
Abstract
We sought to describe the prevalence of and motivation for cannabis use and whether legalization of cannabis impacts the frequency and perceived risks and benefits of use in people living with HIV (PWH). The study was based on two HIV clinics located in Cleveland, Ohio, and Aurora, Colorado. Participants responded to a 45-question survey, and responses were summarized in aggregate and stratified by the frequency of cannabis use and site. Three hundred ninety-seven participants completed the survey. The frequency of use was not different between the sites. Daily cannabis users compared with yearly or never users identified the benefits of cannabis as relief from stress, anxiety, or depression, improved sleep, improved creativity, improved focus or concentration, and increased energy. The benefits of pain management, improved appetite, and helping to decrease or stop other medications were selected at similar rates, regardless of the frequency of use. Daily users were less likely to identify treatment of disease as a benefit and legal problems, addiction to cannabis, impaired memory, increased use of other drugs, personal or relationship problems, decrease in intelligence, new or worsening health problems, and getting high as risks of use compared with yearly or never users. Compared with participants in Ohio, Coloradoans were more likely to identify cannabis benefits as decreasing/stopping other medications and getting high, and less likely to identify legal problems and addiction as risks. Legalization of cannabis did not affect the frequency of cannabis use in PWH. Daily cannabis users are more likely to identify benefits and less likely to identify risks of use compared with yearly or never users. A better understanding of the potential benefits and risks of cannabis use can help guide safer use of cannabis in PWH and allow physicians to provide better counseling on risk reduction.
Introduction
Legislation for the legalization of medical use of marijuana has been passed in 36 states and Washington, DC, and for recreational use in 16 states and Washington, DC. 1 In states that have legalized cannabis, rates of regular cannabis use, defined as repeated use not meeting criteria for cannabis use disorder as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 2 are higher. 3,4 However, these higher rates were generally also found even before cannabis was legalized in these states. 5 In the United States, the legalization of cannabis has not resulted in increased use among youth but has been associated with increased use among adults. 6 –8
The prevalence of cannabis use among people living with HIV (PWH) is about 25%, which is higher than use in the general population (<10%). 9 –12 Reasons for cannabis use being more common among PWH have been considered, although rigorous research regarding motivations for cannabis use in PWH remains insufficient. 11,13 –17 In a study comparing PWH with those without HIV, the primary reason for initiation of cannabis use was recreation for both groups; however, PWH were more likely than those without HIV to identify improved mental health and decreased physical symptoms as reasons for continued use. 13
Additional reasons for use in PWH are to improve appetite, address HIV medication side effects including nausea, reduce stress, anxiety, and depression, and manage muscular and nerve pain as well as paresthesias. 11,14 –17 Current evidence for selected effects of cannabis and cannabinoids relevant to our survey has been summarized in Supplementary Table S1 based on a comprehensive review by the National Academy of Sciences, Engineering and Medicine in 2017 and annotated based on Ahmad and Hill. 18,19 Finally, the higher prevalence of use among PWH may be because HIV and symptoms associated with HIV are included among the qualifying conditions for medical marijuana in all states. 1
Cannabis use has also been associated with negative effects such as impaired cognition and pulmonary disease, conditions which PWH are already predisposed to. Previous studies have found that PWH who use cannabis are more likely to have cognitive dysfunction than those who do not. 20 Cannabis use is linked to the development of cannabis use disorder and mental illness. 5 However, the long-term effects of chronic cannabis still need to be investigated. PWH who use cannabis more frequently, such as daily or weekly, are less likely to perceive cannabis use as a risk than those who use less frequently. 10 While substance use other than cannabis has been associated with nonadherence and increased mortality in PWH, the effects of cannabis use on medication adherence, CD4+ cell count, and HIV viral load are inconclusive. 12,15,21 –23
This study is based on two sites, one site in Colorado where cannabis was legalized for medical use in 200024 and recreational use in 2012, and another site in Ohio where cannabis was legalized for medical use in 2016 and has not been legalized for recreational use. 24 –26 We sought to assess the perceived risks and benefits of cannabis use in PWH in the context of differing legal environments. These perceptions may help physicians understand some of the reasons for cannabis use in PWH and allow them to counsel their patients based on the current level of evidence (Supplementary Table S1). 18,19
We expected that cannabis use would be higher in Colorado, where medical and recreational cannabis are legal. We also hypothesized that those who use cannabis more frequently would be more likely to perceive benefits and less likely to perceive risks, as they have chosen to continue to use cannabis. Finally, we anticipated that the participants in Colorado would be more likely to perceive benefits and less likely to perceive risks of cannabis use, as they have greater exposure to cannabis use, both in PWH and in the general population, and its legality could make it seem more acceptable.
Methods
Study design
The two study sites were MetroHealth Medical Center in Cleveland, Ohio, and University of Colorado Health (UCHealth) in Aurora, Colorado. Eligible participants were patients seen in the HIV clinics at each site. Eligibility criteria included the following: age of 18 years or older, HIV infection, and a clinical encounter in the prior 2 years. At the Colorado site, the electronic medical record was used to identify eligible patients and abstract email addresses. The survey link to a REDCap database 27 was then sent out via email up to three times. At the Ohio site, eligible patients were sent a link to the survey through an online patient portal. At both sites, patients were informed of the study's purpose and risks through a cover letter and could choose to participate by clicking the link to the survey. Survey responses were anonymous. The study was approved by the MetroHealth Institutional Review Board and the Colorado Multiple Institutional Review Board (COMIRB).
Questionnaire
A survey was developed to understand the perceived risks and benefits of cannabis use among PWH. Individual risks and benefits were selected based on a national survey of U.S. adults published by Keyhani et al. 28 Questions were adapted from several broadly utilized and accepted tools designed and validated for clinical substance use screening purposes. Among those used were the National Institute for Drug Abuse-Modified Alcohol, Smoking, and Substance Involvement Screening Test (NM-ASSIST) 29 and Alcohol Use Disorders Identification Test–Concise (AUDIT-C). 30 Additional questions were added to assess details of use. A community advisory board of PWH was asked to test the questionnaire and provide comments regarding clarity of questions and survey fatigue-related concerns in two iterations. The survey took on average ∼7 min during test runs. The survey questions can be found in the Supplementary Material.
Data analysis
Demographics were summarized overall and by groups using median (range) and frequency (column percent), as appropriate for continuous and categorical variables, respectively. Data were stratified by clinical site (Colorado or Ohio) and by frequency of cannabis use. Cannabis use frequency was determined by response to this question “Over the past year, how often did you use cannabis?” Respondents selected “never, once or twice a year, monthly, weekly, daily or almost daily.” The frequency of cannabis use was categorized into three groups, namely daily use, weekly or monthly use, and yearly or no use. The Kruskal–Wallis, chi-square (or Person's exact chi-square), or Fisher's exact tests were used to compare groups, as appropriate. Survey responses were aggregated overall, by frequency of cannabis use, and by clinical site. Comparisons between groups were made using Pearson's exact chi-square tests.
Univariable followed by multivariable logistic regression was used to model each survey response (dependent variable) by cannabis use frequency (weekly/monthly cannabis use vs. yearly/never, and daily use vs. yearly/never) and clinical site (Colorado vs. Ohio) (variables of interest), as well as age, sex (male vs. female), race (Black or African American vs. White, Hispanic regardless of race vs. White, and Other racial group vs. White), education level (Bachelor's degree and beyond vs. Associate's degree or less), employment status (employed vs. not employed), yearly income (less than or equal to $20,000 per year vs. more), smoking status (current smoking vs. never and past smoking), alcohol use status (alcohol use at least two to four times per month vs. less), illicit drug use status (current use of illicit drugs other than cannabis vs. no), and the number of substances used (more than one substance including tobacco, alcohol, or illicit drugs vs. no).
Two multivariable models were generated for each benefit and risk. Multivariable model 1 included variables with p < .1 in univariable models with cannabis use frequency included, regardless of significance. Multivariable model 2 included all variables in multivariable model 1 and clinical site, regardless of significance. Adjusted odds ratios (aOR) are reported with a 95% confidence interval (CI). A p value <.05 was considered significant. No adjustment for multiple comparisons was made in this exploratory study. All analyses were computed using SAS 9.4 (Cary, NC).
Results
In Colorado, 249 of 1,874 potential participants completed the survey (12.9% completion rate). In Ohio, 148 of 867 potential participants completed the survey (17.1% completion rate). The demographics of the participants are summarized in Table 1, stratified by cannabis use. Of the 397 respondents, 31% reported daily cannabis use, 17% weekly or monthly use, and 52% yearly or no use, without significant differences between clinical sites (p = .34). Daily cannabis users were younger than those who used less frequently. Weekly or monthly users were more likely to be female than both daily and yearly or never users. Daily and monthly or weekly users were less likely to be White, not Hispanic, to have completed a Bachelor's degree or higher, and to have an annual income greater than $100,000, and were more likely to be disabled than yearly or never users. Daily users were less likely to work 40 or more h/week than yearly or never users.
Demographic and Socioeconomic Factors Overall and by Frequency of Cannabis Use
Data are represented as median (range) and frequency (column percent).
Kruskal–Wallis or Pearson's exact chi-square test for continuous and categorical variables, respectively.
Kruskal–Wallis, chi-square, Fisher's exact, or Pearson's exact chi-square test as above.
GED, General Educational Development.
Participants in Colorado were older [median 53 (range 27–81) vs. 48 (20–67) years; p < .01], with differences in racial distribution (White 69% vs. 61%, Black 10% vs. 28%, Multiracial 5% vs. 3%, Hispanic, regardless of race 17% vs. 9%; p < .0001). While employment status was similar, more respondents in Ohio had an annual income below the poverty level (41% vs. 26%; p < .01) and were less likely to have at least a Bachelor's degree (30% vs. 44%; p < .01). Respondents in Colorado were less likely than those in Ohio to use tobacco (27% vs. 45%; p < .001) or to use more than one substance (16% vs. 26%; p = .02), but the use of alcohol and illegal drugs other than cannabis was similar. Even with differing legal environments, the likelihood of having a cannabis card was similar across sites (21%).
The use of other substances, including tobacco, alcohol, and illicit drugs, is summarized in Table 2, stratified by cannabis use. Daily and weekly or monthly cannabis users were more likely to be current smokers than yearly or never users. Weekly or monthly, but not daily, users were more likely to drink alcohol at least two to four times per month compared with yearly or never users, whereas illegal drug use other than cannabis was similar across groups (8% overall). Both daily and weekly or monthly cannabis users were more likely to use more than one substance than yearly or never users. Daily cannabis users, but not weekly or monthly users, were more likely to have a medical cannabis card than yearly or never users.
Medical Cannabis Card and Other Substance Use Overall and by Frequency of Cannabis Use
Data are represented as frequency (column percent).
Kruskal–Wallis or Pearson's exact chi-square test for continuous and categorical variables, respectively.
Kruskal–Wallis or Pearson's exact chi-square test as above.
Perceived benefits of cannabis use
Participants were asked, “What do you believe are the benefits of cannabis?” and were allowed to select more than one choice. Responses are summarized by the frequency of cannabis use in Supplementary Table S2. Benefits selected at similar frequencies regardless of how often cannabis is used included pain management (81%), improved appetite (65%), to help decrease or stop other medications (33%), and to get high (34%). Perceptions of other benefits were different depending on the frequency of cannabis use. Figure 1 shows aOR for perceived benefits of cannabis by the frequency of use.
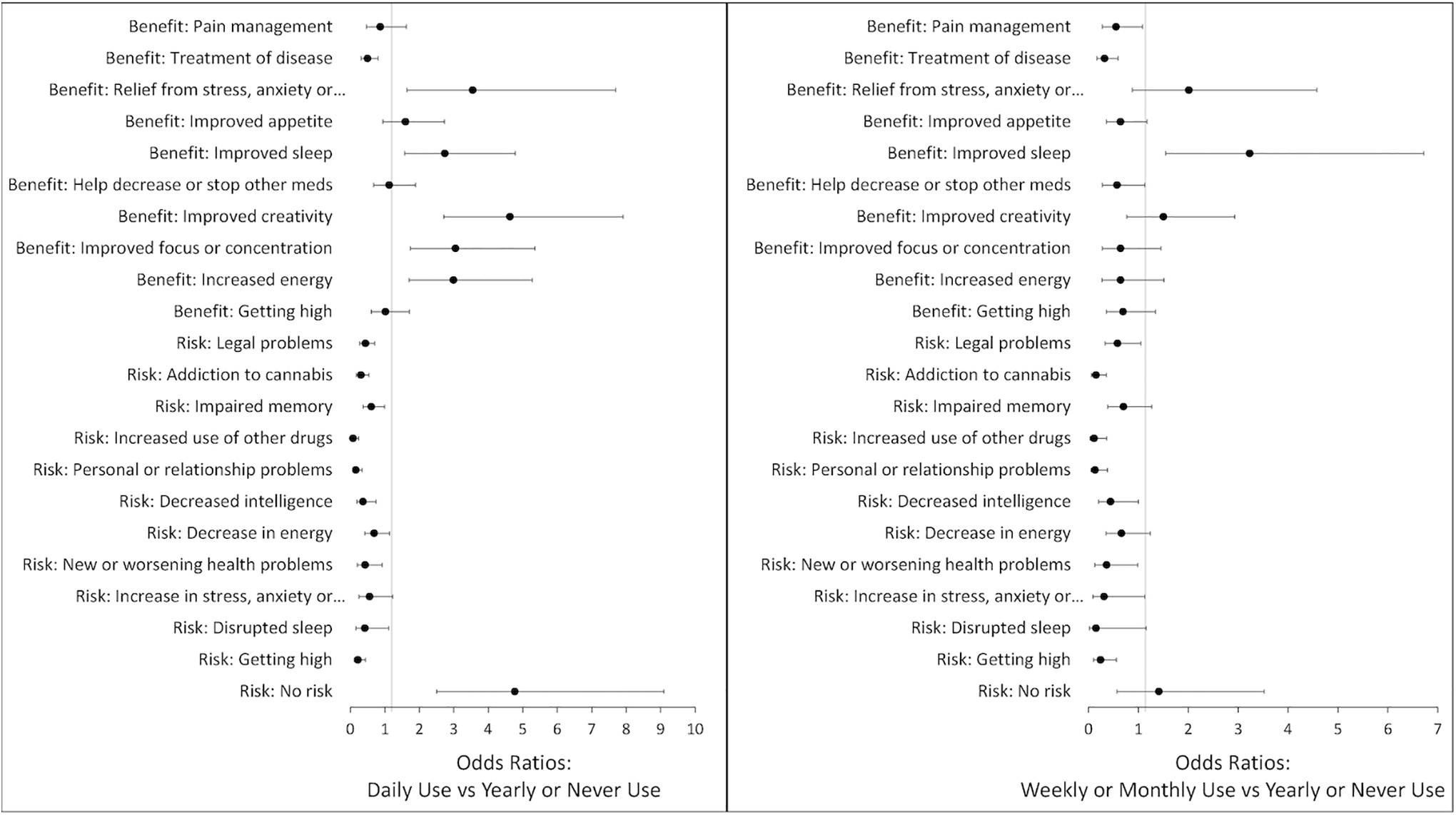
Perceived benefits and risks of cannabis compared with yearly or never cannabis users. Symbols represent odds ratios adjusted for clinical site, sex, race, education level, employment status, yearly income, smoking status, alcohol use status, illicit drug use status, and number of substances used. Error bars are 95% confidence intervals around the adjusted odds ratios.
Daily users were more likely than yearly or never users to select relief from stress, anxiety, or depression (aOR 3.55; 95% CI 1.64–7.69), improved sleep (aOR 2.74; 95% CI 1.57–4.78), improved creativity (aOR 4.63; 95% CI 2.71–7.91), improved focus or concentration (aOR 3.05; 95% CI 1.74–5.36), and increased energy (aOR 2.99; 95% CI 1.7–5.28). Daily users were less likely than yearly or never users to select treatment of disease (aOR 0.5; 95% CI 0.31–0.08) as a benefit of use. Weekly or monthly users were more similar to yearly or never users in their perceived benefits of cannabis use than daily users, with the exception that weekly or monthly users were more likely than yearly or never users to select improved sleep (aOR 3.23; 95% CI 1.55–6.72) and less likely to select treatment of disease (aOR 0.32; 95% CI 0.17–0.59) as benefits of cannabis use.
Perceived risks of cannabis use
Participants were also asked, “What do you believe are the risks of cannabis?” and again allowed to select more than one choice. Responses are summarized by the frequency of cannabis use in Supplementary Table S3. Overall, the risks that were selected at similar frequencies across cannabis use groups were a decrease in energy (35%) and an increase in stress, anxiety, and depression (11%) and disrupted sleep (8%). Perception of other risks varied depending on the frequency of cannabis use. Figure 1 shows aOR for perceived risks of cannabis by the frequency of use. Daily users were less likely than yearly or never users to select legal problems (aOR 0.44; 95% CI 0.27–0.71), addiction to cannabis (aOR 0.31; 95% CI 0.17–0.54), impaired memory (aOR 0.61; 95% CI 0.37–0.99), increased use of other drugs (aOR 0.08; 95% CI 0.03–0.24), personal or relationship problems (aOR 0.16; 95% CI 0.07–0.34), decrease in intelligence (aOR 0.37; 95% CI 0.19–0.75), new or worsening health problems (aOR 0.43; 95% CI 0.2–0.92), and getting high (aOR 0.22; 95% CI 0.11–0.44).
Weekly or monthly users were more similar to daily users in perceptions of cannabis risks than yearly or never users. Weekly or monthly users were less likely than yearly or never users to select addiction to cannabis (aOR 0.15; 95% CI 0.06–0.36), increased use of other drugs (aOR 0.11; 95% CI 0.03–0.37), personal or relationship problems (aOR 0.13; 95% CI 0.05–0.38), decrease in intelligence (aOR 0.44; 95% CI 0.2–1), new or worsening health problems (aOR 0.36; 95% CI 0.13–0.99), and getting high (aOR 0.24; 95% CI 0.1–0.56). Daily users were more likely than yearly or never users to select that there are no risks to cannabis use (aOR 4.78; 95% CI 2.51–9.12); whereas weekly or monthly users responded more similarly to yearly or never users (aOR 1.41; 95% CI 0.57–3.52). Overall, 63 (16%) respondents indicated that there were no risks to cannabis use: 31% of daily users, 13% of weekly or monthly users, and 8% of yearly or never users.
Differences in perceived risks and benefits between sites
Respondents in Colorado were more likely than those in Ohio to identify decreasing or stopping other medications (aOR 1.67; 95% CI 1.02–2.73) and to get high (aOR 2.49; 95% CI 1.53–4.07) as benefits, more likely to select addiction to cannabis (aOR 2.05; 95% CI 1.2–3.48) as a risk, and less likely to select legal problems (aOR 0.28; 95% CI 0.18–0.44) as a risk of cannabis use.
Discussion
Based on previous studies on the use of cannabis after legalization, it was expected that cannabis use would be higher among participants in Colorado, where both recreational use and medical cannabis use are legal. 5,6 However, our study showed that the frequency of use did not differ significantly between participants from the two different sites, suggesting that among PWH, legalization may not have a significant effect on the frequency of cannabis use. However, the different legal landscape between Ohio (medical use only) and Colorado (medical and recreational use) regarding recreational use may have influenced the differences between respective cannabis users in perceiving certain risks and benefits. For instance, ease of access in Colorado may have contributed to the higher perception of risk concerning the development of addiction, as well as a lower perceived risk of legal problems. Similarly, the societal validation by the legal status of recreational cannabis use in Colorado may make it easier to report “getting high” as a benefit. However, overall, there were not as many differences in the perceived risks and benefits between sites as was expected.
Overall daily cannabis users were more likely to feel that there were benefits to use and less likely to feel that there were risks. Treatment of disease was the only benefit that yearly or never users were more likely to select than daily users. The relief of stress, anxiety, or depression, improved sleep, improved creativity, improved focus or concentration, and increased energy were the benefits selected by daily users of cannabis, but these were less likely to be perceived as benefits by those who do not use cannabis frequently. Those who do not use cannabis frequently may perceive the treatment of disease as a benefit because HIV diagnosis is an approved use of medical marijuana, while those who use cannabis more frequently are more likely to perceive benefits related to specific symptoms of their disease or side effects of treatment. Monthly or weekly users were more similar to yearly or never users in their perception of benefits.
One of the reasons for their less frequent use may be that they do not perceive as many benefits as those who use more frequently. Interestingly, only 7 (3%) yearly or never users and none of the other participants felt that there were no benefits to cannabis use, suggesting that the vast majority of PWH do agree that there is some benefit to use. This finding is self-evident in PWH who continue to use cannabis. However, the presence of such belief even in the majority of nonusers is an important finding. Two benefits that were perceived at similar rates among cannabis use groups were improved appetite and pain management.
Improved appetite was selected as a benefit by 71% of respondents. Cannabis was used for appetite stimulation in PWH before widespread access to antiretroviral therapies. However, there have not been conclusive studies that cannabis use is still effective in improving appetite in PWH. 19,20 Pain management was selected as a benefit by 82% of respondents. There is substantial evidence that cannabis is effective in the treatment of chronic pain; however, most studies have looked at a specific condition, such as neuropathy, multiple sclerosis, or chemotherapy-induced pain. 19 The effect of long-term use of cannabis for pain, and for the treatment of pain specifically in PWH still needs to be studied.
Daily users were less likely than yearly or never users to select negative effects of cannabis use, suggesting that there are perceived risks of cannabis use that are not experienced, or not acknowledged, as frequently by those who use cannabis daily. Those who use daily may be biased against perceiving risks of use as they have chosen to use cannabis frequently, although a proportion would likely meet the criteria for cannabis use disorder, which is for all addictive behaviors often associated with psychological processes of rationalization and denial. 31 –33 Of all the respondents, 18% felt that there was no risk to cannabis use; however, daily users were more likely to select that there were no risks than those who used cannabis less frequently.
It is important to counsel patients on the possible risks of use, even if they do not identify that they are experiencing any. While being more similar to yearly or never users in their perception of benefits, monthly or weekly users were more similar to daily users in their perception of risks. Similar to daily users, they may be biased against perceiving risks as they choose to continue using cannabis. However, they were still less likely to select that there were no risks to use than daily users and may be more receptive to counseling on the possible risks of cannabis use.
Daily and weekly or monthly users were more likely to use more than one substance, including tobacco, alcohol, cannabis, and other illicit drugs, than those who reported yearly or never use. This information can help providers identify which patients are at risk of using multiple substances and would benefit from counseling on substance use, especially since substances other than cannabis have been associated with worse HIV outcomes. For example, alcohol and stimulants have been associated with decreased treatment adherence. 22 Daily cannabis users were more likely to have a medical cannabis card than other patients. Asking about whether or not a patient has a medical cannabis card can help physicians identify patients who may be using cannabis daily and open the discussion on the risks and benefits of use.
There were several important limitations to this study. The higher rate of cannabis use in our participants compared with previous studies 9,10,12,22 suggests that PWH who use cannabis may have been more likely to complete the survey. The survey was sent electronically; therefore, those who are more comfortable using technology may have been more likely to respond to the survey as well. Participants may have under- or overreported cannabis use, and paired survey responses from participants and relatives or friends could improve the objectivity of the results. Furthermore, we did not collect details on the route or types of cannabis cultivars, which may have provided greater details on risks and benefits. 34 Finally, the potential for harm reduction through the informed use of naturally occurring cannabinoid combinations was not addressed. For instance, the use of cannabidiol in conjunction with delta-9-tetrahydrocannabinol (THC) has been shown to maintain the pursued positive effects of THC, while reducing its important negative effects, such as paranoia and anxiety. 35
Conclusions
In summary, we found that PWH identified both benefits and risks to cannabis use, regardless of the frequency of use. The frequency of use did not differ significantly between the two sites, suggesting that the legality of cannabis does not affect use in this population. The legal status and stigma of cannabis may influence how comfortable and open health care providers are in discussing its effects and reasons for use. Especially in states where cannabis is approved for medical use, health care providers who treat PWH should be aware of their perceived risks and benefits to appropriately counsel patients on cannabis use based on the summary of current evidence. This would inform safer use of cannabis in PWH and hopefully reduce harms associated with cannabis use.
Footnotes
Authors' Contributions
M.K., G.B., and K.M.E. contributed to the conception and study design. S.L. and G.B. contributed to data acquisition. C.O.H. contributed to data analysis and interpretation. S.L. contributed to drafting the article. All authors were involved in revising the article.
Author Disclosure Statement
C.O.H. has received research grant funding and has served as a consultant for Gilead Sciences and as a consultant for Theratechnologies. K.M.E. has received research grant funding and served as a consultant for Gilead Sciences, and served as a consultant for Janssen Pharmaceuticals and ViiV Sciences.
Funding Information
This study was supported by the National Institutes of Health (NIH)/National Center for Advancing Translational Sciences (NCATS); Colorado Clinical and Translational Science Award (CTSA) grant number UL1 TR002535. Contents are the authors' sole responsibility and do not necessarily represent official NIH views.
Supplementary Material
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.