
Abstract
Human immunodeficiency virus type 1 (HIV-1) is characterized by a large degree of genetic variability because of high rates of recombination and mutation, sizable population sizes, and rapid replication. Therefore, this study investigated HIV-1 subtype distribution and the appearance of drug resistance mutations (DRMs) in viruses that are prevalent in Makassar, South Sulawesi, Indonesia. The HIV-1 pol, env, and gag genes were amplified from 63 infected individuals and sequenced for a subtyping analysis. CRF01_AE was identified as the predominant HIV-1 circulating recombinant form (CRF) in Makassar, South Sulawesi, Indonesia. Subtype B and recombinant viruses containing CRF01_AE, CRF02_AG, and/or subtype B gene fragments were also detected. Several major DRMs against non-nucleoside reverse transcriptase inhibitors were found among antiretroviral therapy (ART)-experienced subjects, whereas ART-naive subjects did not possess any transmitted drug resistance. The prevalence of DRMs was very high among ART-experienced subjects; therefore, further surveillance is required in this region.
Human immunodeficiency virus type 1 (HIV-1) infection remains a significant global health issue. HIV-1-infected individuals receive antiretroviral therapy (ART), which is highly effective and recommended for all individuals diagnosed with HIV-1 irrespective of their CD4+ T-lymphocyte count. The significant development of antiretrovirals for ART has transformed HIV-1 from an almost uniformly fatal infectious disease into a manageable chronic disease. First-line ART drug regimens consist of a combination of two groups of reverse transcriptase (RT) inhibitors; nucleoside RT inhibitors (NRTI), such as zidovudine (AZT) and lamivudine (3TC), and non-nucleoside RT inhibitors (NNRTI), including efavirenz (EFV) and nevirapine (NVP), are prescribed in Indonesia. 1
Indonesia is a country with the largest number of HIV-infected cases in Southeast Asia. Based on data reported by the Indonesian Ministry of Health, south Sulawesi was 1 of the 10 provinces with the highest number of HIV-infected cases in 2019. Makassar, Pare-Pare, and Kabupaten Janeponto had the highest prevalence of HIV in South Sulawesi province. 2 Makassar is the capital city of South Sulawesi, the fifth largest metropolitan city after Jakarta, Surabaya, Bandung, and Medan in Indonesia, and has the highest HIV infection rate in South Sulawesi.
As a result of the HIV epidemic and its integral roles as a metropolitan city, HIV-1 epidemiology needs to be investigated in Makassar. Previous studies identified CRF01_AE as the most prevalent HIV-1 circulating recombinant form (CRF) across the majority of Indonesian cities, including Medan (North Sumatra), Kepulauan Riau, Pontianak (West Kalimantan), Manado (North Sulawesi), Jakarta, Surabaya (East Java), Bali, and Maumere (West Nusa Tenggara). 3 The prevalence of subtype B was reported to be high in West Papua and Papua. 4,5 Nevertheless, data on HIV-1 epidemiology in Makassar remain limited.
ART has improved the quality of life of infected individuals and has also decreased mortality and morbidity associated with HIV-1 infection. The emergence of acquired drug resistance (ADR) among ART-experienced subjects and transmitted drug resistance (TDR) among ART-naive subjects are major issues associated with ART. The prevalence of drug resistance mutations (DRMs) among ART-naive HIV-positive pregnant women was estimated to be 2.3%–25%, and was recently found to be 24% in freshly infected juveniles, 6 whereas the prevalence of TDR in Surabaya was <5%. 7 However, data on HIVDR in Makassar remain limited; therefore, surveillance for the emergence of DRMs is needed in the area.
Sixty-three HIV-1-infected individuals were recruited and enrolled in the Voluntary Counseling and Testing program in Makassar Hospital. This study was approved by the institutional ethics committees of Universitas Airlangga (approval number: 25-995/UN3.14/PPd/2013) and the Kobe University Graduate School of Medicine (approval number: 784). Written informed consent was acquired from all study participants before the execution of this study. Inclusion criteria for recruiting participants to this study were adults older than 18 years, HIV infections confirmed by three diagnostic methods, and experienced ART for >1 year or ART naive. Exclusion criteria were individuals younger than 18 years and pediatric patients.
Whole peripheral blood samples from 63 individuals (60 ART-experienced and 3 ART-naive individuals) were collected into ethylenediaminetetraacetic acid-treated vacutainer tubes. Plasma was separated by centrifugation at 800 g for 10 min. Peripheral blood mononuclear cells (PBMCs) were isolated by density gradient centrifugation using Histopaque 1077 (Sigma-Aldrich, St. Louis, MO). Cellular DNA was isolated from PBMCs using the QIAamp DNA blood mini kit (QIAGEN, Hilden, Germany). The HIV-1 pol gene encoding RT (the RT gene) and protease (the PR gene) and the viral env and gag genes were then amplified using the GoTaq Green Master Mix (Promega) and a pair of specific primers corresponding to the target genes.
Primers for amplification and sequencing were the same as those previously described 3 and information is available upon request. Sequencing data collection and alignment were performed using Genetyx software version 10 (Genetyx, Tokyo, Japan). Viral RT, PR, env, and/or gag genes were successfully amplified and sequenced from 48 subjects. The nucleotide sequences collected in this study were registered to the GenBank database with the accession numbers ON244098–ON244133 (PR genes), ON244134–ON244168 (RT genes), ON244206–ON244242 (env genes), and ON244169–ON244205 (gag genes).
HIV-1 subtyping was performed using the recombinant identification program (RIP) available at the HIV sequence database website (
Subtypes A1, A2, B, C, D, and G as well as CRF01_AE and CRF02_AG, as major pandemic subtypes, and CRFs of HIV-1, and three CRF01_AE/subtype B-recombinants, CRF15_01B, CRF33_01B, and CRF34_01B, as recombinants frequently found in Indonesia, were included in the phylogenetic tree analysis. Sequence information on the representative reference strains of subtypes and CRFs was retrieved from the website (
The demographic characteristics of 63 study participants are given in Table 1. Of these, 73.0% were male and 27.0% were females. The median age of all patients was 34.2 years (range between 21 and 47 years). In addition, 36.5% of patients were of Bugis and Makasar ethnicity. Among these individuals, intravenous drug use and heterosexual intercourse were the two main transmission routes, accounting for 34.9% and 30.2% of infections in the study population. Among 63 individuals, 60 had received ART for longer than 1 year, whereas the remaining 3 were ART naive.
Demographic Characteristics of Study Participants
ART, antiretroviral therapy; AZT, zidovudine; EFV, efavirenz; NVP, nevirapine; 3TC, lamivudine; TDF, tenofovir disoproxil fumarate.
Medication history showed that the majority of ART-experienced individuals had been treated with the combination of 3TC, tenofovir, and EFV (49.2%), with an average treatment duration of >3 years.
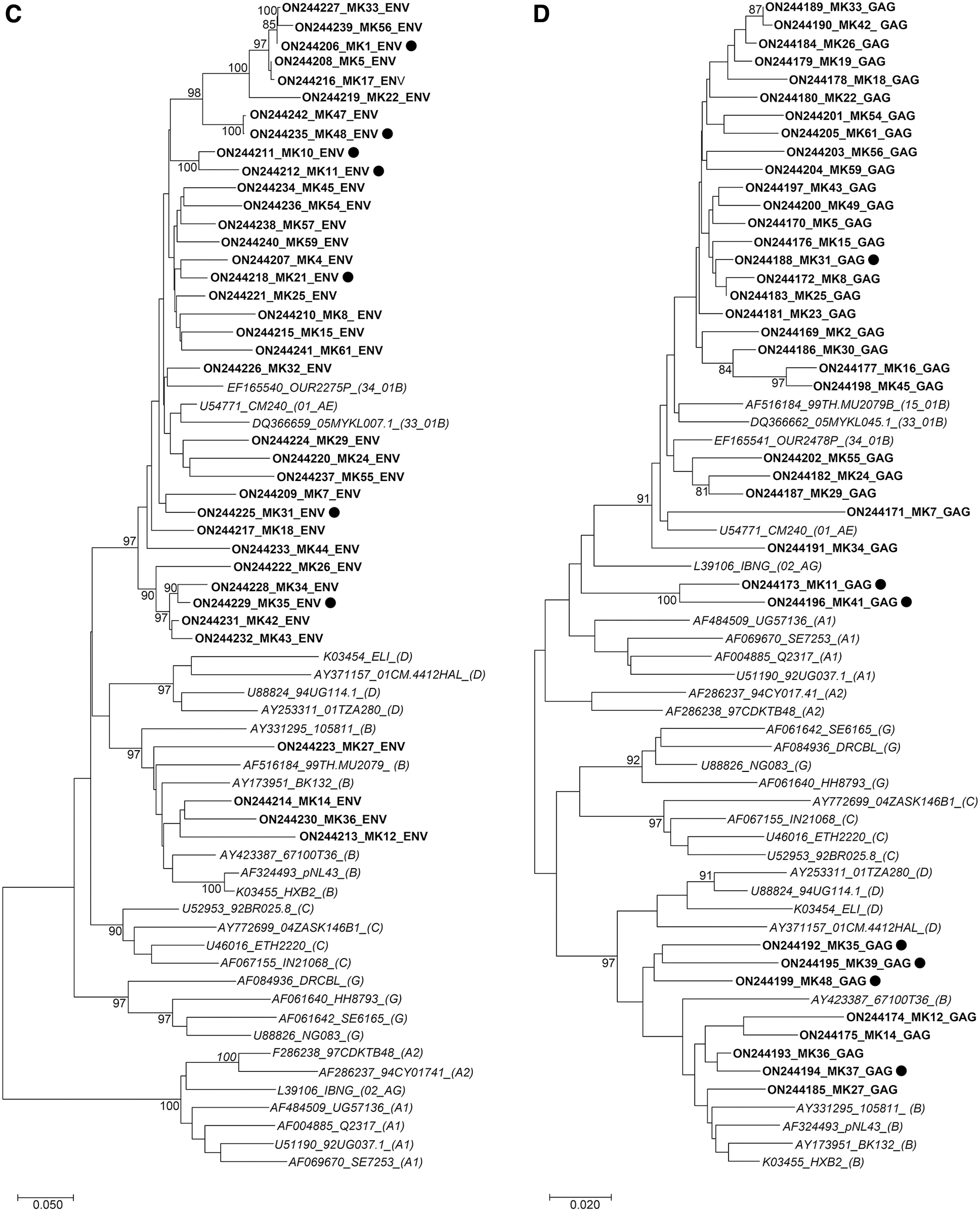
Thirty-eight PR (296 bp), 36 RT (762 bp), 38 env (383 bp), and 39 gag (369 bp) gene fragments were successfully sequenced from 48 samples and subjected to a phylogenetic analysis. According to the phylogenetic tree, RIP, and jpHMM analyses, the distribution of each subtype and CRF were as follows: 33 of 48 (68.8%) were CRF01_AE, 6 of 48 (12.5%) were recombinant viruses containing CRF01_AE and CRF02_AG genomic fragments, 4 of 48 (8.3%) were subtype B, 4 of 48 (8.3%) were recombinant viruses containing CRF01_AE and subtype B genomic fragments, and 1 of 48 (2.1%) was a recombinant virus containing CRF02_AG and subtype B genomic fragments (Fig. 1).
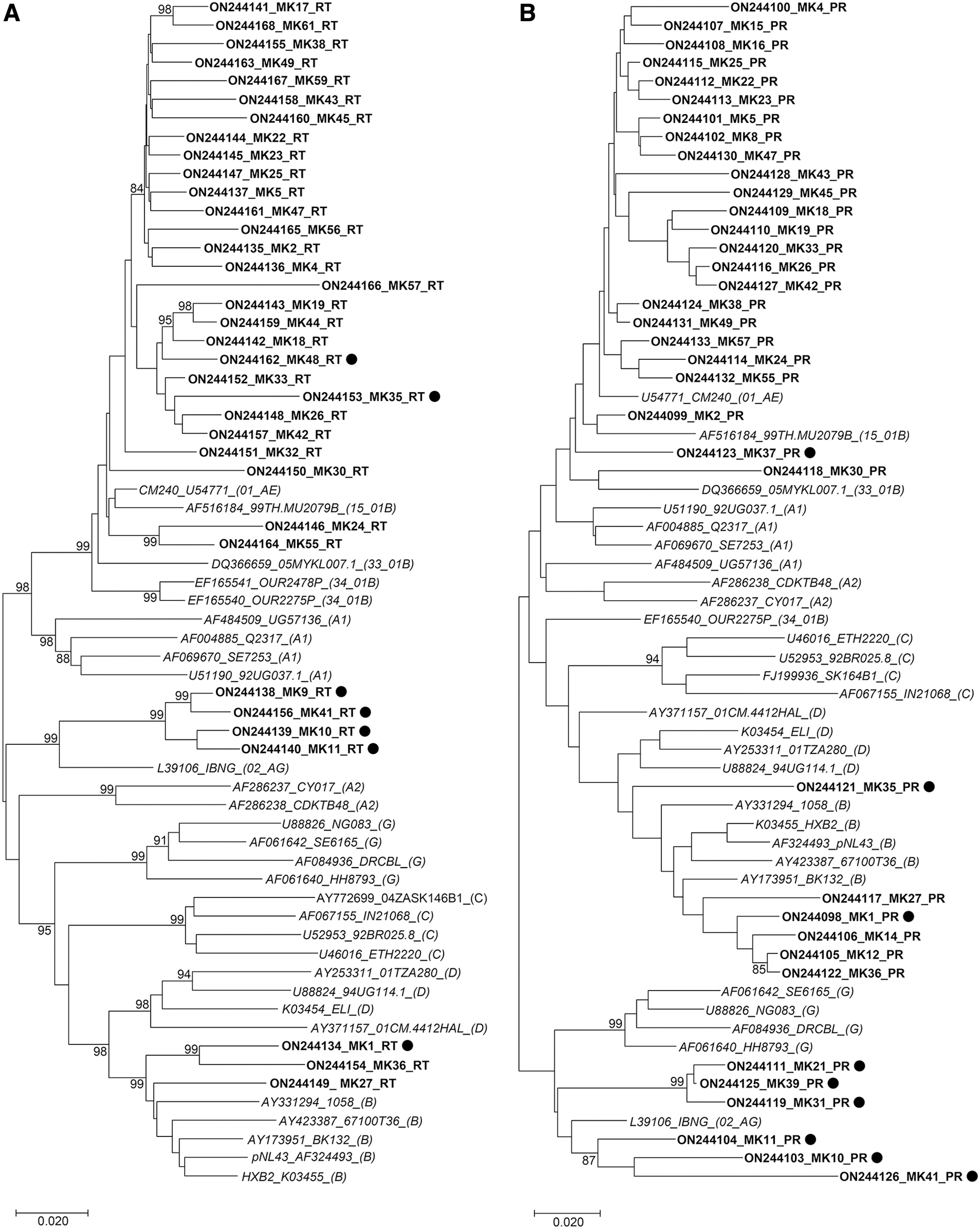
Phylogenetic tree analysis of HIV-1 RT, PR, env, and gag genes collected in Makassar, Indonesia. Phylogenetic trees were constructed for the HIV-1 RT
In this study, CRF01_AE was the predominant CRF in Makassar, Indonesia, similar to other provinces in Indonesia, including Medan, Manado, Surabaya, Jakarta, and Bali. 3
As discovered by the online Genotypic Resistance Interpretation Algorithm (
Drug Resistance Mutations and HIV-1 Subtypes/Circulating Recombinant Forms Detected in Viral Genes Derived from HIV-1-Infected Individuals Receiving Antiretroviral Therapy
Mutations associated with high resistance according to the guidelines published by the International AIDS Society United States (IAS-USA) are shown. Major mutations are shown in bold.
CRF, circulating recombinant form; ETR, etravirine; HIV-1, human immunodeficiency virus type 1; NRTI, nucleoside RT inhibitors; NNRTI, non-nucleoside RT inhibitors; PI, protease inhibitor; RT, reverse transcriptase; RPV, rilpivirine.
The main DRMs found in RT genes were K103N and E138A, which confer resistance to EFV, NVP, etravirine (ETR), and rilpivirine (RPV). Our previous studies on Pontianak and several provinces in Indonesia revealed the emergence of K103N and E138A among 28.6% (2 of 7) and 20.0% (8 of 40) of RT genes derived from ART-treated individuals, respectively. 3,6 In addition, minor DRMs detected in RT genes were V90I and V179D, which confer resistance to ETR. Moreover, major and minor DRMs were detected in two PR genes, MK10 and MK4. The main mutations found were D30N and M46I, which confer resistance to nelfinavir and indinavir/ritonavir.
In contrast, no TDR was identified among ART-naive individuals. Minor DRMs, including M36I (33 of 38, 86.8%), L89M (32 of 38, 84.2%), K20R/I (27 of 38, 71.1%), and I93L/M (19 of 38, 50.0%), were repeatedly detected in PR genes. The aforementioned mutations were discovered to be natural polymorphisms amid CRF01_AE viruses. 8 These results are similar to previous findings showing the presence of minor DRMs affiliated with PR inhibitors in several regions across Indonesia. 3 Nevertheless, treatment outcomes were largely unaffected by the large number of natural polymorphisms found in CRF01_AE. 9
Based on the present results, CRF01_AE was identified as the dominant HIV-1 CRF in Makasar, Indonesia, similar to other regions in Indonesia. In addition, major and minor DRMs conferring resistance to NRTI were frequently found in RT genes derived from ART-experienced subjects. We consider continuous monitoring for the emergence of HIVDR to be necessary to maintain the efficiency of ART and reduce TDR in Indonesia.
Sequence Data
Nucleoside sequences are available under GenBank accession numbers ON244098–ON244205.
Footnotes
Acknowledgments
The authors express their appreciation to all study participants and staff at the Voluntary Counseling and Testing program in Makassar Hospital. This article was proofread by Medical English Service, Kyoto, Japan.
Authors' Contributions
S.Q.K., Nasronudin, and M.K. conceived the study. S.Q.K., N.L.A.M., and S.U. performed the experiments. S.Q.K., N.L.A.M., T.K., A.N.H., and M.K. analyzed the data. S.Q.K. drafted the article. All authors reviewed the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part by the Grant in Aid from Universitas Airlangga (Faculty research excelent Grant No.130/UN3.9.4/PT/2022), the program of the Japan Initiative for Global Research Network on Infectious Diseases (J-GRID) from the Ministry of Education, Culture, Sport, Science and Technology in Japan, and the Japan Agency for Medical Research and Development (AMED); and the Institute of Tropical Disease as the Center of Excellence (COE) program by the Ministry for Research and Technology (RISTEK) of Indonesia.