800450, rs1800451, and rs5030737, respectively), indicating larger cognitive deterioration. 15,40
For MBL-2 allele polymorphism, all samples were showing a variable pattern of polymorphism for different codons. In MBL 52 codon, two fragments (91 and 28 bp) represent homozygous (MBL-2 D/D) allelic variants in all the samples, except IHDS-2 (Fig. 4A). In MBL-2, 54 codons showed the presence of 119, 84, and 35 bp fragments representing heterozygous allelic variants (MBL-2 A/B) in all samples, except IHDS-2 (Fig. 4B), while in MBL-2, 57 codon showed the presence of 119, 63, and 56 bp fragments representing heterozygous allelic variants (MBL-2 A/C) in all samples, except IHDS-2 (Fig. 4C).
Thus, variance in the SNPs of MBL genotypes and the absence of MBL-2 A/A homozygous genotype leads to reduced expression of MBL-2 demonstrating the overall trend for a more rapid disease progression in all the HIV-positive individuals. Considering the polymorphism of all the different host genetic factors, it is observed that the IHDS-2 sample is unique in its polymorphic presentation and its association with immunological and virological parameters warranting further in-depth research. Apart from this association, we have observed a marginally reduced count of CD4-positive cells in the neurocognitive group compared with those without neurocognition. Due to insignificant differences, we could not establish its association. Additionally, we have observed a marginally reduced count of CD4-positive cells in a neurocognitive group compared with those without neurocognition.
Considering the importance of the viral and host genetic factors in contributing to the progression of HAND will help out to explain the multifaceted route of neuropsychological dysfunction in HIV-positive individuals in the development of this neurocognitive disorder. This would help in the improvement of therapeutic strategies, namely pharmacogenetics measures encouraging neuroprotection against HAND. Thus, among different host genetic factors, chemokine receptors play a significant role in the infection, transmission, tropism, and pathogenesis as well as in the control of overall infection in a variety of diseases. They are a potent chemoattractant for a variety of cells involved in host defense. Genetic polymorphism in these host genetic factors will affect the rate of disease progression in HIV-infected individuals leading to HAND and needs further attention. 41
Although genetic polymorphism in various chemokine receptors is associated with disease progression, we could not establish a concrete association between polymorphism data and disease progression due to a limited number of samples in the current study as well as a lack of follow-up samples. The polymorphism data generated on a large scale along with analysis of normal healthy controls will help in the understanding association of polymorphism with the disease status and thereby modulating therapeutic strategies for getting neuroprotection in people living with HAND.
Conclusions
The variations in the viral load might be associated with the polymorphism in the host genetic factors such as CCR5, SDF, and MBL2 codons following disease progression leading to an intricate course of neurocognitive impairment. The genetic analysis of the HIV nef gene sequences indicated the mutations from various motifs distributed throughout the full-length nef sequences of both the groups with an association of distinct motifs responsible for disease progression. Due to immunological impairment, however, such polymorphism in the host and viral genetic components might be directly or indirectly associated with an increased or decreased risk of HAND.
Footnotes
Acknowledgments
This study is the part of PhD topic performed by the first author and registered (PRN 12049001008) at Symbiosis International University, Pune, India. The samples used in this study were generously provided by Dr. Manisha Ghate. The author acknowledges the support of all those who directly or indirectly were part of this study.
Authors' Contributions
S.J. processed all the samples and performed laboratory experiments along with the writing of first draft of the article. V.N. conceptualized and guided the experiments and revised the article. Both the authors have approved the final version of the article.
Sequence Data
HIV-1 nef gene sequences studied from IHDS samples are deposited in GenBank and representing the following accession numbers MT337374 to MT337383.
Data Availability Statement
The associated data with the samples are available with institutional repository, while laboratory experimental data are available from V.N.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.