
Abstract
We assessed the effectiveness and safety of switching to generic dolutegravir/lamivudine (DTG/3TC) among People living with Human Immunodeficiency Virus (PWH) in Western India. In this single-center, retrospective observational study, PWH, who switched to DTG/3TC, were followed for virologic, immunologic, and clinical effectiveness, and safety, including weight changes, hyperglycemia, and dyslipidemia. Multivariate linear mixed-effects models were used to predict average change in weight adjusted for age, sex, duration of previous antiretroviral (ARV) regimens, and baseline weight. From May 2017 to July 2022, out of 434 PWH switched to DTG/3TC, 304 with at least 1 follow-up visit were included. Median [interquartile range (IQR)] age was 54 (IQR 49–61) years and 70.1% were male. Prevalence of baseline comorbidities was 57.9% (hypertension—41.5%, chronic kidney disease—40.9%, and diabetes mellitus—18.8%). Reasons for switch were affordability (47.4%), desire for simplification (41.8%), ARV toxicities (19.1%), and concern about potential toxicities (10.2%). Median (IQR) duration of follow-up on DTG/3TC was 40 (IQR 31–49) weeks. No virologic failure was observed. Rates of virologic suppression [viral load (VL) ≤20 copies/mL or target not detected (TND)] at 12, 24, 48, 72, 96 and 120 weeks were 95.2%, 95.9%, 90%, 100%, 81.3%, and 88.4%, respectively. Only 9 (3%) PWH permanently discontinued DTG/3TC. Predicted adjusted mean weight gain of +3.3 kg was observed at 96 weeks. Switching from tenofovir disoproxil fumarate (TDF)/emtricitabine or lamivudine (XTC)/non-nucleoside reverse transcriptase inhibitor (NNRTI) and duration on DTG/3TC were significantly associated with weight gain. Apart from trend in worsening hyperglycemia (nine PWH with new onset diabetes), no clinically significant change in lipids and estimated glomerular filtration rate (eGFR) was documented. Switching to DTG/3TC is an effective and safe option among virologically suppressed PWH with high comorbidity burden in India. In view of the several advantages of DTG/3TC, it may be considered for potential scale-up in the right population, both in private and public health care settings in India.
Introduction
Conventional Highly Active Antiretroviral Therapy (HAART) regimens consist of a backbone of two nucleoside/nucleotide reverse transcriptase inhibitors [N(t)RTIs] and a core antiretroviral (ARV) drug. The core ARV drugs belong to three classes: Integrase Strand Transfer Inhibitors (INSTIs), Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs), or ritonavir-boosted protease inhibitors (PI/r). Two-drug ARV regimens have emerged as an alternative option to conventional HAART. Advantages of two-drug ARV regimens include minimizing toxicity associated with N(t)RTIs, decreasing lifetime cumulative exposure to ARVs, and averting costs. 1,2 These two-drug regimens include a core ARV drug with high genetic barrier to resistance.
Dolutegravir/lamivudine (DTG/3TC) has proven to be effective for the treatment of People living with Human Immunodeficiency Virus (PWH) in both naive and switch indications. Most data on the efficacy and safety of DTG/3TC have been established from rigorously conducted randomized clinical trials (RCTs). 3 –5 In pooled analysis of GEMINI-1 and GEMINI-2 trials, initiating DTG/3TC among ARV-naive PWH was associated with durable efficacy and long-term tolerability at 144 weeks. 3 Switching to DTG/3TC demonstrated noninferior and durable efficacy and safety compared to continuing tenofovir alafenamide (TAF)-based three-drug regimens at 144 weeks in the TANGO trial, and was non-inferior to continuing various three-/four-drug ARV regimens for maintaining virologic suppression at 48 weeks in the SALSA and DOLAM trials. 4 –6
Guidelines for the use of ARVs from high-income settings have recommended use of DTG/3TC in treatment naive and as a switch option among virologically suppression (VS) PWH. 7,8 However, there are limited data on the real-world effectiveness and safety of DTG/3TC across diverse geographic settings. 9 –15 In a retrospective study from Madrid, the use of DTG based dual therapies in practice increased over a period of 5 years, with 89.3% maintaining virologic suppression at week 48. 15 Among PWH in China, switch to DTG/3TC demonstrated excellent virologic efficacy and acceptable safety profile at week 48. 9
India is estimated to have around 2.4 million PWH with overall adult prevalence of 0.21%, one-third of them being 50 years of age or older. As of March 2022, about 77% PWH were aware about their human immunodeficiency virus (HIV) status, 84% received antiretroviral therapy (ART), and 85% on ART were VS. During the same period, globally 85% PWH knew about their HIV status, 88% were on ART, and 68% were VS. 16 Around 1.5 million PWH in India are on ART, mostly provided by public health care settings through the free ART program. The preferred first-line regimen is combination of tenofovir disoproxil fumarate/lamivudine/dolutegravir (TDF/3TC/DTG), and those on tenofovir disoproxil fumarate/lamivudine/Efavirenz600 (TLE600) are proactively being transitioned to TDF/3TC/DTG. 16
A generic version of DTG/3TC fixed-dose combination (FDC) has been available in India since September 2021. We aimed to study the effectiveness and safety of generic DTG/3TC as a switch strategy in routine clinical practice among PWH in Western India. To our knowledge, this is first real-world study on the use of generic DTG/3TC in an Indian population.
Methods
Design
This is a retrospective analysis of routinely collected clinical data from a single-center private clinic from Pune, Western India.
Setting
Institute of Infectious Diseases (IID) is a private clinic [accredited by the National Accreditation Board for Hospitals and Healthcare Providers (Constituent Board of Quality Council of India)] providing comprehensive outpatient care to PWH from Western India. Apart from clinical follow-up, laboratory tests, including viral loads (VL), CD4 counts, and metabolic parameters, are performed at the clinic's accredited laboratory. All data are entered into electronic medical records (EMRs) during routine follow-up. Individuals pay out-of-pocket for medications and laboratory tests. Informed consent (approved by Independent Ethics Committee) for using routinely collected clinical and laboratory data for research is obtained from all PWH at the time of registration at the clinic.
Participants
Inclusion criteria included PWH ≥18 years of age switching to DTG/3TC from May 2017 with at least one follow-up visit. Before the availability of DTG/3TC FDC, PWH were prescribed three pills (one DTG 50 mg + two 3TC 150 mg, once daily). Since September 2021, all PWH used an FDC formulation of DTG/3TC after it was approved and became available. Switch to DTG/3TC were done in PWH with confirmed VL <200 copies/mL for at least 12 months, without historical evidence (either clinically anticipated or evidence of past M184V) of 3TC resistance and after excluding Hepatitis B virus (HBV) co-infection and/or active tuberculosis (TB).
Routine clinical follow-up after initiating DTG/3TC was recommended at 1, 3, and 6 months and every 6 months subsequently. Due to disruption in follow-up due to coronavirus disease-19 (COVID-19) pandemic, follow-up times were approximated to closest scheduled time points within range of ±3 months. The generic DTG/Lamivudine (FDC) used is marketed by Emcure Ltd. Dose of 3TC was not adjusted until estimated glomerular filtration rate (eGFR) was <15 mL/min/m2. 17
Measurements
Baseline demographics (age, sex, date of HIV diagnosis, baseline comorbidities, and prior ARV regimens) were abstracted from EMR. Routine clinical data, including weight, self-reported adherence, and comorbidities, were documented at every follow-up visit. HIV-1 VL (Cobas AmpliPrep/Taqman, v2.0; Roche Diagnostics) were performed every 6 months. CD4 counts (BD FACSCount Cell analyzer; Becton Dickenson) were scheduled to be performed every 6 months. Metabolic screening with fasting blood sugar levels (BSL) and lipid profiles were performed annually and serum creatinine every 6 months after initiation of DTG/3TC.
Hypertension (HTN) was defined based on Indian guidelines on HTN-IV. 18 This includes systolic blood pressure of ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg or any level of blood pressure in individuals taking antihypertensive medications. Diabetes was defined by following criteria: confirmed fasting blood sugar ≥126 mg/dL, or any BSL in individuals taking antidiabetes treatments. 19 Chronic Kidney Disease Epidemiology collaboration (CKD-EPI) equation was used to calculate eGFR. 20 Staging of chronic kidney disease (CKD) using eGFR was based on Kidney Disease Improving Global Outcome (KDIGO) criteria. 21 Reasons for switching to DTG/3TC were documented in EMR.
Objectives
The primary objective of the study was to assess proportion of PWH with VS [VL ≤20 copies/mL or target not detected (TND)] at last follow-up. Secondary objectives for effectiveness included the proportion of PWH with virologic failure (VF; confirmed VL ≥200 copies/mL) and proportion developing/maintaining low-level viremia (LLV; VL 21–199 copies/mL).
Safety objectives included proportion of PWH discontinuing DTG/3TC due to adverse events/death, weight changes assessed by significant weight gain (mean weight change and sustained gain ≥5% and ≥10% from baseline), metabolic outcomes assessed by progression of hyperglycemia (fasting-blood sugar level [F-BSL] ≤99 to ≥126, ≤99 to 100–125, and 100–125 to ≥126 mg/dL), and mean change in lipid parameters and proportions with dyslipidemia (shift to high lipid parameter categories) defined as fasting-total cholesterol (TC) ≥200 mg/dL, low-density lipoprotein cholesterol (LDL-C) ≥130 mg/dL, high-density lipoprotein cholesterol (HDL-C) ≤50 mg/dL, and triglyceride (TG) ≥150 mg/dL. 22 Renal safety was assessed by mean change in eGFR and change in eGFR category from >60 to ≤60 mL/min/m2 (sustained change in eGFR for 3 months).
Statistical analysis
Data on categorical variables were summarized as number (%) and continuous variables were presented as medians and interquartile ranges (IQR). Changes in continuous variables from baseline values for each group are represented as mean differences with 95% confidence intervals (CIs). Values for creatinine/eGFR at last follow-up and highest BSL and lipid parameter values on follow-up were considered to calculate mean change.
Multivariate linear mixed-effects models using a restricted-maximum likelihood method were used to predict average change in weight from baseline. Models were adjusted for age, sex, duration of prior ARV regimen, and baseline body weight. Statistical imputation for missing data was not performed. Bootstrapping with 1,000 bootstrapped samples was used to obtain estimates of 95% CI. p-Values and 95% CI were adjusted for multiple comparisons using the Bonferroni correction. No formal sample size calculations were performed. Data were extracted and cleaned in an MS Excel file. Statistical analysis was done using IBM SPSS Statistics software for Windows, Version 28, and Stata Statistical software for Windows, Version 17.
Results
Study population
From May 2017 to July 2022, among 4,630 individuals in active follow-up, 434 PWH were switched to DTG/3TC, 304 with at least 1 follow-up visit were included in the analysis (Fig. 1). Nine individuals discontinued DTG/3TC within 24 weeks of initiation. One individual discontinued DTG/3TC during the 169th week after being initiated on dialysis for CKD. Death occurred in one individual at 44 weeks after DTG/3TC switch.
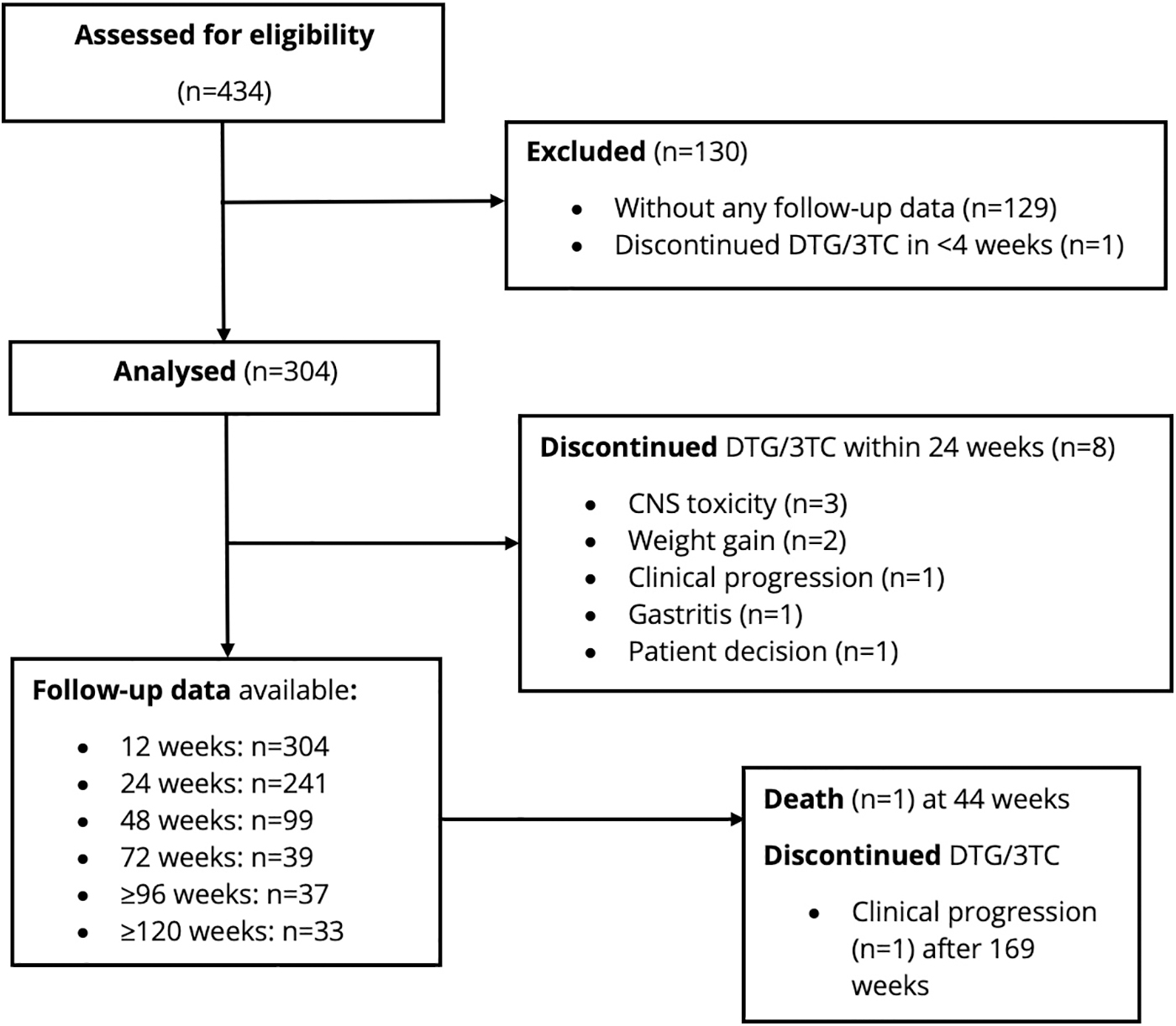
Enrollment and follow-up.
Baseline characteristics
Median age of 304 PWH was 54 (IQR 49–61) years, 70.7% were ≥50 years, and 70.7% were males (Table 1). High rates of comorbidities were prevalent at baseline. Among 57.6% PWH with comorbidities, HTN (41.5%), CKD (40.9%), and diabetes mellitus (DM; 18.8%) were most common. Individuals had long-standing HIV infection (median duration since HIV diagnosis: 15.4 years) and median duration of prior ARV exposure was 12.8 (IQR 9.3–16.3) years. Eighty-nine percent PWH had taken two ARV regimens before DTG/3TC switch (details of pre-DTG/3TC regimens summarized in Supplementary Table S1). Major ARV regimens preswitch included TAF/FTC/INSTI (38.8%) and TDF/3TC/NNRTIs (24.7%). Baseline mean weights (standard error) kg in the TDF/emtricitabine or lamivudine (XTC)/NNRTI, TDF/XTC/ INSTI, TAF/FTC/NNRTI and TAF/FTC/INSTI were 66.8 (1.4), 66.7 (4.2), 68.6 (1.73). and 73.3 (1.16).
Baseline Characteristics at Pre-Dolutegravir/Lamivudine SWITCH
Unless specified otherwise.
Individual comorbidity proportions do not add up since many patients are afflicted with CKD and/or diabetes mellitus and/or hypertension.
ART, antiretroviral therapy; ARV, antiretroviral; BSL, blood sugar levels; CKD, chronic kidney disease; CNS, central nervous system; eGFR, estimated glomerular filtration rate; FTC, emtricitabine; HDL-C, high-density lipoprotein cholesterol; HIV, human immunodeficiency virus; INSTI, integrase strand transfer inhibitors; IQR, interquartile range; LDL-C, low density lipoprotein cholesterol; NNRTI, non-nucleoside reverse transcriptase inhibitor; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate; TG, triglyceride; TND, target not detected; VL, viral load; XTC, emtricitabine or lamivudine.
Reasons for switch to DTG/3TC included affordability (DTG/3TC costs less than three-drug INSTI-based regimens; 47.4%), desire for simplification (41.8%), adverse events on previous ARV regimens (19.1%), and concern about potential toxicities (bone and renal for TDF; 10.2%). Commonest recent adverse events on previous ARV regimens included central nervous system (CNS) toxicity (6.6%) and nephrotoxicity (5.6%). Low-level viremia (21–199 copies/mL) at switch was present in 7.2% PWH. Median pre-DTG/3TC CD4 counts were 601 (IQR 448–776)/mm3. Median eGFR pre-DTG/3TC switch was 85 (IQR 61.1–105.1) mL/min/1.73 m2. Seventy-two PWH had an eGFR ≤60 mL/min/1.73 m2 pre-switch. Approximately 90% PWH had F-BSL values available at baseline with 15.5% and 39.5% individuals having ≥126 and 100–125 mg/dL, respectively. Proportions of PWH with dyslipidemia were slightly higher at baseline (Table 1). Median weight at baseline was 70 (IQR 60–78) kg.
Virologic effectiveness
Median duration of follow-up on DTG/3TC treatment was 40 (IQR 31–49, range 6–280) weeks. High rates of virologic suppression (VS) were maintained after switch. Among 243 individuals with at least 1 VL data available at follow-up, 95.5% had VS at last follow-up (Table 2). One individual had a VL of 91,340 copies/mL at 6 months after DTG/3TC switch; however, it declined to 61 copies/mL when repeated after 3 months. Rates of VS at 12, 24, 48, 72, 96, and 120 weeks were 95.2%, 95.9%, 90%, 100%, 81.3%, and 88.4%, respectively. Virologic outcomes at last follow-up among PWH switched to DTG/3TC are summarized in Table 2. Figure 2 depicts Kaplan-Meier curve for survival free with VL >20 copies/mL. No VF was noted postswitch. There was no difference in rates of VL ≤20 copies/mL/TND according to subgroups, including preswitch ARV regimens (Table 3).
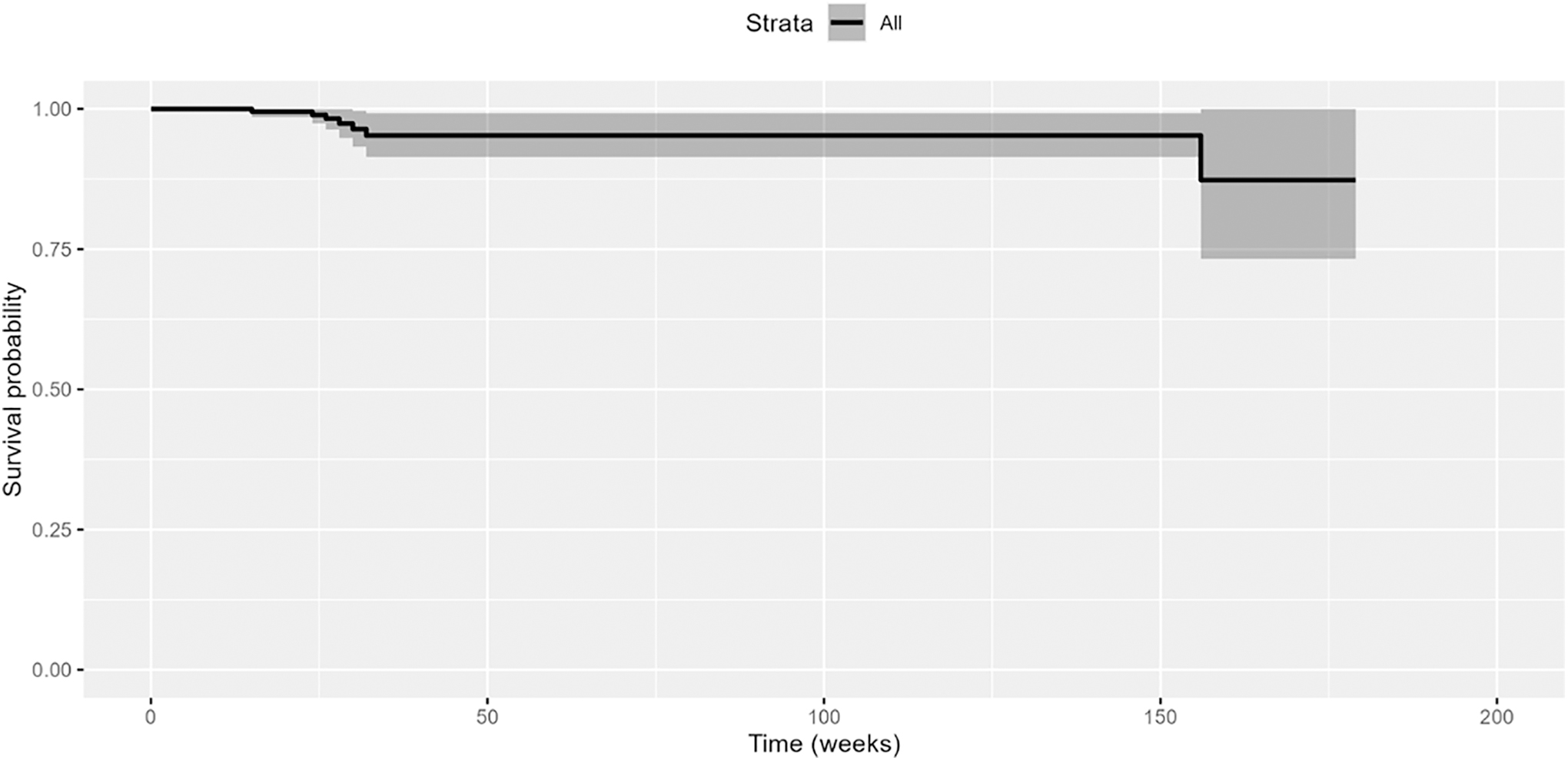
Kaplan-Meier curve for survival free with VL >20 copies/mL. VL, viral load.
Virologic Outcomes at Last Follow-Up Among People with Human Immunodeficiency Virus Switched to Dolutegravir/Lamivudine
Virologic Outcomes (Viral Load <20/Target Not Detected) at Last Follow-Up According to Subgroups
“—” Indicates unstable results on binary logistic regression due to 100% VL ≤20/TND (outcome) achieved in at least 1 factor level.
CI, confidence interval; OR, odds ratio.
Seven individuals with VL ≤20 copies/mL or TND developed LLV at last follow-up, while 3 individuals continued to maintain LLV.
Immunologic and clinical effectiveness
Total number of CD4 counts performed after initiating DTG/3TC was 36. Determining CD4 counts is optional among PWH after achieving sustained VS and CD4 counts ≥350/mm3. Clinically insignificant median change in CD4 count (−31/mm3, 95% CI −77.5 to 15) on follow-up was noted. No clinically significant change in CD4 count categories was documented during follow-up. Only two individuals had a CD4 count drop >30%; however, these were single measurements.
One participant developed pulmonary TB, necessitating discontinuation of DTG/3TC. No other clinically significant HIV-related event occurred.
Adverse events
Twelve (3.9%) individuals self-reported adverse events. Nine individuals permanently discontinued DTG/3TC. Reasons for discontinuation include insomnia (n = 3), weight gain (n = 2), gastritis (n = 1), CKD needing dialysis (n = 1), and development of TB (n = 1) and unaffordability (n = 1). Median time to discontinuation was 15 (IQR 14–20) weeks.
One death was reported in an individual due to CKD and fluid overload. This individual was obese, had HTN and CKD, was regularly taking DTG/3TC for 44 weeks, and was VS 2 months before death.
Weight changes
The change in predicted adjusted mean weight over time after DTG/3TC switch stratified according to baseline regimens is shown in Figure 3. Adjusted mean change from baseline in weight at 96 weeks was +3.3 (95% CI 2.3 to 4.4) kg for overall population. Individuals who switched from TDF/XTC/NNRTI had statistically significant difference in adjusted mean change compared to those who switched from TAF/FTC/NNRTI [+1.8 kg, 95% CI (0.45 to 3.1), p = .003] and TAF/FTC/INSTI [+1.9 kg, 95% CI (0.84 to 3.1), p < .001], but not compared to those switching from TDF/XTC/INSTI [+1.4 kg, 95% CI (−1.1 to 3.9), p = .810].
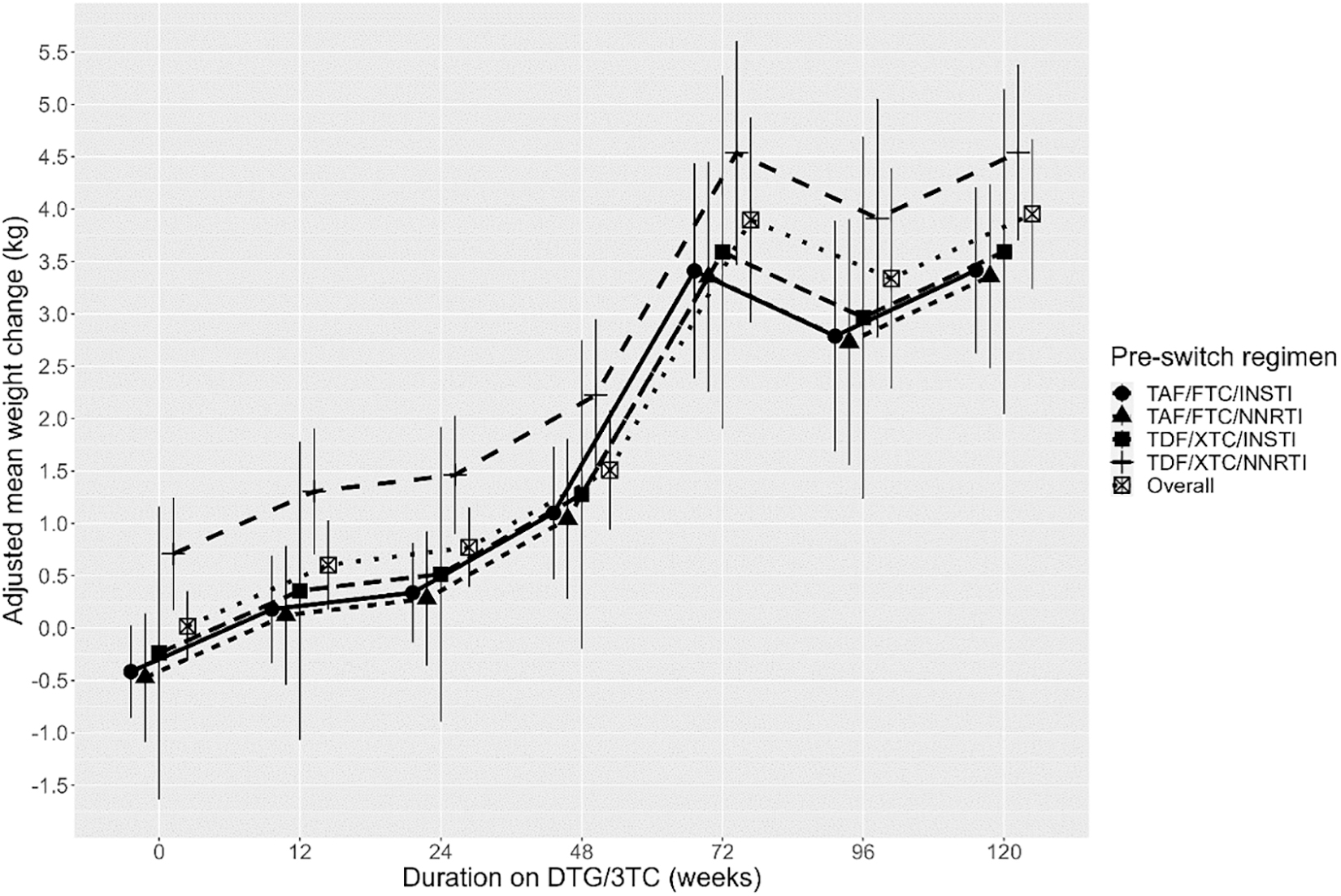
Adjusted mean weight change stratified according to pre-DTG/3TC regimens. DTG/3TC, dolutegravir/lamivudine.
Duration on DTG/3TC was significantly associated with adjusted mean change in weight over time. Compared to baseline, adjusted mean weight (kg) change at 12, 24, 48, 72, 96, and 120 weeks was +0.12 (p = .121), +0.8 (p = .091), +1.5 (p < .001), +3.9 (p < .001), +3.3 (p < .001), and +4.0 (p < .001), respectively.
Sustained weight gain of ≥5% and ≥10% was seen in 6.4% and 2.4%, respectively (Table 4). Higher proportions of PWH gained weight ≥5% after switching from TAF/FTC/NNRTI (5.7%) and TDF/XTC/NNRTI (5.6%). However, weight gain ≥10% was only observed in higher proportions for PWH (5.5%) switching from TDF/XTC/NNRTI.
Rates of Confirmed Weight Gain ≥5% and ≥10% on Dolutegravir/Lamivudine According to Preswitch Regimens
Metabolic changes
Proportion of PWH with BSL ≥126 increased from 47/275 (15.5%) at baseline to 38/98 (38.8%) on follow-up [difference 22.8%, 95% CI (12.1 to 33.5)]. There was a trend toward progression of hyperglycemia from 100–125 and ≤99 to ≥126 mg/dL among 16 and 4 individuals, respectively (Table 5). Among PWH with baseline BSL ≤99 mg/dL, 15 (50%) had BSL 100–125 mg/dL on follow-up. Nine PWH developed new-onset diabetes during the study.
Metabolic Safety-Progression in Metabolic Measures from Baseline, Postswitch to Dolutegravir/Lamivudine Stratified According to Preswitch Antiretroviral Regimens
N indicates number of individuals with observations.
TC, total cholesterol.
Mean change (mg/dL) in TC, LDL-C, HDL-C, and TG after DTG-3TC switch was −19.5, +3, −12, and −7.6, respectively. Proportion of individual's progression within the lipid parameter categories is summarized in Table 5. These changes in lipid parameters are clinically insignificant, except for higher proportions progressing to HDL-C ≤ 50 mg/dL.
Changes in eGFR
Mean change in eGFR for overall population was 4.7 mL/min/1.73 m2 and there was no clinically significant change in eGFR stratified according to baseline regimens (Table 6). Change in eGFR from >60 to ≤60 mL/min/1.73 m2 sustained over 3 months was noted in 4 (3.0%) individuals. All the four individuals had HTN and three had concomitant DM. The fall in eGFR to ≤60 mL/min/1.73 m2 occurred at median of 12 weeks after DTG/3TC switch. None of these individuals progressed to CKD category G3b through to last follow-up visit.
Renal Safety-Change in Estimated Glomerular Filtration Rate from Baseline Postswitch to Dolutegravir/Lamivudine Stratified According to Preswitch Antiretroviral Regimens
N indicates number of individuals with observations.
Discussion
This study documents excellent virologic, immunologic, and clinical effectiveness, and safety of generic DTG/3TC as a switch strategy among VS PWH from three-drug ARV regimens in a real-world setting in India. Advantages of switching to DTG/3TC include avoiding toxicities, lower cumulative ARV exposure, and cost savings. A modeling study documented the potential to offer significant health care cost savings with switch to DTG/3TC in the United States. 23 In India, a similar modeling study demonstrated cost-effectiveness of use of DTG-based three-drug ARV regimen for treatment-naive PWH. 24 Using DTG/3TC in ARV-naive individuals in our clinic is limited by the need to perform baseline VL that is expensive and longer turnaround time for results.
Our PWH cohort had a high prevalence of baseline medical comorbidities like HTN, CKD, and DM. Among PWH with CKD, preswitch regimens mostly included ABC or TAF. Use of TAF is recommended without dose adjustment until eGFR declines to <15 mL/min/1.73 m2. 25 Use of TAF may be associated with higher risk of renal toxicities in the presence of comorbidities. 26 The association of use of ABC with myocardial infarction is unclear, but studies have attributed this risk to channeling bias due to preferred use of ABC in PWH with CKD, which is an independent risk factor for adverse cardiovascular events. 27
Hence, a proactive change may be considered in this context and was an important reason for switch to DTG/3TC in our setting. Other common reasons for switching included desire for simplification, concern for future ARV toxicities, and averting costs. Adverse events associated with pre-DTG/3TC ARV regimens were next common reason for switch. The prevalence of baseline metabolic comorbidities was low in the SALSA and TANGO trials, with an eGFR <30 mL/min/1.73 m2 being an exclusion criterion in the SALSA trial. 5,28 In contrast, the major reasons for switching to DTG/3TC in real-world situations include renal toxicity, dyslipidemia, and request for simplification. 10,29,30 Our study suggests the beneficial potential of DTG/3TC switch in PWH populations with high rates of baseline comorbidities and/or toxicities; however, comparison with other ARV regimens is needed for further confirmation of these findings.
No VF (VL ≥200 copies/mL) was documented at follow-up in our study. Maintaining high VS rates may be attributed to high adherence levels and regimen safety, despite some disruption in follow-up care due to the COVID-19 pandemic. At our clinic, teleconsultation and couriering medicines were used to ensure adherence during this period. Sustaining high adherence rates may also be a function of pill burden; DTG/3TC is available as one pill once a day regimen. More than 95% VS rates have been seen with DTG/3TC switch in RCTs and real-world scenarios. 5,9,11,4,31 –33 Durable VS (96.4%) at week 240 has also been shown in a retrospective study of switching to DTG/3TC among Italian PWH. 30
Of individuals with CD4 count data, no clinically significant change was documented. CD4 counts were not performed routinely among VS PWH after achieving CD4 counts ≥350/mm3. With a pre-DTG/3TC median CD4 count of 601/mm3; and continued VS postswitch, a significant drop in CD4 counts is highly unlikely. Good CD4 count responses have been reported in RCTs and real-world studies. 5,9,11,31 –33 Only one death unrelated to DTG/3TC was documented in our study. No significant HIV-related clinical progression (except one PWH with TB) was seen throughout follow-up.
Very few adverse events leading to treatment discontinuation were noted in our study. Out of nine PWH, four discontinued due to reasons other than adverse events (TB, CKD needing dialysis, and cost). While doubling the dose of DTG has been shown to be efficacious when a three-drug DTG-based ARV regimen is used concomitantly with rifampicin, no data are available for use of DTG/3TC in this context. 34,35 Further studies need to be undertaken to develop strategies for using DTG/3TC with concomitant rifampicin, as TB continues to occur in some PWH at higher CD4 counts in our settings. Very few drug-related adverse event (AE) leading to treatment withdrawal were reported in the TANGO and SALSA trials, with no occurrence of drug-related serious adverse events. 4,5 In real-world scenarios, rates of AEs and AEs leading to treatment discontinuations with DTG/3TC switch were minimal in both short- and long-term studies. 9,30
Weight gain after initiating or switching to an INSTI-based regimen is a major concern. 36 Among VS PWH in the HIV-outpatients study cohort (HOPS), switching to INSTI-based regimen was associated with an increase in body mass index (BMI). 37 In our study, small increases in weight were noted after DTG/3TC switch. Only 2.4% PWH gained more than 10% weight, seen mostly among PWH switching from TDF/XTC/NNRTI. Adjusted mean change in weight from baseline to week 48 was 2.1 kg in the SALSA study and 2.2 kg from baseline to week 144 in the TANGO study. 4,5
In our study, switching from TDF/XTC/NNRTI compared to other ARV regimens and duration on DTG/3TC was significantly associated with adjusted mean weight gain. Considerably more weight gain was observed in a retrospective observational study when switching from TDF/FTC/EFV to INSTI-based regimens versus continuing the same. 38 In a meta-analysis of pre-exposure prophylaxis trials, the use of TDF has been associated with weight loss >5% when compared to placebo or cabotegravir. 39 Impaired weight gain with EFV may be partially associated with CYP2B6 slow or intermediate metabolizer genotype. 40,41 Monitoring for weight gain and BMI after switching to DTG/3TC, especially from TDF/XTC/EFV regimen, is critical.
Initiating ART with INSTIs has been associated with higher incident risk of DM, likely associated with weight gain. 42 Risk of new onset DM/hyperglycemia within 6 months of initiating ART was higher with an INSTI-based versus non-INSTI-based regimen in an analysis of large administrative databases in the United States, with highest risk for elvitegravir followed by DTG. 43 However, data on the risk of hyperglycemia after initiating DTG/3TC are unclear due to small event numbers. In the SALSA trial, three PWH in the DTG/3TC group reported new-onset DM compared to one in the comparator arm. 5
However, no difference in the proportion of participants with insulin resistance, as defined by Homeostatic Model Assessment for Insulin Resistance ≥2, was seen in both the SALSA and TANGO trials through 48 and 144 weeks, respectively. 4,5 Although limited by small numbers, trend in worsening hyperglycemia was seen in our participants, especially after switching from NNRTI-based regimens. Further analysis to determine risk factors was not done. The mechanism of INSTI- or DTG-associated risk for DM is unclear; an association with altered macrophage fatty acid metabolism has been observed. 44 Periodic monitoring of BSL is warranted among PWH switching to DTG/3TC.
There was no clinically meaningful change in eGFR among PWH after DTG/3TC switch in our study. Four individuals developed CKD; however, this may be attributed to underlying comorbidities. When switching from three-drug non-INSTI-based regimens, a benign decrease in eGFR is expected due to inhibition of tubular secretion of creatinine by DTG. 45 No clinically significant impact on eGFR has been reported in RCTs and real-world settings post-DTG/3TC switch. Monitoring creatinine after switch to DTG/3TC may be discontinued or performed less frequently if other underlying risk factors are absent.
Marginal increase in the proportion of PWH progressing into higher category of lipid parameters was noted in this study. However, this is limited by the small number of observations and needs to be confirmed with longer follow-up data. In a post hoc analysis of the TANGO study, PWH, who switched to DTG/3TC, experienced favorable changes in lipid parameters, which were generally greater among those who switched from boosted baseline regimens. 28 In a real-world study among Chinese patients, incidence rate of AEs caused by elevated TC and TG did not change post-DTG/3TC switch, but the proportion of those with normal LDL-C decreased from 88.4% to 75%. 9
Chronic HBV infection needs to be ruled out before DTG/3TC switch and can pose a challenge in settings with high burden of HBV infection and limited access to screening tests. India is categorized in the intermediate HBV endemic countries with a prevalence of 2%–4% in the general population and 3.4% among heterosexual and pregnant PWH. 46,47 While rapid point-of-care HBV screening tests are widely available in India, a major challenge is the lack of health care personnel awareness regarding the importance of diagnosis of chronic HBV infection in various situations. Strengthening of training of health care personnel is critical for routine screening for chronic HBV infection in high-risk populations, including PWH.
Our study has some limitations, including single-arm design, impact of unmeasured confounders, nonavailability of height measures for all PWH precluding calculation of BMI, unavailability of data on lifestyle changes that may impact weight changes, nonuniform follow-up because of COVID-19 pandemic disruption and inability to perform all scheduled VL tests due to cost issues, and approximation of follow-up times to ±3 months and limited number of individuals at extended follow-up times. Almost one-third PWH were excluded from the analysis as no follow-up data were available after DTG/3TC switch.
However, no difference in baseline characteristics was observed between those excluded and included in the study (Supplementary Table S2). Most PWH had one VL measurement on follow-up. However, many measurements were performed at or beyond 48 weeks post-DTG/3TC switch due to challenges in accessing care during the COVID-19 pandemic. Moreover, all PWH with more than one VL measures continued to maintain virologic suppression. Nevertheless, durability of virologic suppression post-DTG/3TC switch should be interpreted with caution. Formal statistical testing to determine significance was not done due to the impact of multiplicity analysis. This study was carried out in a private institute, although similar results may be expected in settings that provide free treatment and laboratory tests.
Conclusions
In conclusion, DTG/3TC confirmed its effectiveness and safety as a switch option from three-drug ARV regimens among PWH with high baseline comorbidity burden in Western India. This study adds to literature on the use of generic DTG/3TC as a switch strategy in diverse geographic settings. In view of several advantages of DTG/3TC, it may be considered for potential scale-up in the right population, both in private and public health care settings in India.
Footnotes
Acknowledgments
We would like to thank all individuals consenting to providing routinely collected clinical and laboratory data for research analysis.
Authors' Contributions
Sa.P. designed the study and drafted the article, S.G. and A.C. conducted research and extracted data, Su.P. performed data analysis, D.D. and C.R. performed laboratory test, and K.J. and V.B. conducted research and ensured quality control of the data.
Author Disclosure Statement
Sa.P. has received speaker fees from Emcure Ltd. All other authors have no competing financial interests exist.
Funding Information
No funding was received for the work reported in the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.