
Abstract
Diversified antiretroviral therapy (ART) approach is needed in methods that were acceptable to communities and maintain good viral suppression outcomes to reach the UNAIDS targets to end the HIV/AIDS epidemic by 2030. Ethiopia is fully implementing differentiated service delivery (DSD) approaches, appointment spacing, and standard care. This study aimed to determine the time to HIV virological failure and its predictors among patients with a DSD model. An institution-based retrospective cohort study was conducted with data collection dates ranging from May 1, 2021, to May 30, 2021. All adult HIV-positive patients (n = 2,148) between January 2018 and January 2021 were a source population. Data were extracted using a standard checklist by trained data collectors and entered into EpiData, exported to SPSS version 20 for data management, and then exported to R Studio version 1.4 for analysis. Kaplan–Meier survival curves, the log-rank test, and Cox proportional hazard regression models were employed. The incidence of virological failure was 86 per 10,000 person-months. The independent predictors for the hazard of virological failure were being on standard care [adjusted hazard ratios (AHR) = 1.91; 95% confidence interval (CI) 1.07–3.40], primarily educated (AHR = 3.46; 95% CI 1.02–11.72), having no education (AHR = 3.45; 95% CI 1.01–11.85), and ambulatory status at baseline (AHR = 1.81; 95% CI 1.06–3.09). Patients who had a viral load with a detectable range from 50 to 999 at engagement (AHR = 2.65; 95% CI 1.33–5.27) and a 1-month increase in ART for HIV patients (AHR = 1.045; 95% CI 1.01–1.09). The incidence of virological failure was 86 per 10,000 person-months, whereas the incidences were 52 per 10,000 person-months and 71 per 10,000 person-months on appointment spacing model and standard care, respectively, with independent predictors: patient category, educational status, baseline functional status, viral load at engagement, and duration of ART.
Introduction
A
According to a systematic review, the diversified service delivery approach in sub-Saharan Africa has a viral suppression rate of 59%. 4 The percentage of participants on ART who achieved virological suppression increased from 38% to 87%. 5 In a randomized interventional study conducted in Zimbabwe, 47% had a viral load of at least 1,000 copies/μL. 6 According to a systematic review and meta-analysis study, viral suppression was observed across population subgroups with the initiation of community ART, including in men, adolescents, and key populations, at 1 year, with the statement that studies have not found any evidence of viral suppression at 2 years. 7
An Ethiopia population-based HIV impact assessment survey from 2017 to 2018 by Ethiopian Public Health Institution shows that among all HIV-positive adults aged 15–49 years in urban Ethiopia, the proportion with viral load suppression was 68.2%, whereas the proportion of adults aged 15–64 years with viral load suppression was 70.1%: About one third of the adults living with HIV in the urban areas of Ethiopia do not have viral load suppression. 8
Diverse groups of people living with HIV (PLHIV) have different preferences and expectations, and differentiated care is a client-centered strategy that streamlines and adapts HIV services across the cascade to reflect these preferences and expectations while minimizing unnecessary costs to the health system and the client. 2 Taking changing DSD concepts from pilot to scale will be difficult. Countries must assess their unique situation, specify the anticipated client demands in various contexts, introduce suitable models, and be prepared to change programming based on quantitative and qualitative results. 3 Ethiopia uses the appointment spacing model (ASM), a 6-month follow-up approach of differentiated HIV service delivery from these several differentiated care approaches.
The ASM approach was the one used throughout the nation at all ART treatment facilities for stable adult patients. Stable clients in ASM get follow-up appointments for clinical visits and ART refills every 6 months. 9,10 In ASM, clinically stable adults with HIV are those who have been taking ART for at least a year, have no adverse drug reactions that need to be monitored on a regular basis, are not currently ill or pregnant, are not currently nursing, have a good understanding of lifelong adherence and evidence of treatment success, and, in the absence of viral load monitoring, have rising CD4 cell counts or CD4 counts above 200 cells/mm3. Standard care of HIV refers to the usual routine monthly based care of HIV clients for ART refill and clinical evaluation without differentiation. 11
Differentiated HIV care models offer promising opportunities to increase the number of HIV/AIDS patients receiving treatment, enhance the efficiency of services, and streamline operations without placing additional burden on the health care system and with better outcomes for HIV chronic care treatment. 11,12
There is a need to diversify ART distribution using methods that were acceptable to communities and maintain good outcomes such as retention and viral suppression to reach the UNAIDS targets to end the AIDS epidemic by 2030. 5 Studies have shown that these techniques have equivalent outcomes in terms of lowering viral loads and keeping patients compared with standard HIV treatment. No firm conclusions could be reached from research on task shifting or studies reporting cost-effectiveness results. Kenya has started to spread differentiated care models; however, as various models were used to achieve targeted virological suppression, more investigation, quality improvement, and research are needed. 13 Following the initial rollout in 2017, the first multistakeholder evaluation of national DSD implementation in Uganda found that multilevel interventions are required to speed up additional DSD implementation in Uganda from the demand-side and supply-side dimensions. 14
It was difficult to provide quality HIV care services with targeted viral suppression efficiently to a large numbers of patients with diversified needs if the same old clinical care model, based on a “one size fits all” and largely undifferentiated for individual needs, was followed, rather than employing a different approach that would benefit patients to the best way possible. 15 Existing evidence on the clinical outcomes of DSD models for HIV treatment in sub-Saharan Africa was limited in both quantity and quality but suggests that retention in care and viral suppression were roughly equivalent to those in conventional models of care. 4
Ethiopia has adopted various DSD models since the end of 2016 to achieve the 2020 and 2030 viral suppression targets. Appointment spacing is being implemented at full scale. 10 The goal of this study was to assess the risks of patient outcome status in terms of virological failure among patients receiving standard care and the ASM. To contextualize diversified care models such as appointment spacing in our chronic HIV care service and to improve HIV care outcomes, it is necessary to study their successes and failures. This research's findings, which take into account better care outcomes, will be useful to partners working on HIV care with the new DSD model.
Materials and Methods
Study settings
The study was conducted in Debre Berhan Comprehensive Specialized Referral Hospital, which was located 130 km North of Addis Ababa, capital of Ethiopia. It was established in 1937. It was giving curative health care services for more than 2.8 million people. The Hospital gives emergency, inpatient, outpatient, delivery, and specialized services. The ART clinic was one of the departments in the outpatient case team of the hospital.
There is a separate waiting area, follow-up room, adherence counseling room, and out patient department room at the ART clinic. The clinic provides follow-up care for those with HIV (ART and prevention of mother to child transmission). The clinical care for children who have been exposed to HIV is also provided, and they are enrolled in the follow-up if HIV was discovered after a clinical and laboratory evaluation. The clinic has one physician and five clinical nurses trained in the treatment and follow-up of patients with HIV, four adherence counselors, two data clerks, and two pharmacists. The clinic has documentation and medical record documentation unit, in which 2,148 clients have follow-ups in the unit in the 2020/2021 fiscal year. From whom 497 patients were on ASM of care.
Study design and period
A retrospective cohort study design was conducted with a data collection time from May 1, 2021, to May 30, 2021, in the cohort of PLHIV from January 2, 2018, to January 1, 2021.
Study population
Source population: All adult HIV-positive clients on antiretroviral treatment in Debre Berhan comprehensive specialized hospital.
Study population in the exposed group: All PLHIV assigned to ASM at Debre Berhan comprehensive specialized hospital ART clinic.
Study population in the non-exposed group: All PLHIV assigned to standard of care at Debre Berhan comprehensive specialized hospital ART clinic with a history of eligibility of being stable client while they had not assigned in ASM due to any possible reason, that is, self-preference, lack of information about the service, and limited advocacy of the service approach.
Study subject: All HIV-infected individuals sampled from the ASM and standard of care in Debre Berhan comprehensive specialized hospital.
Inclusion and exclusion criteria
Inclusion criteria are as follows: Client aged 15 years and older with an ASM. Client aged 15 years and older with a history or fulfill the eligibility criteria of stable patients.
Exclusion criteria are as follows: Patients with incomplete data and difficult to address such variables through any means of verification (phone review, electronic medical record).
Sample size determination
Using Open-Epi, version 3, the sample size was determined. For the cohort of HIV-positive patients using the usual care and appointment-spacing paradigm, the following factors were taken into account. Retention in care was regarded as the main predictor from the predictors, and it was used to construct the sample size. By taking retention in care into account, virological failure of an HIV patient was considered an outcome variable. Patients using the ASM were classified as exposed, whereas those receiving normal treatment were classified as unexposed.

By considering the following assumption:
n1 = n2 = sample size in the two groups of population
Z 1 = 95% level of confidence
Z 2 = 80% of power
p1 − p2 = minimum meaningful difference in proportion between the exposed and control groups
p 1 = proportion of patients in the ASM
p 2 = proportion of patients on standard of care taken from a 6-monthly based study, which shows the proportion remaining in care retention in adherence club care at 24 months where a greater proportion of participants were still in intervention care (75.0%) compared with standard care (64.1%). 16
In which 
where n1 = sample in ASM and n2 = sample in standard care, with a total of 550 samples.
Sampling procedure
In this study, computer-generated random sampling techniques were used on hospital DHIS2 data in case of selecting the unexposed group. First, medical registration numbers of the patients were recorded from DHIS2 database based on the study period. Then, random generations of numbers were conducted, and then, the sampling procedures were allocated as follows (Fig. 1).
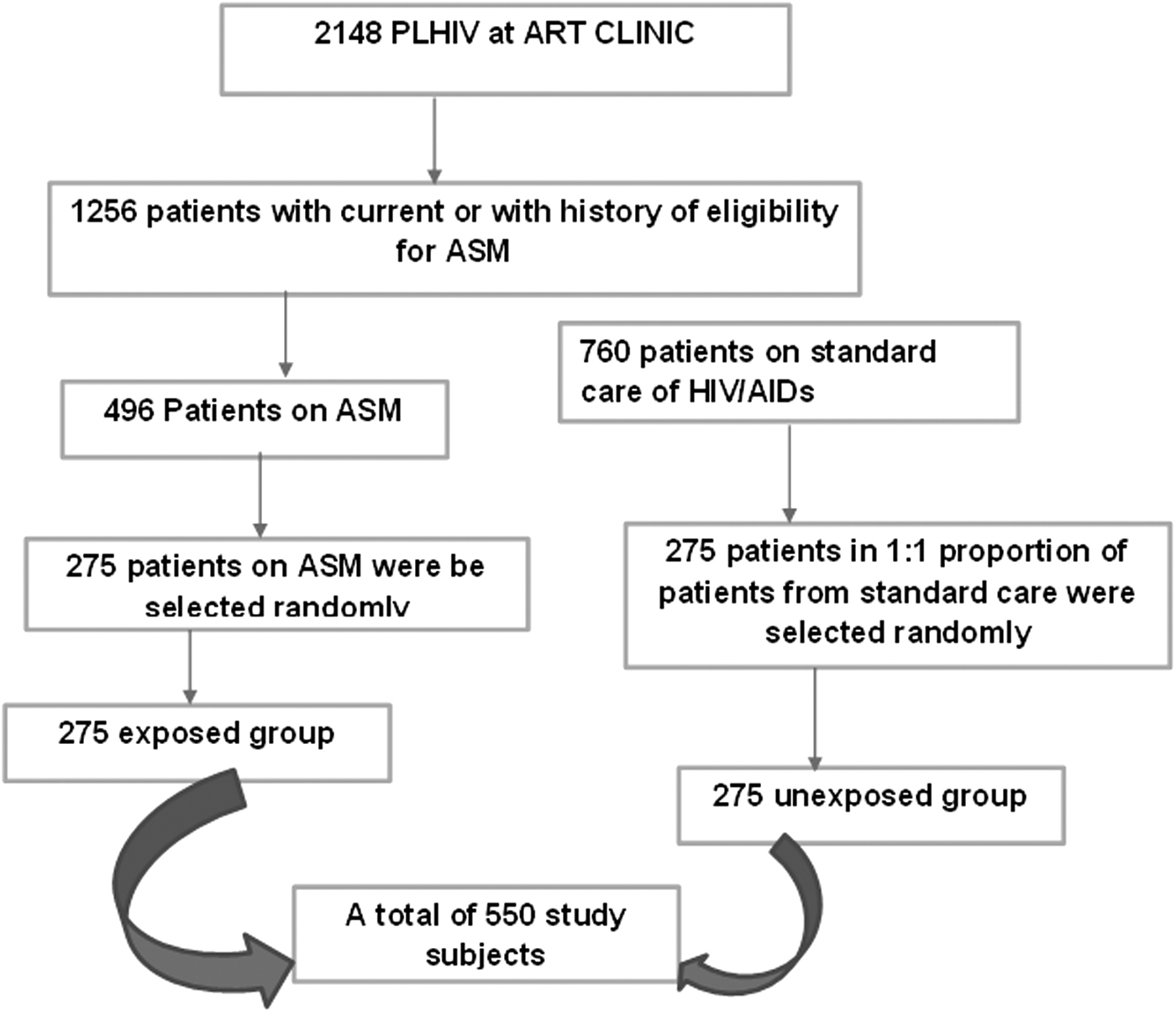
Procedure for taking samples from the patient records at Debre Berhan comprehensive specialized hospital for an investigation into virological failure in differentiated service delivery of HIV/AIDS, 2021.
Data collection method and tool
Data were collected by using standard abstraction format and checklist from the secondary sources. The tools were first prepared in English after reviewing different literatures by considering electronic- and paper-based ART registration and follow-up forms used in the ART clinic. Four data collectors who have been trained in ART were assigned for data collection, and 2-day training were given for data collectors. Patients' medical registration number (MRN) was collected from the ART database; charts were retrieved and reviewed for more required data. The contents of the tools include: demographic factors, baseline characteristics, clinical characteristics, and clinical adherence.
Patients on ART with a class of ASM and standards of care were grouped in the selected ART site from DHIS2 database and their document review. Randomly selected patients MRN were taken in each group. After selecting each group, MRN, the detail of data was collected using the structured data abstraction form and checklist to complete the required data. Abstractions for this study include sociodemographic variables related to gender and age; clinical data pertaining to opportunistic infections; current viral load and CD4 counts and their dates of measurement; date of ART initiation, current and prior ART regimens; number of clinical visits; retention level; outcome-related variables; and baseline characteristics and their outcomes including the dates of ascertainment or censoring of the outcome as a basic interest variables.
Study variables
Dependent variable
Time to virological failure
Independent variables
Demographic characteristics: age, sex, educational level, marital status
Clinical characteristics: opportunistic infection, WHO clinical stage, CD4 count, ART regimen, ART regimen change, were planned for data collection
Baseline characteristics: CD4, viral load, functional characteristics, treatment regimen, opportunistic infection
Adherence characteristics: retention at fixed time points, 6, 12, and 24 months, loss to follow-up, visit level, retention during the era of COVID-19
Data quality management
Data collectors were ART-trained nurses and health officers without the involvement of the authors to avoid information biased and for the sake of clients' confidentiality. Data collectors were trained for 2 days on the purpose of the study and ethical aspects. Pretest was carried out before the actual study to check the reliability and validity of the checklist. The principal investigator assessed the quality of daily collected data in day-to-day manner as supportive supervision during the whole period of data collection. Completeness of the information on all variables as recorded in the registers and the legibility of each filled data in the data collection forms were audited at the end of each day, to ensure that accuracy and chart records with incomplete data were not being included in the sample. To address time-dependent variable in the exposed and unexposed groups, approximately equivalent enrolment of HIV care was considered.
Operational definitions
Virological failure
Record of viral load ≥1,000 copies/mL of blood in HIV-infected patients on standard and ASM after eligibility of ASM or in the course of ASM.
DSD model
A context-based patient-centered appointment spacing (having follow-up every 6 months) and standard model of care (having follow-up care in monthly bases) at Debre Berhan comprehensive specialized hospital.
Exposed cohort
HIV-infected patients on ART with ASM.
Unexposed cohort
HIV-infected patients on ART without ASM while having a history of eligibility for ASM. They were fulfilling the criteria of stable patient or client while they remained in the standard care.
Loss to follow-up
Patients missing their follow-up visits for more than or equal to 2 months, during the course of ASM or after eligibility for ASM.
Incomplete card
When the outcome variable, virological failure, and main independent variables, namely, CD4+ cells, WHO stage, functional status, were not registered.
Transferred out
ART using HIV-infected patients, who were transferred to another ART facility and their dates of transferred-out were also being recorded.
Time to virological failure
Record of viral load ≥1,000 copies/mL of blood in HIV-infected patients on ART after engagement of ASM for those clients on ASM and eligibility criteria fulfillment of client on standard care while time to virological failure will be assessed at a critical follow-up time at 6, 12, 18, 24, and 36 months of the cohort.
Survival time
Follow-up time in a month, from the first date of being on ASM or eligible for ASM up to revealing of virological failure.
Censored
Patients on an ASM or in standard care with or with a history of eligibility for ASM, having an outcome status of lost to follow-up, death, or the one who did not experience the event up to the end of the cohort study.
Data processing and analysis
The information was taken from the patient's file, and then, it was examined for consistency and completeness. For statistical analysis, the data were first entered into EpiData version 3 and then exported to SPSS version 20 and R-Studio version 1.4. To analyze this time to virological failure outcome variable, R was installed with the appropriate packages, including foreign, survival, survminer, ggplot2, and others. Before doing the Cox proportional hazard regression analysis, data exploration techniques such frequency tables, cross-tabulation, nonparametric survival estimates methods, and survival curves were used to summarize and present the data in a clear and useful way. The rate of virological failure during the course of the investigation was shown using Kaplan–Meier survival curves. The log-rank test was utilized to determine if there were variations in virological failure among clients in appointment spacing model and traditional care. Univariable Cox regression models were employed to screen associated factors with the desired outcome using crude hazard ratios and their 95% confidence interval (CI).
Variables whose p values were <.25 were candidate variables for multivariable Cox regression analysis. Likelihood ratio test (LRT) was also used to identify candidate variables in addition to univariable analysis. Multivariable Cox proportional hazard regression model was employed for those candidate variables. Variables whose p values lower than .05 under this model were considered an independent predictor of time to virological failure of HIV patients. The corresponding adjusted hazard ratios (AHRs), their 95% CIs, and p values in the final model were reported. Efron methods were used for parameter estimation. The proportionality assumption of this Cox regression was assessed using Kaplan–Meier curves and log-rank test for each categorical independent variable. Finally, scale Schoenfeld residual plots and global tests for the final model were employed. The insignificant global test value indicates that the proportionality assumptions of the Cox regression analysis were valid (Table 1).
Valid Proportional Assumption of Cox Proportional Hazard Model Among Covariate's in the Over All Global Test (p = .502) of Survival Regression with Evidence of the Test Statistics
This test coincided with the scale Schoenfeld residual plots.
Ethical consideration
Assigned responsible data collectors ensured that all ethical guidelines, particularly those pertaining to the protection of patient medical information, were followed during the data-gathering process. Ethical concerns were also covered during the data collectors' training. The ethics review committee of Debre Berhan University provided ethical assurance. Letters of authorization were acquired from the chosen hospital. Other interested parties, such as the head of the patient card administration, the ART case team leader, and data Clarks, were made aware of the project. The patient's code was utilized as a unique identification, and all information was stored in a way that could not compromise personal privacy.
Results
Sociodemographic characteristics of respondents
A total of 526 adult HIV-positive patients' data were extracted from the patient profile, with 95.6% of patients' complete record. Of the total 263 HIV patients attending on standard care, 45 (17.1%) had virological failure, whereas 19 (7.2%) of the 263 patients with ASM had virological failure (Fig. 2).
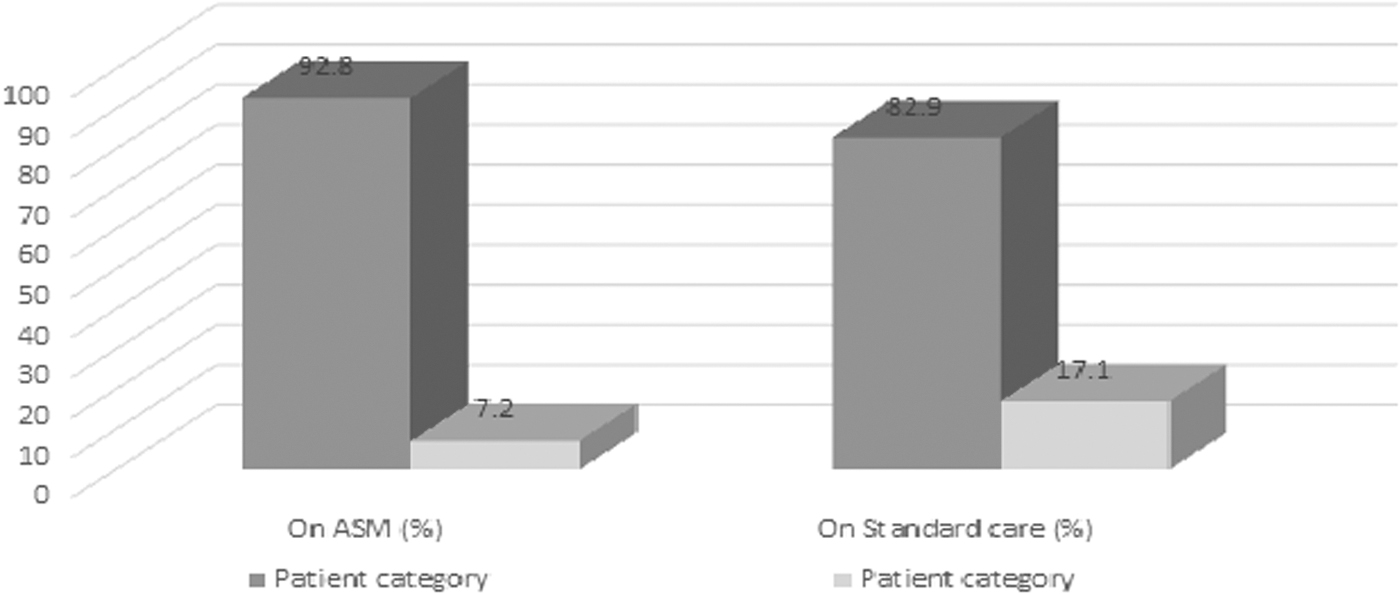
Virological failure based on patient category on HIV/AIDs differentiated care as ASM and standard care at Debre Berhan comprehensive specialized hospital, 2021. ASM, appointment spacing model.
HIV patients who were older than 55 years, patients who had no education and primary education, patients from rural areas, merchant, and farmer patients had a higher proportion of virological failure (Table 2).
Sociodemographic Characteristics on Time to Virological Failure Among HIV Patients Attending at Debre Berhan Comprehensive Specialized Hospital, Debre Berhan, Ethiopia, 2021 (N = 526)
ASM, appointment spacing model.
Baseline characteristics of respondents
HIV patients with baseline clusters of differentiation 4 (CD4) count of ≤200 cells/mm3 had higher proportion of virological failure, whereas patients with CD count of ≥500 cells/mm3 had lower proportion of virological failure. HIV patients with baseline WHO clinical stage who were on stage II had a higher proportion of virological failure than at other stages. HIV patients with baseline functional status of bedridden and patients who had opportunistic infection at baseline had a higher proportion of virological failure compared with its respective categories (Table 3).
Baseline Characteristics of Respondents on Time to Virological Failure Among HIV Patients Attending at Debre Berhan Comprehensive Specialized Hospital, Debre Berhan, Ethiopia, 2021 (N = 526)
1a, d4T-3TC-NVP; 1b, d4T-3TC-EFV; 1c, ZDV-3TC-NVP; 1d, AZT-3TC-EFV; 1e, TDF-3TC-EFV.
ART, antiretroviral therapy; CPT, cotrimoxazole preventive therapy; WHO, World Health Organization.
Clinical-related characteristics of respondents
HIV-positive patients who had a change of T stage after ASM enrolment or eligibility for ASM had higher virological failure of 9 (16.7%) compared with patients who had no change of T stage after ASM enrolment or eligibility for ASM (Table 4).
Clinical-Related Characteristics by Time to Virological Failure Among HIV Patients Attending at Debre Berhan Comprehensive Specialized Hospital, Debre Berhan, Ethiopia, 2021 (N = 526)
T stands for treatment stage with the same criteria with WHO clinical stage criteria while the patient/client takes at least 6 months of ART. For example, T2 means patient with stage 2 defining illness and on ART.
Adherence-related characteristics of respondents
HIV patients who had a history of poor adherence had higher proportion of virological failure compared with patients who had no history of poor adherence. Virological failure for HIV patients who had not counseled for ASM and patients who were lost to follow-up during COVID-19 were in a higher proportion compared with the respective categories (Table 5).
Adherence-Related Characteristics on Time to Virological Failure Among HIV Patients Attending at Debre Berhan Comprehensive Specialized Hospital, Debre Berhan, Ethiopia, 2021 (N = 526)
LTFU, lost to follow up.
Nonparametric survival analysis
The incidence of virological failure was 86 per 10,000 person-months while the median time of virological failure was not achieved as it is found to be 12% virological failure with in this study's data duration.
The Kaplan–Meier survival curve in the right-hand side (cumulative hazard curve) shows that the HIV patients who were on standard care had higher hazard of virological failure than patients who were on the ASM (Fig. 3).
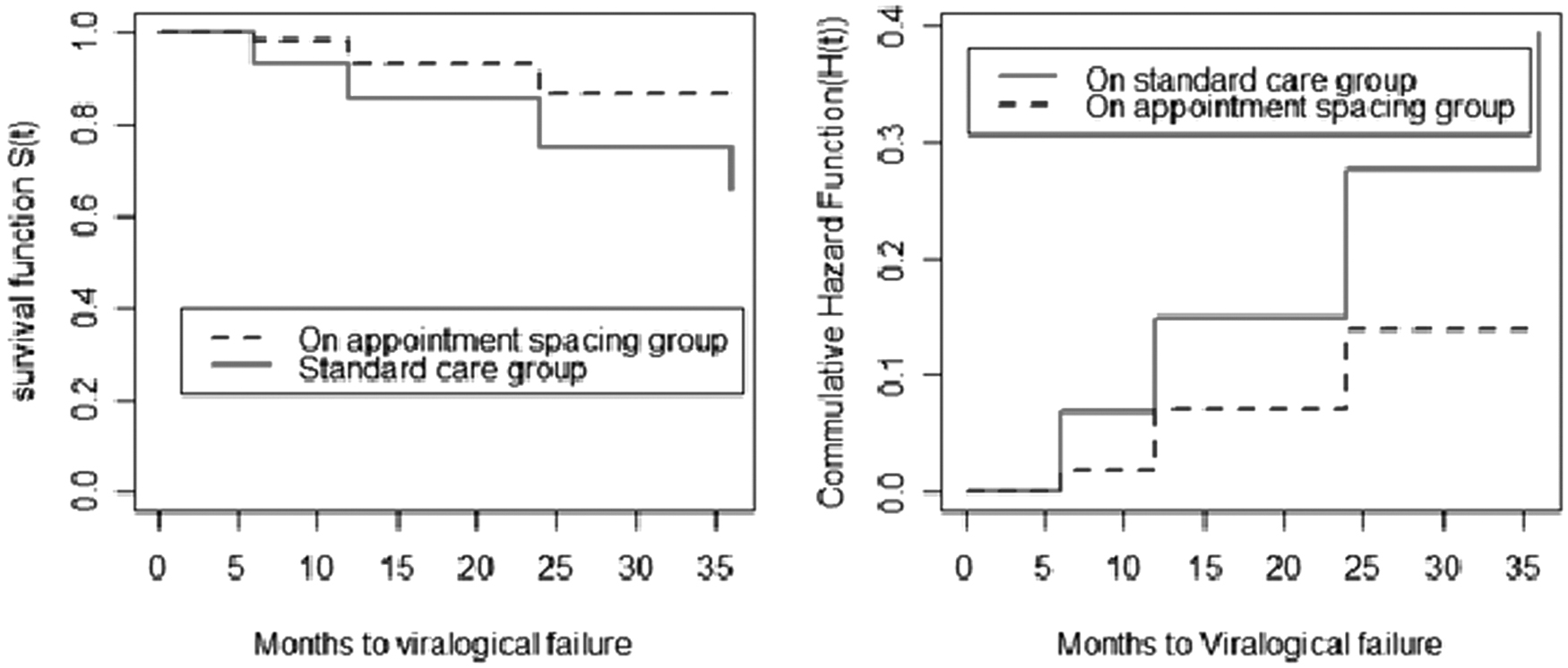
The Kaplan–Meier survival curve and cumulative hazard plot for virological failure among HIV patients attending on standard care and ASM care at Debre Berhan referral hospital, Ethiopia, 2021.
Factors associated with time to virological failure among HIV patients
The results of bivariable analysis showed that the variables, such as patient category, gender, educational status, occupational status, functional status, viral load at engagement, history of poor adherence, counseled for ASM, lost to follow-up during COVID-19, and total months of ART, were found to be significantly associated with time to virological failure at a p value of <.25.
After controlling the effect of other predictors (confounders) in multivariable Cox proportional hazard regression, patient category, educational status, functional status, viral load at engagement, and total months of ART were found to be significantly associated with time to virological failure at p value ≤.05. The hazards of virological failure of HIV patients on standard care were 1.91 (AHR = 1.91; 95% CI 1.07–3.40) times more likely to occur than HIV patients on the ASM. Patients who had primary education were about 3.5 times more likely to have the hazard of virological failure compared with patients who had certificate and above (AHR = 3.46; 95% CI 1.02–11.72), and patients who had no education were almost 3.5 times more likely to have the hazard of virological failure compared with patients who had certificate and above (AHR = 3.45; 95% CI 1.01–11.85).
Patients with ambulatory status at baseline were almost two times more likely to have the hazard of virological failure than patients with working status at baseline (AHR = 1.81; 95% CI 1.06–3.09). Patients who had viral load with a detectable range from 50 to 999 copy/mm at engagement on ASM or at eligibility were almost 2.7 times more likely to develop the hazard of virological failure than patients who had an undetectable viral load at engagement (AHR = 2.65; 95% CI 1.33–5.27). A 1-month increase of ART for HIV patients shows a 1.045 increment on the hazard of virological failure (AHR = 1.045; 95% CI 1.01–1.09) (Table 6).
Associated Factors with Time to Virological Failure Among HIV Patients Attending at Debre Berhan Comprehensive Specialized Hospital, Ethiopia, 2021 (N = 526)
significant, **highly significant, the bold is to show significant measure of association with their interval estimate/confidence interval.
AHR, adjusted hazard ratios; CHR, crude hazard ratios; CI, confidence interval.
Discussion
This study's primary objectives were to quantify the incidence of HIV virological failure and to pinpoint its determinants among HIV-positive individuals on the hospital's differentiated care delivery system in Ethiopia's Amhara regional state, Debre Berhan specialized comprehensive hospital. The incidence of virological failure was 86 per 10,000 person-months in the overall study participants, compared with 71 per 10,000 person-months with study participants in standard care and 52 per 10,000 person-months with study participants in ASM. The results of a semiparametric proportional hazard model showed that patient category, educational level, functional state, viral load at engagement, and overall ART duration were all significant predictors of time to virological failure.
Debre Berhan comprehensive specialized hospital provides DSD with contextualizing patients on appointment spacing in whom patients attend the hospital every 6 months for clinical evaluation and ART refill. However, there are patients on standard care with monthly follow-up. The study focuses on identifying time to virological failure and its predictors in these two categories of DSD. The incidence of virological failure was 86 per 10,000 person-months while the median time of virological failure was not achieved as it was found to be 12% of virological failure. The incidence of virological failure in this study is much lesser than a retrospective follow-up study on first-line ART virological failure in which the incidence of viral load suppression rate was 11.17 per 100 person-months. 16 This difference might be due to difference in study population as its study population includes both stable and unstable clients. These two studies imply the necessity of DSD in HIV care modalities.
According to this study, patients receiving standard care were 1.91 times more likely to experience virological failure than those receiving appointment-spacing therapy. This result affirms the significance and initiative of the unique HIV care program developed by WHO and Federal Ministry of Health (FMOH). 10,11,17 This finding is also in line with studies conducted in clinic-based DSD model in which there are suppressed virological outcomes as the service going on. 18 –20 In contrary, studies conducted in Kenya and a qualitative study in South Africa suggest that these approaches had similar outcomes in viral load suppression and retention in care and were acceptable alternatives to standard HIV care. 13,21 This difference might be due to the difference in socioeconomic status of the study population, accessibility of health care service, and the presence of different support groups of HIV care in the study area. Therefore, this finding implies the need in implementing context-specific patient-centered care and evidence-based services as it results in better virological outcomes.
Virological failures were found to be associated with level of education in which the finding shows that there was a decreased tendency of getting the hazard of virological failure as the respondents became more educated, that is, patients who had primary education were about 3.5 times more likely to have the hazard of virological failure compared with patients who had certificate and above, and patients who had no education were almost 3.5 times more likely to have the hazard of virological failure compared with patients who had certificate and above. However, there are studies on standard care of HIV that do not show association of educational level with virological failure in the differentiated care model, 22,23 in other way, the findings of this study were supported by a sole study on standard care of HIV. This finding demonstrates the significance of education for this outcome. 22
Baseline characteristics and patient disease progression status at the early enrolment of HIV care have a fundamental consequence on the prognosis of ART or other comprehensive care. At baseline, the functional status of the patient is a determinant for occurrence of virological failure as it is highly associated with viral load, CD4 count which intern is highly associated with the presence or absence of opportunistic infection, which corresponds to the presence of physiological and psychological diseases. In this study, patients with ambulatory status at baseline were almost two times more likely to have the hazard of virological failure than patients with working status at baseline with the implication of tracing the importance of HIV-infected patients as early as possible before having impairment of functional status for better outcome of the care.
Viral load is the major determinant factor to categorize patients as stable or engaged in the ASM. WHO and FMOH set the viral load ≤1,000 copy/mL, to say the patient is stable or not, whereas the golden target of HIV care is to make the virological level undetectable or <50 copies/mL, so the interest of this study is to see whether the viral load >50 or <50 copies/mL at engagement of ASM or after eligibility on standard care prediction for virological failure. In this study, the hazards of developing virological failure in patients with detectable viral load 50–999 copies/mL were 2.7 times more likely compared with patients who had an undetectable viral load at engagement. This finding is supported by the ultimate goals of WHO and FMOH guidelines and program targets, which recommend that reaching an undetectable viral load saves the patient from experiencing virological failure. 10,11,24 This implies that differentiated HIV care such as appointment spacing is the right track to realize the ending target of HIV/AIDS in 2030 and achieving the third target of the third 95s.
In this study, the duration of ART refers to the number of months of respondents while taking ART from engagement to ASM or duration after eligibility of ASM. This study considers the duration of ART as an important variable to be assessed as there were indications of virological failure among the length of time from the pharmacological point of view, from patient adherence level, and point of care in the health system. With this consideration, the duration of ART among the respondents was found to be significantly associated with virological failure, in which, the association shows 1 month increase of ART for HIV patients, which shows a 1.045 increment on the hazard of virological failure. This finding were in line with a case–control study on lack of virological suppression that was found to be associated with longer duration of ART. 25 This finding implies that there is an increased risk of virological failure with increased duration of ART with a possible reason of high chance of developing drug resistance, failing the possibility of drug and clinical adherence, gaps in the quality HIV care provision from the health system and care provider side.
Conclusions and Recommendations
The incidence of virological failure was 86 per 10,000 person-months, whereas the incidence was 52 per 10,000 person-months on ASM and 71 per 10,000 person-months on standard care. Patient category, higher educational status, baseline functional status level, viral load level upon engagement or eligibility for the differentiated care approach, and length of ART intake in months were all predictors of virological failure. To improve the virological outcome of HIV care and emphasize the intervention of virological failure, it is preferable to concentrate on strengthening differentiated HIV health care services such as the ASM by taking into account predictors such as patient category, educational status, baseline functional status, viral load, and ART duration.
Limitation of the study
The study appreciates the following limitation beside its valuable findings: since the study is a retrospective cohort study, there were incomplete data in patients' records, and missing of important variables needed to be included in this study. The differentiated care model is not well implemented in every health institution equally, which led the study to be conducted in a single hospital with better care model implementation. In this study, standard HIV care and ASMs were found to be limited in that they created limited discussion parameters.
Footnotes
Acknowledgments
We express our heartfelt acknowledgment to all individual who participated in this study, respondents, data collectors, Debre Berhan University, and Debre Berhan comprehensive specialized hospital for their valuable contributions to this study.
Consent for Publication
All authors declared that they have agreed for publication.
Data Availability
Data are available upon request from the principal investigator.
Authors' Contributions
Conceptualization: A.D.M., W.A.M., H.K.A., A.H.B., and E.T. Data curation: A.D.M., A.L.S., B.T.D., and A.M. Formal analysis: A.D.M., W.A.M., A.L.S., B.T.D., and M.E. Funding acquisition: not applicable. Investigation: A.D.M., W.A.M., H.K.A., A.H.B., A.M.A., and E.T. Methods: A.D.M., W.A.M., H.K.A., A.L.S., A.H.B., and A.M. Project administration: A.D.M., W.A.M., and H.K.A. Software: A.D.M., A.L.S., and B.T.D. Supervision: W.A.M., H.K.A., A.H.B., and A.M.A. Validation: W.A.M., H.K.A., A.H.B., and A.M.A. Visualization: W.A.M., H.K.A., A.L.S., and A.H.B. Writing original draft: A.D.M. Writing, reviewing, and editing: A.D.M., W.A.M., H.K.A., A.L.S., A.H.B., and B.T.D. Accountability: All authors agree to be accountable for this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.