
Abstract
Recent studies suggest that the introduction of antiretroviral agents such as integrase strand transfer inhibitors (INSTI) may lead to weight gain in people living with HIV (PLHIV). In this retrospective observational study, we report the weight changes observed in virologically suppressed HIV patients after 12 months of switching to bictegravir/emtricitabine/tenofovir alafenamide (BIC/F/TAF) due to a national change in public policy in Mexico. Patients on prior regimens based on TDF/FTC or ABC/3TC plus non-nucleoside retrotranscriptase inhibitor, INSTI, or protease inhibitor were included. In the 399 patients analyzed, a significant weight increase was found, as well as an increase in body mass index (BMI), total cholesterol, low-density lipoprotein cholesterol (LDL-C), glucose, creatinine, and CD4+ cells after 12 months of switching treatment (all p ≤ .001). Mean weight gain was 1.63 kg [confidence interval (95% CI): 1.14–2.11], whereas the average percentage of weight gained was 2.5% (95% CI: 1.83–3.17). After considering the confounding effect of baseline weight status, the change in weight and BMI did not present significant differences between any of the prior treatment schemes. In conclusion, PLHIV switching to BIC/F/TAF therapy experienced weight gain after the first year of switching treatment. Although this weight gain could be due to the switch in treatment regimen, it cannot be excluded that it was caused by other factors since no comparable control group could be used for comparison.
Introduction
According to the World Health Organization, 39% of the worldwide adult population are overweight, and 13% are obese. These conditions are associated with other diseases, including type 2 diabetes, cardiovascular disease, and most types of cancer. 1,2 In Mexico, 72.1 and 76% of adult men and women, respectively, have overweight or obesity, which highlights the importance of these diseases among the Mexican population. 3
The prevalence and incidence of overweight and obesity in people living with HIV (PLHIV) has increased over the past two decades, likely a reflection of trends in the world. 4 While the success of antiretroviral therapy (ART) in reducing associated mortality and other comorbidities in PLHIV has been observed, 5 weight gain after initiation of ART could increase the risk of metabolic and cardiovascular diseases, which are now considered the leading cause of death in PLHIV on ART. 6
The introduction of new antiretroviral drugs has brought an improvement in the safety profile, adherence, and efficacy of HIV treatment. Thus, regimens based on integrase strand transfer inhibitors (INSTI) are currently the most widely used. 7 Recent studies report that INSTI or tenofovir alafenamide (TAF)-containing regimens are associated with greater weight gain than non-nucleoside retrotranscriptase inhibitor (NNRTI)- or protease inhibitor (PI)-based regimens. Among these drugs, dolutegravir (DTG) and bictegravir (BIC) were associated with the most significant increases in body weight. 8,9
The purpose of this study was to determine the changes in weight observed after 12 months of switching to bictegravir/emtricitabine (F)/tenofovir alafenamide in virologically suppressed HIV patients. As a secondary objective, we sought to evaluate if the prior treatment regimen before switching to BIC/F/TAF impacted the magnitude of weight change.
Materials and Methods
Study design
On September 2019, a national public policy in Mexico led to a change in treatment regimen for virologically suppressed PLHIV to BIC/F/TAF (as in treatment-naive patients) as the first-line therapy. 10 This resulted in patients switching to this treatment regimen as of early 2020. To evaluate changes in weight in patients after this change in treatment scheme, we conducted a retrospective observational study between January 1, 2020, and February 28, 2021, at an HIV clinic in a second-level hospital of the social security provider Instituto Mexicano del Seguro Social (IMSS) in Mexico City. This was a single-arm observational study, meaning that no control group was included due to the difficulties of obtaining a comparable and unbiased control group since this public policy affected all patients equally at the national level. The study was approved by the institutional research and ethics committee with approval number R-2021-3404-074.
Participants
Patients ≥18 years of age with prior diagnosis of HIV infection who had been on ART and virologically suppressed (HIV-1 RNA <50 copies/mL) for >6 months, and who have received a switching of treatment regimen to BIC/F/TAF were included. Pregnant women, patients with incomplete medical records, and patients with other previous antiretroviral treatment regimens different than tenofovir disoproxil fumarate (TDF) and emtricitabine (FTC) or abacavir (ABC) and lamivudine (3TC) plus NNRTI, INSTI, or PI were excluded from the study.
Variables
Demographic data including age, sex, and comorbidities, as well as the number of prior antiretroviral regimens, were extracted from medical records. To assess the study endpoint, values for body weight were collected in addition to body mass index (BMI), total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides, glucose, creatinine, and CD4+ cells at the time of switching (baseline measurement) and after 12 months. Changes (Δ) in weight, BMI, and metabolic variables were calculated as the difference between the 12th month of follow-up value with respect to the baseline measurement.
Statistical analysis
Descriptive data are presented as mean with standard deviation. Qualitative variables are presented as frequency and percentage. The paired t-test was used to compare changes in weight and metabolic parameters after 12 months of switching the antiretroviral treatment scheme. These data are presented as mean differences with confidence intervals (95% CIs).
A repeated-measures analysis of variance (RM ANOVA) model was built to determine the potential effect of the change in antiretroviral regimen on follow-up variables after 12 months. These results are shown with the p-value obtained through Wilks' λ statistic. Paired comparisons were performed with the post hoc Bonferroni test. To determine the differences in the changes of these variables according to the prior antiretroviral regimen, a random-effects analysis of covariance model was built considering baseline weight in kilograms as the covariate.
To evaluate the potential effect of prior treatment schemes on weight gain and a ≥ 5% weight gain, a log-binomial regression model was created, adjusting for the variables sex, age, months of duration on prior treatment regimen, and years from HIV diagnosis to treatment switch. The treatment group categories were treated as indicator variables and NNRTI was arbitrarily considered the reference category. These results are presented as risk ratios (RR) and 95% CI.
Statistical significance was defined as a p-value <.05. The statistical software SPSS v.21 for Windows was used for analyses. Figures were created with GraphPad Prism v.9.0.1. The study was approved by the institutional research and ethics committee with approval number R-2021-3404-074.
Results
Out of 523 patients who met the inclusion criteria, 116 were excluded because they did not have complete data in their medical records and 8 more for not having any prior treatment schemes considered exposures in this study. Thus, 399 patients were included for analysis. Baseline characteristics of patients according to exposure groups are shown in Table 1. Most patients (97.2%, n = 388) were men with a mean age of 38.4 (standard deviation: 10.5) years. The most frequent prior antiretroviral regimen before enrollment was based on NNRTI (60.9%, n = 243). Important differences in the duration of prior treatment regimens were observed, with shorter duration observed in the INSTI group [6 months, interquartile range (IQR): 5–9], followed by the NNRTI group (27 months, IQR: 17–50) and the PI groups (36 months, IQR:15–67).
Baseline Characteristics of the Study Sample According to Previous Treatment Regimen
A regimen may include changes to the same or different classes of antiretrovirals.
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; INSTI, integrase strand transfer inhibitors; LDL-C, low-density lipoprotein cholesterol; NNRTI, non-nucleoside retrotranscriptase inhibitors; PI, protease inhibitors.
Patients in the PI group had the longest median time from HIV diagnosis to switch in the treatment regimen, 6 years (IQR: 4–13). Baseline weight and BMI were similar across all study groups, whereas only total cholesterol was higher in the NNRTI group. The distribution into BMI categories was constant across the study groups, with a greater representation of the normal weight category (BMI: 18–24.9).
The results of the analysis of weight change, BMI, and laboratory parameters are shown in Table 2. There was a significant increase in weight, BMI, total cholesterol, LDL-C, glucose, creatinine, and CD4+ cells count after 12 months of switching to the ART (all p ≤ .001). The mean weight gain was 1.63 kg (95% CI: 1.14–2.11), whereas the average percentage of weight gained was 2.51% (95% CI: 1.83–3.17). Changes in BMI categories after 12 months were observed, with patients at low or normal weight shifting toward an upper category (p < .0001). Nonetheless, the BMI of patients with overweight and obesity tended to decrease (p < .0001). No substantial changes in the use of statin and fibrate therapy 12 months after the switch in ART were observed.
Changes in Variables After 12 Months of Treatment Regimen Switch
Data are presented as mean and standard deviation. Comparison made by paired samples t-test.
Figure 1shows the comparisons of weight (Fig. 1A) and BMI (Fig. 1B), both of which increased similarly in the three groups of previous treatment regimen after 12 months of follow-up. Although the combined effect of time and prior treatment regimen was not statistically significant in the RM-ANOVA model for weight [F(1, 396) = 1.53, p = .21], there was a significant effect for time alone [F(1, 396) = 26.482, p < .001], and the post hoc analysis showed that only the weight in the NNRTI group (77.2 ± 0.88) was greater than the INSTI group (72.5 ± 1.42) at 12 months (p < .01) (Fig. 1A).
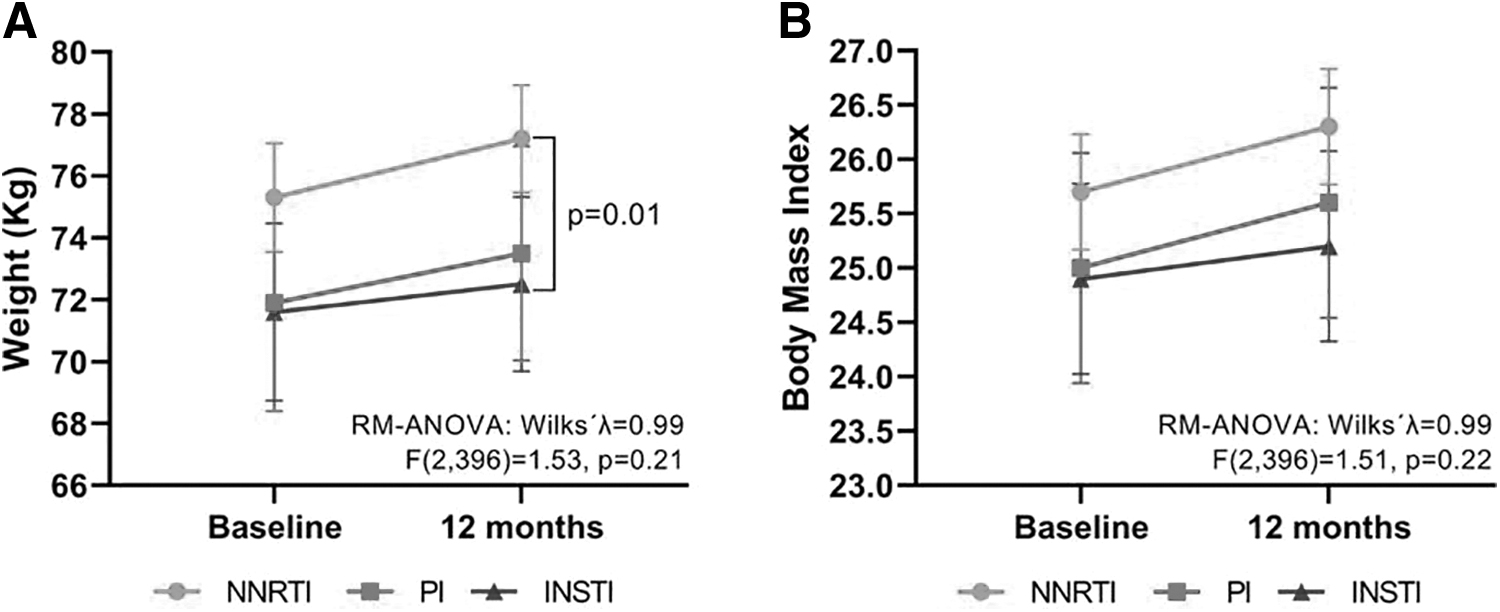
Comparison of weight and BMI at baseline and at 12 months according to the previous treatment regimen. Data are presented as mean and 95% confidence interval. Comparisons were made by RM-ANOVA with pairwise comparisons by the Bonferroni post hoc test. BMI, body mass index; INSTI, integrase strand transfer inhibitors; NNRTI, non-nucleoside retrotranscriptase inhibitors; PI, protease inhibitors; RM-ANOVA, repeated measures-analysis of variance.
There were no differences for the combined effect of time and prior treatment scheme for BMI (Fig. 1B), but there was also a significant effect for time alone [F(1, 396) = 27.599, p < .001]. Supplementary Table S1 shows the change in metabolic parameters at the time of treatment switch and after 12 months of follow-up. Only the combination of time and treatment group had a significant effect on creatinine (increase).
After the elimination of the confounding effect of baseline weight, the change in weight and BMI was not significantly different between any of the prior treatment groups. Likewise, the changes in metabolic parameters were similar between groups, only creatinine levels showed a significantly greater increase in the NNRTI group compared with the INSTI group (Table 3).
Comparison of Changes in Weight, Body Mass Index, and Metabolic Parameters After 12 Months of Treatment Switch, According to the Previous Treatment Regimen
Data are presented as mean ± standard error. Comparison made by random-effects ANCOVA model considering the baseline weight as a covariable, with pairwise comparisons by Tukey's post hoc test.
p < .05 in comparison with the NNRTI treatment.
ANCOVA, analysis of covariance.
Basic descriptive data of subjects who had previous TDF/FTC or ABC/3TC regimens are shown in Supplementary Table S2. In Supplementary Table S3, comparisons of changes in weight, BMI and metabolic parameters after 12 months following the switch in ART are shown. Similar to what is observed in Table 3, there were no significant differences in weight, BMI, and metabolic parameters according to the two previous treatments.
The results of the binomial regression analysis showed that none of the treatments was associated with a higher risk of weight gain (NNRTI: reference; PI: RR = 0.89, 95% CI = 0.65–1.22, p = .48; INSTI: RR = 0.94, 95% CI = 0.69–1.27, p = .94) after adjusting for sex (RR = 1.93, 95% CI = 0.72–5.20), age (RR = 1.00, 95% CI = 0.98–1.01), duration (months) of prior treatment (RR = 1.00, 95% CI = 0.99–1.01), and time (years) from HIV diagnosis to treatment switch (RR = 1.02, 95% CI = 1.00–1.05).
None of the prior treatment groups conferred a statistically significant higher risk of experiencing a weight gain greater than 5% after 1 year (NNRTI: reference; PI: RR = 0.65, 95% CI = 0.42–1.00, p = .05; INSTI: RR = 0.95, 95% CI = 0.61–1.48, p = .95), which was adjusted for sex (RR = 0.67, 95% CI = 0.27–1.68), age (RR = 0.98, 95% CI = 0.96–0.99), duration (months) of prior treatment (RR = 0.99, 95% CI = 0.98–0.99), and time (years) from HIV diagnosis to treatment switch (RR = 1.00, 95% CI = 0.97–1.04).
Discussion
Results in our retrospective cohort study show that switching to a bictegravir/emtricitabine/tenofovir alafenamide-based regimen correlates with weight gain after 12 months of treatment in HIV-infected and virologically suppressed patients. We found a mean weight gain of 1.63 kg, and a mean percentage weight gain of 2.51%. Whether these changes were caused by the new treatment cannot be concluded from our study since a control group was not used. As a secondary objective, we sought to evaluate if the prior treatment scheme before switching to BIC/F/TAF impacted the magnitude of weight change. Our findings do not support that the prior treatment scheme significantly affects the magnitude of weight change after 12 months.
The weight change observed in our sample was less than that observed in the GS-US-380–1489 and GS-US-380–1490 trials. 11,12 The first trial compared BIC/F/TAF against DTG/ABC/3TC and the second, BIC/F/TAF versus DTG/F/TAF. The greatest change in weight occurred in the first year with an adjusted mean weight of 3 kg in both studies combined, followed by annual changes of +0.5 to +0.7 kg/year until week 192. 13 These numbers are higher than those observed in our study. However, it is important to highlight that trials 1489 and 1490 were conducted in patients naive to antiretroviral treatment, and in whom weight gain is expected as a return to health, whereas our study involved virologically suppressed HIV-infected patients who switched ART therapy due to a change in public policy.
Our results are similar to the TANGO study, which evaluated a switch in treatment regimen. This study was conducted in virologically suppressed HIV patients, in which DTG/3TC was compared versus continuing ART for three or four TAF-based drugs. The adjusted mean weight gain from baseline to week 48 was 0.8 kg in both groups. Follow-up at week 144 reported a mean change of 2.2 and 1.7 kg for the DTG/3TC and TAF-based groups, respectively. 14
The 4030 trial, a study of virologically suppressed HIV patients for ≥6 months on ART with DTG plus F/TDF or F/TAF, reported a median weight change from baseline to week 48 of +1.3 kg in the BIC/F/TAF group versus +1.1 kg in the DTG+F/TAF group (p = .46), meaning that there were no significant differences in weight change by the second-generation INSTI groups. Weight change differed by baseline nucleoside reverse transcriptase inhibitor (NRTI) [+2.2 kg (F/TDF) and +0.6 kg (F/TAF), p < .001], with no difference between BIC/F/TAF and DTG+F/TAF. 15 This weight gain according to baseline NTRI was also observed in the OPERA cohort, which examined weight changes in PLHIV who switched from TDF to TAF while maintaining other components of the ART regimen. Switching to TAF was associated with early (first 9 months after switch) and pronounced weight gain (1.80 to 4.47 kg/year). 16
We were not able to make this last comparison in our sample since we did not include a control group that had continued treatment with TDF. However, based on the findings in the OPERA cohort, it is reasonable to think that the weight gain we observed could be attributable to TAF, being greater with INSTI as with BIC.
Adding to the prior point, the Swiss HIV Cohort Study analyzed changes in BMI before the introduction of TAF or INSTI. The BMI increased by 0.31 kg/m2 per year through years 1 to 4, while we observed an increase of 0.57 kg/m2 in our sample, which also supports the notion that the weight gain observed is due to antiretroviral treatment. 17
Noteworthy, patients' weight gain in our study occurred in all groups, regardless of prior treatment scheme. This suggests that changing to BIC/F/TAF may lead to weight gain independently of the previous treatment regimen. Trials 4030 and 4449 showed no significant changes in weight when switching from one INSTI to another INSTI. 15,18
Regarding the BMI, 31.3% of our sample had overweight at baseline, 50% had grade 1 obesity, and 9% had grade 2 obesity. This trend has been evident in the last two decades, coinciding with a previous comparative cohort study done with a North American sample of patients with HIV obtained through the NA-ACCORD and NHANES databases. 19 A limitation in our cohort study was not performing bioimpedance analyses, which could affect the classification of patients as overweight or obese according to their percentage and distribution of body fat, considering the theories of lipohypertrophy related to the effect of INSTIs on adipocytes. 20,21
On the contrary, in the biochemical analysis of the lipid profile, elevation of LDL-C and serum total cholesterol was shown in this study. This increase is compatible with what was reported in clinical trials 1489 and 1490 in naive patients. 11,12 However, in study 4030, there was no difference in fasting lipid change. 15
We found significant increases in fasting serum glucose and creatinine. In the TANGO study, 65% of participants in the DTG/3TC group had insulin resistance by week 48, defined as Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) ≥2 (odds ratio: 0.59, 95% CI: 0.40–0.87). 14 Given that INSTI is a widely used group of drugs, it is important to consider evaluating new onset of diabetes in PLHIV with the use of INSTI in prospective studies.
There was a mean increase of 0.13 mg/dL in the serum creatinine values, coinciding with trial 1489 where an increase in the median creatinine of 0.11 mg/dL and a decrease in the glomerular filtration rate at week 48 were observed for both treatment groups (BIC/F/TAF and DTG/ABC/3TC). 11
Metabolic and weight changes that occur in patients switching to second-generation INSTI, BIC, or DTG, is an important question that remains unanswered. According to our sample and other studies, this gain is lower when an antiretroviral treatment switch is performed compared with treatment-naive patients. 15,18 Other studies have reported that weight gain is greater in women starting or switching to TAF or INSTI. 22 –24 However, more prospective data are needed. In Latin America and other regions, there is still a group of patients who could be switched to this treatment regimen, hence the relevance of our findings.
Regarding the potential generalizability of our results, it is important to note that our study only included 4% of women versus 96% men, reflecting an underrepresentation of women, to whom our findings should not be generalized. This underrepresentation cannot be explained by the estimated prevalence of HIV in Mexico, since in 2019 the estimated prevalence of HIV in men was 0.30% (95% CI: 0.25–0.38) and 0.078% (95% CI: 0.062–0.095) in women, which equates to a relationship of ∼4:1. 25 However, these estimates diverge from the number of persons living with HIV according to the national registry data, since by 2022 there were a total 347,794 persons living with HIV in Mexico, of which 284,204 (81.72%) were men and 63,590 (18.28%) were women, 26 which could reflect that women remain largely undiagnosed and thus without access to treatment in Mexico.
Furthermore, our sample consisted only of patients affiliated to the social security provider IMSS, which could potentially not be representative of the general population of people living with HIV without medical insurance in Mexico.
The main limitation of this study is the absence of a control group, which does not allow us to conclude that the new treatment scheme caused the changes in weight gain. We were not able to include a comparable control group since change of treatment regimen was due to a change in public policy nationwide affecting all PLHIV equally. One alternative to evaluate this change in public policy with comparable control groups could have been to perform a regression discontinuity analysis (RDA), 27 although this was not in our possibilities for this study. We encourage researchers and policymakers in Mexico to conduct an RDA in a larger scale to evaluate the impact of this change in public policy on weight and other outcomes.
Other limitations of our study include its retrospective nature, which could compromise the validity of outcome assessment, as weight measurements were performed by different people, without certainty of a standardized protocol, and with unknown calibration of devices. In addition, the follow-up period occurred during the COVID-19 pandemic and changes in weight could have been influenced by isolation and changes in individual and social behavior. In addition, eating and physical activity habits were not assessed in this study, which are important factors that could have explained the change in weight, as well as the presence of diabetes (5.5%) and psychiatric disorders (6.0%), which are also associated with weight gain. In addition, our study sample may differ from populations in other regions of the world, something that must be taken into account when interpreting these results.
Conclusions
PLHIV switching to BIC/F/TAF therapy experienced weight gain after the first year of switching treatment. Although this weight gain could be due to the new treatment regimen, it cannot be excluded that it was caused by other factors since this was a single-arm cohort with no comparison group. When comparing weight gain according to prior treatment scheme, we did not observe a significantly different risk of weight gain between having received NNRTI, PI, or INSTI. Future studies that include variables such as body and visceral fat distribution, HOMA-IR index to assess insulin resistance, and cardiovascular risk scales are needed.
Footnotes
Authors' Contributions
E.P.-B., S.P.-C., and M.F.G.-M. made substantial contributions to the conception, design of the study, and to the acquisition of data. J.M.-G. and A.K.-G. substantially contributed to data analysis. M.F.G.-M., J.M.-G., A.K.-G., and A.O.-H. prepared the article. All authors gave approval of the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.