
Abstract
Early antiretroviral therapy (ART) initiation is WHO recommendation to fasten viral suppression and for prevention of further viral transmission sexually. There is no evidence showing the level of adherence to ART after initiation of the universal test and treat (UTT) strategy in Ethiopia, including study area. This study was aimed to determine the level of ART adherence and associated factors among HIV/AIDS patients in context of UTT strategy. A health facility–based study was conducted on 352 people living with HIV who started their ART follow-up after application of UTT strategy in Ethiopia from April 15 to June 5, 2020. Systematic random sampling method was used to select the study participants. Interviewer administered questionnaire was used to collect data and the collected data were entered directly in to SPSS version 21 and analyzed. Both bivariate and multivariate logistic regression analyses were carried out. Strength and direction of association was determined by using adjusted odds ratio (AOR) with 95% confidence interval. The total 352 participants included the study. The overall level of adherence was 290 (82.4%). Commonly used ART regimen was TDF +3TC+EFV, 201 (57.1%). In bivariate analysis, type of health institutions, crude odds ratio (COR) = 2.934 (1.388–6.200), age level of 18–27 years, COR = 0.357 (0.133–0.959), current viral load of 3log scale, COR = 0.357 (0.133–0.959), and change of ART medication, COR = 8.088 (1.973–33.165) were associated with medication adherence. Health institution type AOR = 2.615 (1.147–5.9600) and change of ART medication, AOR = 7.267 (1.683–31.384) were independent predictors of ART adherence. Low level of ART adherence was detected in this study. It was below the recommended good adherence standard and 90-90-90 target strategy. Therefore, patients should get adequate and comprehensive ART adherence counseling before initiation of ART treatment and during the follow-up time.
Introduction
Globally, 39
The early initiation of eligible patients on ART through early diagnosis and linkage of HIV-positive patients to chronic care is one of the key to reach UNAIDS HIV elimination targets. 6 Although the number of people accessing ART is increasing through the year, effectiveness of the therapy highly depends on strict adherence to ART. 5 Universal voluntary counseling and testing followed by immediate initiation of ART for all those diagnosed HIV positive (universal test and treat, UTT) has the potential to reduce HIV incidence dramatically but would be very challenging and costly to deliver in the short term. 7 According to the WHO, rapid initiation of ART is defined as commencement of highly active antiretroviral therapy (HAART) within 7 days of HIV diagnosis. It strongly recommends ART initiation on the same day as HIV diagnosis, after ensuring the person's willingness and readiness to start ART immediately, unless there are clinical reasons to delay treatment. 8
In Ethiopia, an estimated 670,906 people living with HIV (PLHIV) were registered in 2016, of which 385,642 were women and 285,263 men. 9 Prevalence of viral load suppression among HIV-positive adults aged 15–64 years in urban Ethiopia is 70.1%, which is close to the three 90s of UNAIDS target, but it varies by age, gender, and geographic region. 10 Considering the dramatic effect of ART on viral load suppression, it is reasonable to consider using treatment in individuals infected with HIV as a means of preventing HIV transmission. Effective ART in preventing infected individuals from their pathophysiological progression to AIDS has been established to date and continuously improved over time with assumption of high adherence level maintenance so that the UTT policy helps to curb the HIV epidemic. 11
Different investigators identified varying levels of adherence and several associated barriers of optimal adherence of ART at hospital level 12 –15 but at the health center level, there is scarcity of data particularly after adoption of UTT strategy. Other studies conducted across Africa reported varying levels adherence to ART among HIV patients. 16 So, this study was aimed to assess the level of ART adherence and the associated factors among PLHIV in context of early initiation of test and treat strategy in Wolaita Sodo, Southern Ethiopia.
Materials and Methods
Study area and period
The study was conducted in Wolaita Sodo Town health institutions, Wolaita Sodo, Ethiopia. Wolaita Sodo Town is located ∼392 km south from Addis Ababa. There are three health centers, one public, one private referral, and general hospital in Wolaita Sodo. They provide different health care services including ART treatment and follow-up. From these health institutions one health center and one public hospital provide ART service.
Study design
A cross-sectional study was conducted in ART clinics of University referral hospital and health center from April 15 to June 5, 2020. A total of 2,490 individuals were on ART in ART clinics of hospital and health center; patients who started the ART follow-up after adoption UTT was included.
Source and study population
All PLHIV and those who attended ART clinics of the hospital and health center were taken as the source population, and all participants who enrolled after the initiation of UTT strategy and attended ART clinics during the study period were considered as the study population. Patients aged older than or equal to 18 years and who took ART for at least 3 months since August 2016 were included in this study.
Inclusion and exclusion criteria
Inclusion criteria were PLHIV who had followed ART for at least 6 months in selected health facilities, willing to give their informed consent, and self-disclose information about the exact nature of their adherence to the dosage schedule of the ART that had been prescribed for them. Adults older than or equal to 18 years of age were included. PLHIV who suffered from any severe mental illness, poor general health, and all HIV-positive patients who had taken the ART medications for <6 months at the time of the study were excluded.
Sample size and sampling technique
The sample size of the study was calculated using a single population proportion formula with the assumptions of 95% confidence level, marginal error (d) of 0.05, and adherence level (p) of 50%. Through application of the abovementioned assumption, the initial sample was 384. As the total population was <10,000, correction formula was used. After adding 10% nonresponse rate, the final sample size calculated was 367. One health center and one hospital in the town where health institutions provided ART service were selected for the study.
Then to select samples from each health facility, samples were proportionally allocated to health center and hospital, which was estimated based on their average patient flow for outpatient services in the months before data collection. From the total of 2,490 PLHIV, 1,867 were found in Wolaita Sodo University Hospital and the remaining 623 were following ART treatment in Sodo health center. After the sample was proportionally distributed to both health facilities, a systematic random sampling technique was used to select samples from each health facility using k values. k Values were separately estimated for each health institution, Wolaita Sodo University Hospital (k = 1,867/275 = 7) and Sodo Health Center (k = 623/92 = 7). Finally, participants were selected by systematic sampling technique using a sampling frame that was developed from the registration book of the patients after the first participant was selected by lottery method.
Study variables
Dependent variable
Adherence to ART.
Independence variables
Sociodemographic, socioeconomic, medication-related variables and patient-related variables.
Data collection technique
Sociodemographic, medication, and health care–related characteristics of study participants were collected by face-to-face interview with a structured and pretested questionnaire. Adherence level was measured by counting the number of pills that remained in the patients' bottles when he/she came for follow-up. Then, based on WHO guidelines, patients who reported an intake of ≥95% of the prescribed medication were considered adherent, and those with a reported intake of <95% were considered nonadherent. 17 Recent medical records were also reviewed to assess CD4 cell count, viral load, WHO clinical staging, current ART regimen, duration of infection, duration of treatment, and presence of TB confection. Data were collected by trained nurses with supportive supervision of the principal investigator.
Data process and analysis
Completeness of the data was checked every day and entered using SPSS version 21. To examine the influence of different variables on medication adherence and controlling for potential confounders, both binary and multiple logistic analyses were performed. Independent variables with p < .25 in the bivariate logistic regression analysis were entered into multivariable logistic regression analysis to control for confounding effect. Value of p < .05 was considered significant in the final model.
Ethical considerations
Ethical clearance was obtained from Wolaita Sodo University Ethical Review Board. A letter of cooperation was written to Wolaita Sodo University referral hospital and Sodo Town Health Center (STHC) and permission was obtained from the hospital and health center administration. Written informed consent was obtained from each study participant after explaining the purpose and procedures of the study. The study participant results were kept confidential and they were assured that only aggregate data will be reported. All necessary results of the participant were communicated with the physician for proper management.
Results
Sociodemographic characteristics
From the total sample size calculated, 352 were included in the study, providing 96% response rate. Most of study participants were selected from Wolaita Sodo University Teaching Referral Hospital (WSUTRH), 245 (69.6%), as it serves large number of PLHIV. From a total of 352 participants, 216 (61.4%) were men and majority 155 (44.0%) were in the age group of 28–37 years. Most participants were married, 47.7%. Concerning educational level, 165 (46.9%) of the study participants completed 1–8 education level and large proportion of study participants were married 168 (47.7%). Regarding monthly income, 109 (31.0%) had a monthly income of 0–500 Ethiopian birr, so majority were dependent (Table 1).
Distribution of Study Participants by Sociodemographic Characteristics Among HIV/AIDS Patients at Wolaita Sodo, Ethiopia, 2020
ETB, Ethiopian Birr; STHC, Sodo Town Health Center; WSUTRH, Wolaita Sodo University Teaching Referral Hospital.
Medication and patient-related characteristics
From the total study participants, 192 (54.5%) had <1 year since HIV-positive result and initiation of therapy. In this study, the duration of median time HIV-positive test result to ART initiation was 5 [interquartile range: 1–10] days. This indicates that the UTT strategy of linking all HIV-positive individuals to ART regardless of their CD4 cell count and clinical stage was applied at the study setting. Majority (n = 293; 83.2%) were having CD4 level of >200 mL/mm3 and for 276 (78.4%) participants the current viral load was <1.7 log scale. The first-line regimen given for PLHIV in Ethiopia was TDF +3TC+EFV and AZT +3TC+EFV, AZT +3TC+NVP, and TDF +3TC+NVP were used as alternative ART regimens.
The second-line regimen was TDF +3TC+LPV/r or ATV/r and AZT +3TC+LPV/r or ATV/r. It is also true in this study that most common combination of ART drug regimen used was TDF-3TC-EFV, 201 (57.1%). The number of participants who started or changed to second-line regimen TDF-3TC-LPV/r or ATV/r was 11 (3.1%) and the main reason for ART change was resistance to previous regimen (Table 2). From the total study participants, majority (n = 161; 45.7%) were in the WHO II clinical stage and TB-HIV coinfection was detected among 26 (7.4%).
Medication and Patient-Related Characteristics Among People Living with HIV in Wolaita Sodo Town, Ethiopia 2020
ART, antiretroviral therapy; VL, viral load.
The level of ART adherence and reasons for poor adherence
This study showed that the level of adherence to ART was 290 (82.4%). The level of adherence was more likely in Wolaita STHC to WSUTRH (90.8% vs. 78.6%) (Table 3).
Bivariate and Multivariable Logistic Regression Model of Sociodemographic Characteristics with Adherence to Antiretroviral Therapy in Wolaita Sodo, Ethiopia
Significant in bivariate regression.
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; ND, not done.
About 48.4% participants with poor adherence to medication were mainly owing to simply forgetting medication followed by toxicity of the drug, 25.8% (Fig. 1).
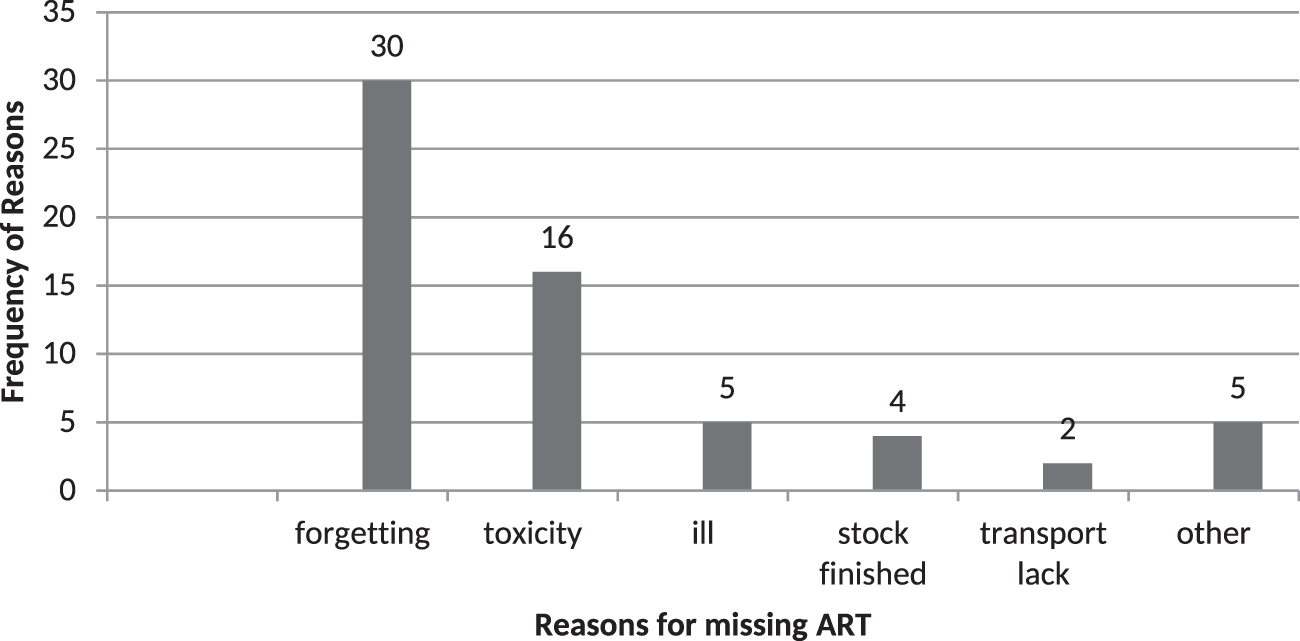
Reasons for poor adherence to ART medication among PLHIV in Wolaita Sodo Town, Ethiopia, 2020. ART, antiretroviral therapy; PLHIV, people living with HIV.
Factors associated with ART adherence
In bivariate analysis, type of health institutions, crude odds ratio (COR) = 2.934 (1.388–6.200); current viral load level of <3 log scale, COR = 0.357 (0.133–0.959); age group of 18–27 years, COR = 0357 (0.133–0.959); and change of ART medication, COR = 8.088 (1.973–33.165) were associated with medication adherence. The likelihood of poor adherence was 7.267 times higher among participants who changed ART medication than those who had not changed ART medication, adjusted odds ratio (AOR) 7.267 (1.683–31.384) (Table 4).
Bivariate and Multivariable Logistic Regression Model of Clinical Characteristics with Adherence to Antiretroviral Therapy in Wolaita Sodo, Ethiopia
Significant in bivariate regression.
Significant in multivariate regression.
NA, not applicable.
Discussion
This study assessed the level of adherence and associated factors among PLHIV in the context of early initiation of ART in southern Ethiopia. The overall level of adherence to medication in this study was 82.4%. This finding was consistent with previous studies conducted in Addis Ababa (79.1%) 18 Eastern Ethiopia (85%), 19 Gondar, Northwest Ethiopia (88.2%), 14 and south Ethiopia (87%). 20 However, the extent of adherence of this study was higher than previous studies carried out in Jimma, Ethiopia (63.9%), 21 North-eastern Ethiopia (71.8%), 22 southern Ethiopia (68%), 23 Oromia (73.1%), 24 southwest Ethiopia (72.4%), 25 and Mangalore (63.7%). 26 On the contrary, our study showed lower level of adherence than previous studies conducted in Debrebirhan, Ethiopia, 95.5%, 27 the level recommended by WHO. 17 This study was comparable with other studies carried out in South Africa (82.9%) 28 and Botswana (86%). 29 However, lower adherence to ART was detected in other African countries, Tanzania (70%), 30 Gauteng Province, South Africa (77%), and India (74.3%). 31
The variation of adherence level to the ART medication could be owing to difference in health care provision system, factors related to patients, socioeconomic factors, medication, and type of study participants included. 32 In this study, level of adherence was more likely in health center than hospital and this might be owing to small number of ART followers at health center than the hospital, which may lead to sufficient counseling and treatment of patients and showed statistically significant association (p = .022). The level of adherence was higher in women. This finding was supported by other studies elsewhere, Ethiopia. 21,24,33 However, this contradicts other studies conducted in Arbamich, south Ethiopia, which showed high adherence level among men, 51.5%, than women, 48.5%. 34 In this study, the combination ART regimen showed association with level of adherence (p < .05).
This study indicated adherence was high among study participants with recent CD4 count >200 mm3/mL. Low viral load (<1.7 log) was detected among most study participants and showed significant association (p < .05) with level of adherence in bivariate analysis. The participants with high viral load (>3 log) was 72.4% lower adherent to ART medication than participants with low viral load this study.
Conclusion
Compared with WHO standard of ART, this study revealed low adherence to ART medication although they adopted UTT strategy. Health institution type, combination of ART regimen, and history of ART change were factors significantly associated with ART adherence. Only application of UTT strategy may lead to achievement of 90-90-90 target program unless strict counseling and health education is provided to improve drug adherence with more emphasis on hospital following participants, medication changed patients, and AZT-3TC-EFV regimen takers.
Footnotes
Acknowledgments
The authors acknowledge study participants who were volunteers to give all relevant information for the study. The authors thank Wolaita Sodo University Teaching Referral Hospital and Sodo Town Health Center staff members for their support during data collection.
Authors' Contributions
A.H.: conceptualization, study designing, data collection, entry, and cleaning and manuscript writing and revision. T.T.: designed the study, data analysis, interpretation, wrote the article and revised it critically for important intellectual content. S.K.: designed the study, data analysis, interpretation, wrote the article and revised it critically for important intellectual content. All authors read and approved the final version of the article.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was financially supported by Wolaita Sodo University and confirmed by grant number of CMHS/08/2019.