
Abstract
Despite the accuracy of confirmatory tests for the diagnosis of human T cell lymphotropic virus (HTLV), inconclusive or false-negative results still occur when diagnosing human T cell lymphotropic virus type 2 (HTLV-2)-positive patients. The goal of this study was to evaluate the sensitivity and accuracy of a confirmatory immunoassay, the Multi-HTLV assay. A total of 246 plasma samples were tested by real-time polymerase chain reaction (qPCR) and used to calculate the sensitivity and typing accuracy of the Multi-HTLV assay. Of the 246 plasma samples, 127 were positive for human T cell lymphotropic virus type 1 (HTLV-1), 112 were positive for HTLV-2, and 7 were positive for both HTLV-1 and HTLV-2. Thereafter, the nonparametric Mann–Whitney U test was used to calculate the concordance between the qPCR test and Multi-HTLV assay in 12 samples with discrepant and inconclusive qPCR results. The Multi-HTLV assay showed high performance in identifying HTLV-1 and HTLV-2 with sensitivities of 97% [95% confidence interval (CI): 0.92–0.98] and 94% (0.87–0.96), respectively. However, due to typing performance (98% for HTLV-1 and 94% for HTLV-2), it had 95% agreement with positive HTLV-1 qPCR results (95% CI: 90.07–97.81) and 86% (78.04–91.01) of HTLV-2 qPCR results were positive. Moreover, this test was able to recognize 80% of indeterminate samples and all HTLV-2 positive samples that showed false-negative qPCR results. Our findings, derived from a substantial number of HTLV-positive samples, underscore the inherent reliability and feasibility of the Multi-HTLV assay, regardless of the molecular testing facilities. Furthermore, the distinctive multiparametric nature of this assay, combined with its straightforward procedural execution, introduces novel perspectives for analyzing specific serological profiles in each patient, as well as the potential for immunological monitoring of disease progression.
Introduction
Infection with human T cell lymphotropic virus types 1 and 2 (HTLV-1/2) is present in all Brazilian regions, with a heterogeneous distribution depending on the ethnic origin of individuals and their geographic location. 1,2 Estimates indicate that in Brazil, this infection directly affects approximately 1 million people, making it the country with the highest absolute number of cases in the world. 3 Although most individuals never develop any signs or symptoms of the disease, they may develop one or more related conditions. 4 –7
HTLV-1 is associated with several clinical conditions with high morbidity and mortality, such as HTLV-1-associated myelopathy/tropical spastic paraparesis and adult T cell leukemia/lymphoma (ATLL). 4,5 HTLV-2, in contrast, is rarely associated with the development of disease. 2,8 Therefore, HTLV-1/2 viral typing and accurate diagnosis play a fundamental role in the assistance, monitoring, and guidance of those infected by this virus. 9
HTLV screening has been a mandatory public health policy in Brazil's blood banks since 1993. 10 However, it was only in 2016 that confirmatory tests were incorporated into the Unified Health System [Sistema Único de Saúde (SUS)] and only for suspected cases of ATLL. 11 The serological diagnosis of these infections is based on the detection of specific antibodies produced in response to viral proteins present in the serum or plasma. 12,13 Initially, simpler methods with high sensitivity (close to 100%) were used for screening, such as enzyme immunoassay (EIA or enzyme-linked immunosorbent assay [ELISA]) or chemiluminescence immunoassay (CLIA). 11,14,15
However, due to the low specificity presented by these tests, the use of complementary tests is recommended by the Brazilian Ministry of Health (whose specificity can vary from 98% to 100%), such as the Western blot (WB) and the line immunoassay (LIA). 11,15 Besides confirming the presence of the virus, these tests are also used to discriminate against the viral type. 15,16
However, despite the high sensitivity and specificity of complementary serological tests for HTLV infection, they have different sensitivities and can generate discordant, inconclusive, and false-negative results, especially when applied to samples from individuals with HTLV-2 and those coinfected with HIV, HBV, and HCV. 11 In these populations, the LIA sensitivity varied from 94.8% to 97.2%, whereas the WB sensitivity varied from 82.4% to 82.8%. 17 –19
For such cases, more specific molecular techniques, such as nested polymerase chain reaction (n-PCR), real-time polymerase chain reaction (qPCR), and polymerase chain reaction (PCR)-restriction fragment length polymorphism analysis (PCR-RFLP), 20 which do not have commercial protocols available, are indicated, making it difficult to implement them on a large scale or in peripheral locations.
In 2021, InfYnity Biomarkers developed and validated a new high-performance multiplex immunoassay (Multi-HTLV) to confirm and discriminate HTLV-1 and HTLV-2 strains. The Multi-HTLV showed 100% sensitivity, 98% specificity, and 100% typing accuracy in 491 HTLV-positive samples (246 HTLV-1-positive samples collected from 100 volunteers and 245 HTLV-2-positive samples from 99 volunteers), 21 making them the closest serological test technique to the effectiveness of molecular tests, considered the “gold standard” for the diagnosis of this infection. Furthermore, the multiparametric nature of this assay opens new avenues for studying patient-specific serological signatures, following the course of infection, and exploring the prognostic utility of HTLV disease. 21
Thus, due to the different sensitivity values presented by the confirmatory tests and their possible correlations with doubtful or false-negative results, the objective of this study was to evaluate the sensitivity of this new serological methodology (Multi-HTLV/InfYnity Biomarkers) as well as the accuracy of typing.
Methods
Ethical statements
This study was approved by the ethics committees of the IMTSP Deliberative Council and Instituto de Infectologia Emílio Ribas (IIER; CAAE: 86379218.6.1001.0061). All participants signed an informed consent form after they agreed to participate in the study. Samples were selected according to the clinical symptoms and qPCR techniques developed in the laboratory.
Study design
The study included stored plasma samples from subjects recruited by the IIER cohort in São Paulo, Brazil, from 1997 and stored in the repository of the Laboratory of Medical Investigation in Dermatology and Immunodeficiencies (LIM/56). This was a cross-sectional study, in which we included all 18-year-old participants who were in regular follow-up for >20 years. Enrollment in the cohort was performed after screening by ELISA with HTLV viral lysate (Gold ELISA HTLV-I+II®; REM), followed by confirmation by WB (HTLV Blot 2.4®; MP Biomedicals) and molecular assays (qPCR and PCR-RFLP).
Owing to the difference in storage time, samples collected between 2018 and 2022 were selected. Thus, 246 HTLV-positive samples were eligible for this study: 127 positive for HTLV-1, 112 positive for HTLV-2, and 7 coinfected for both types (HTLV-1 and HTLV-2), previously identified by qPCR.
To evaluate the accuracy and typing of Multi-HTLV serology under extreme conditions, 12 samples with discrepant qPCR results (false-negative or doubtful) were selected. These samples were preliminarily characterized by PCR-RFLP analysis (Table 1).
Discrepant Samples
F, female; FN, false-negative; HTLV-1, human T cell lymphotropic virus type 1; HTLV-2, human T cell lymphotropic virus type 2; M, male; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism analysis; POS, positive; qPCR, real-time polymerase chain reaction.
Molecular assays
The qPCR analysis was performed as described by Gonçalves et al. (2019), who obtained 97% sensitivity and 100% specificity in their study. In brief, after DNA patterning, qPCR was performed using the hydrolysis probe system for two target sequences: a pol region of the proviral genome of HTLV-1 and another of HTLV-2. The albumin gene was used to control the quality and presence of genomic DNA. For samples from individuals under follow-up who presented doubtful (different results in their duplicates and/or serology) and false-negatives results, PCR followed by PCR-RFLP targeting specific regions of the env was performed as described by Novoa et al. 22
Novel multiplex HTLV immunoassay: Multi-HTLV assays
The model designed and developed by InfYnity Biomarkers (Lyon, France) is based on 14 individually selected HTLV antigens and printed (in duplicate) for each well of a Maxisorp Nunc 96-well plate using the SciFLEXARRAYER printing system (SCIENION). 21 In addition, using the piezoelectric impulse-based printing process, which allows for the printing of antigens in precise X-Y coordinates, three positive control points (PC), designed to check for the presence of human samples and enzyme conjugates, were added (Fig. 1).
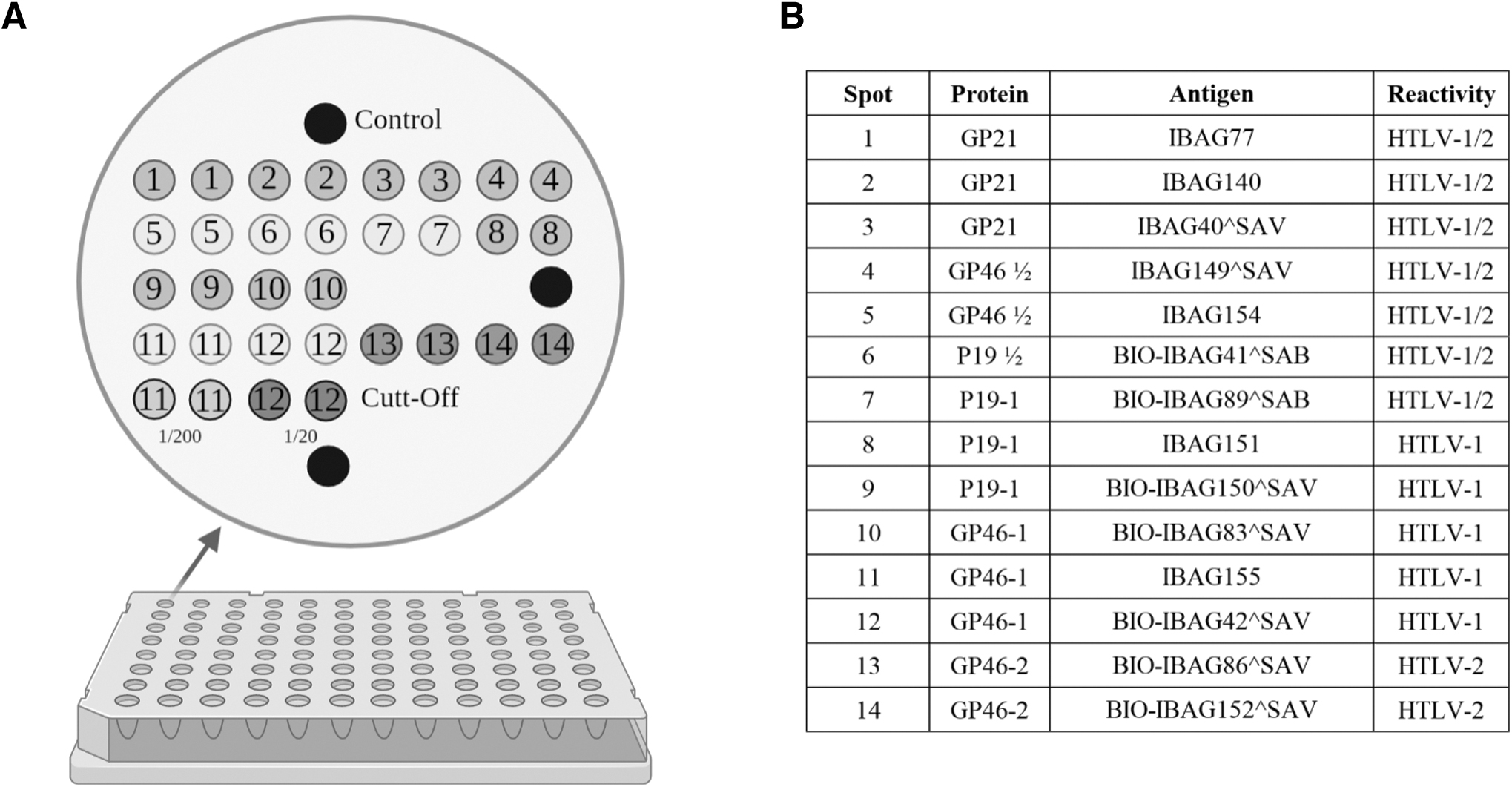
Multi-HTLV antigens map.
The Multi-HTLV assay is performed similarly to the ELISA EIA, allowing the simultaneous detection of circulating antibodies against a set of selected and validated antigens. 21 Initially, the microplates were incubated with plasma from the samples from the repository diluted at a concentration of 1:50 in PBS-T (0.05%, pH 7.5) and bovine serum albumin (BSA; 1%) for 1 h at room temperature. After three washing steps with PBS-T, 100 μL of antihuman IgG secondary antibody conjugated to horseradish peroxidase, diluted in PBS-T (0.05%, pH 7.5) and BSA buffer (1%) at a concentration of 1:2,000, was added to each well, and the microplate incubated for 1 h at room temperature.
To remove unbound secondary antibodies, the microplate was washed again three times with PBS-T, and the precipitating substrate solution (tetramethylbenzidine) was added in a darkroom for 20 min at room temperature. Finally, the reaction was stopped by carefully removing the substrate solution and drying the microplate at 37°C for 10 min. Each plate was read and analyzed using the SciReader CL (SCIENION), which acquires high-resolution digital images and integrated software and calculates the pixel intensity for each spot.
Calculations were performed using the mean value of duplicate points based on the available cutoff values. All data were analyzed using an interpretation algorithm provided by InfYnity Biomarkers S.A.S. This algorithm consists of a logistic regression calculation developed based on the serological profiles of well-characterized serum samples analyzed during the test development and validation stages. 21
Statistical analysis
After applying the interpretation algorithm, sensitivity (number of positive values for Multi-HTLV divided by the number of qPCR-positive samples), and utilizing the corresponding 95% confidence interval (CI), were used to assess the diagnostic accuracy and performance of the Multi-HTLV assay. Hereafter, to calculate the concordance between Multi-HTLV and qPCR, descriptive statistics presented as frequencies were used for categorical variables with a 95% CI, according to Wilson/Brown method. To correlate the discrepant qPCR results with Multi-HTLV, the nonparametric Mann–Whitney test was used. All statistical tests were performed using GraphPad Prism, version 8.0.2.
Results
Multi-HTLV sensitivity and typing accuracy
Multi-HTLV sensitivity was calculated based on the concordance of positivity with qPCR results according to our protocol (regardless of typing). In this part of the analysis, the indeterminate samples were considered negative. Thus, we obtained a sensitivity of 97% (95% CI: 92.18–98.77; n = 123/127) for HTLV-1 and 94% (87.66–96.94; n = 105/112) for HTLV-2. In this step, the sensitivity for samples positive for both types (HTLV-1 and HTLV-2) was not calculated because of the low discrimination of the test (Table 2).
Analysis of the Multi-HTLV Sensitivity
Results are expressed as number of samples.
n, Number of samples.
Typing performance showed a specificity of 98% (94.26–99.71; n = 121/123 typed correctly) for the set of HTLV-1 seropositive samples and 91% (84.51–95.43; n = 96/105) for HTLV-2 seropositive samples. However, for the samples of individuals who were coinfected (HTLV-1 and HTLV-2), Multi-HTLV failed to correctly validate any sample. In this part of the analysis, only positive results were used for both tests, and the ratio was calculated based on perfect agreement between the results (Table 3).
Analysis of the Multi-HTLV Typing Accuracy
Results are expressed as number of samples. The table shows only a comparison of the positive results for both tests.
n, number of samples.
Concordance between PCR-positive results and the Multi-HTLV
Of the 127 samples positive for HTLV-1 by qPCR, 121 of 127 samples (95% with 95% CI: 90.08–97.82) showed concordant validation during the Multi-HTLV assay. Although ∼5% showed nonconcordant results, 2 of 127 samples (2%, 0.28–5.56) showed positive validation, but with discordant typing; 3 of 127 (2%, 0.64–6.72) samples had indeterminate results; and 1 of 127 (1%, 0.04–4.33) samples had a false-negative result.
When comparing the positive results for HTLV-2 between qPCR and Multi-HTLV, we found a lower concordance compared with the positive results for HTLV-1. In this group, Multi-HTLV obtained only 96 of 112 (86%; 78.05–91.01) of results in perfect concordance with qPCR. Although 9 of 112 (8%, 4.29–14.57) of these samples presented positive validations, but with discordant typing, 5 of 112 (4%, 1.92–10.03) samples presented indeterminate results and 2 of 112 (2%, 0.32–6.28) samples had false-negative results.
In the seven samples positive for HTLV-1 and HTLV-2, Multi-HTLV did not agree with any of the qPCR results. Of them, four of seven (57%, 25.05–84.18) samples showed reactivity for HTLV-1, two of seven (29%, 5.08–64.11) samples showed reactivity for HTLV-2, and one of seven (14%, 0.73–51.31) samples had an indeterminate result (Fig. 2).

Flowchart comparing the results between qPCR and Multi-HTLV methods. ELISA, enzyme-linked immunosorbent assay; FN, false-negative; Ind, indeterminate; Multi-HTLV, Multiplex-ELISA/Infynity Biomarkers; qPCR, real-time polymerase chain reaction.
Correlation between qPCR results and the Multi-HTLV in discrepant samples
To evaluate the performance of Multi-HTLV under atypical conditions, four samples that showed doubtful results during qPCR and seven samples that obtained false-negative results were tested. Antigen intensities were significantly higher in positive qPCR samples than in false-negative qPCR or false-negative qPCR plus doubtful qPCR (p = .0024 “positive samples” Fig. 3A and
p
= .0104 “positive samples” Fig. 3B). Correlation between qPCR results and the Multi-HTLV in discrepant samples. 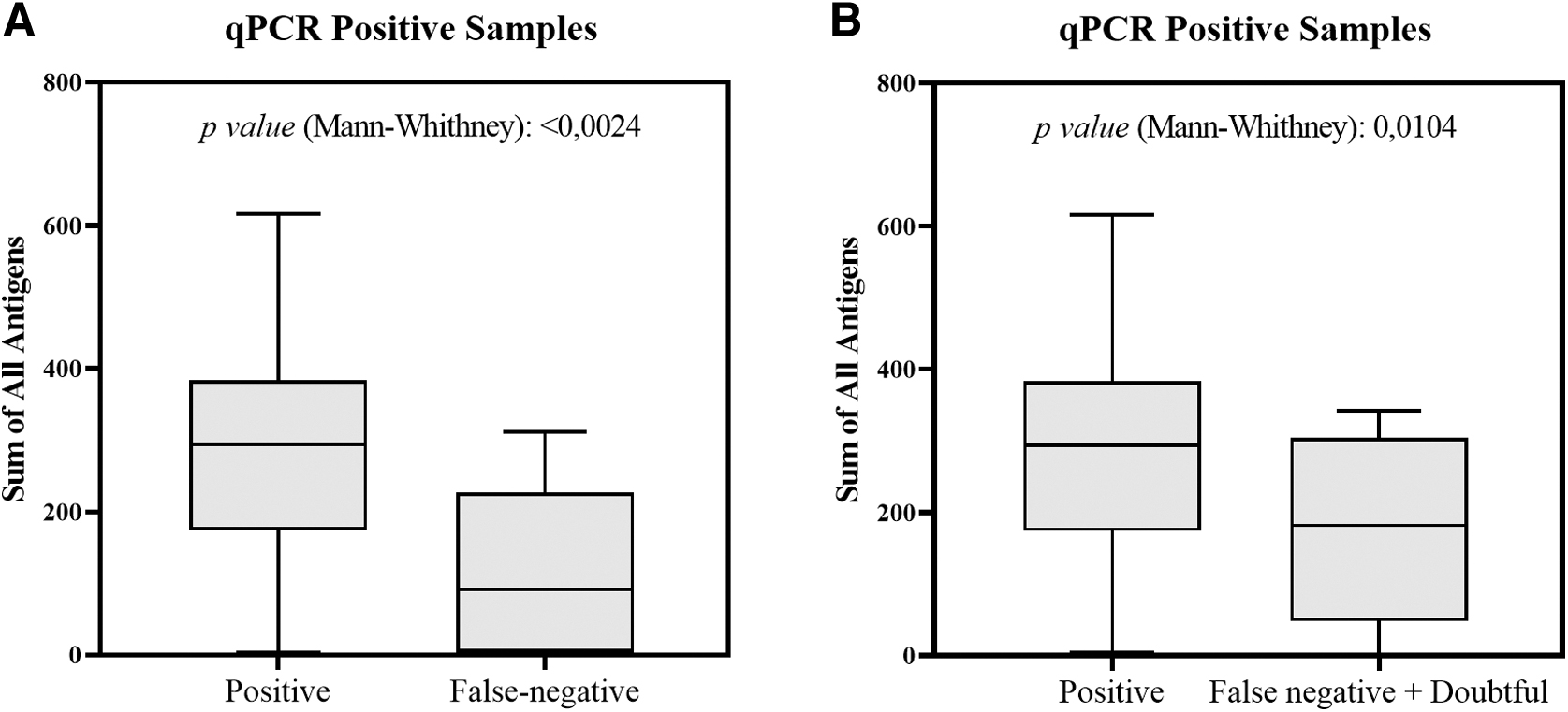
Even samples with false-negative or doubtful qPCR results demonstrated a significant decrease in the mean intensity of Multi-HTLV antigens. The Multi-HTLV was able to correctly identify four of five samples with doubtful results (80%, 37.55–98.97): two of two samples positive for HTLV-1 (40%, 7.11–76.93); two of three (40%, 76.93–7.11) samples positive for HTLV-2, whereas only one sample of this group remained indeterminate, in concordance with qPCR (20%, 1.03–62.45). In addition, this test correctly identified four of seven samples with false-negative qPCR results group (57%, 25.05–84.18).
All identified samples were positive for HTLV-2. However, the HTLV-1 positive samples from this group were not validated correctly: two of seven (29%, 5.08–64.11) samples showed concordant results with the molecular technique (false negative) and one of seven (14%, 0.73–51.31) samples had an indeterminate result (Fig. 4).
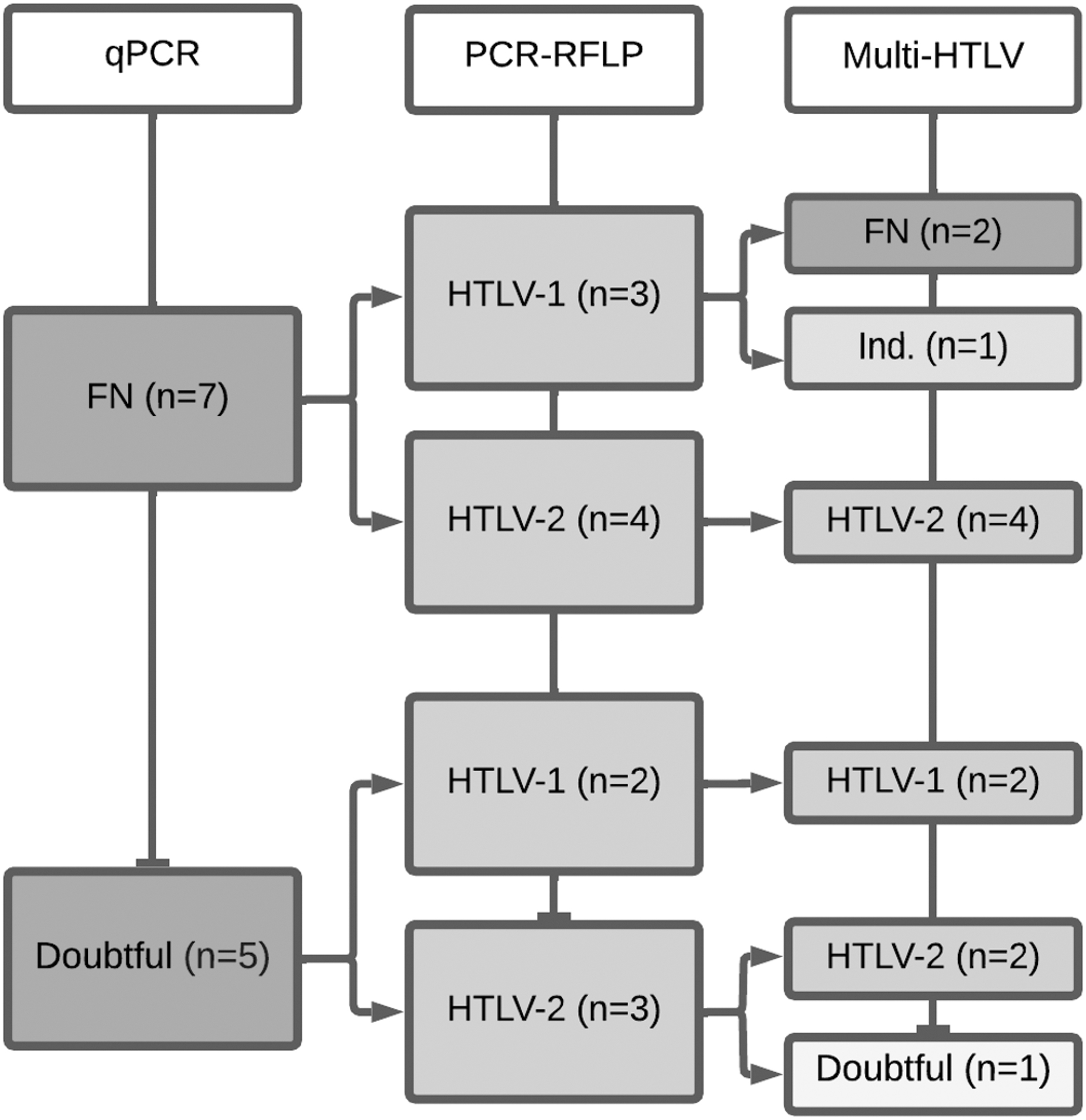
Comparative flowchart between FN and doubtful qPCR/PCR-RFLP and Multi-HTLV results. Comparative flowchart of FN and doubtful qPCR/PCR-RFLP and Multi-HTLV results. PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism.
Discussion
We evaluated a new innovative high-performance Multi-HTLV assay that has the potential to address the key limitations associated with confirmatory serological testing for HTLV. In addition, this test aims to monitor different serological profiles according to each patient, either by an initial visual analysis or later by a high-precision customized algorithm that guarantees more reliable confirmation and typing results. 21 However, this study had two main limitations: the first is associated with the long storage period of the samples, and the second is the lack of data regarding possible associated coinfections. Although the samples were characterized by in-house qPCR, another limitation was related to the lack of comparative serological methods to document the samples.
Improved diagnostic tests that lead to better identification of an infection in patients or blood donors play a fundamental role in public health, helping create strategies to fight infectious diseases. Furthermore, they are effective when used for early identification of the infection, consequently enabling better care and monitoring of those infected. 23 However, in the 30 years since the development of the LIA, no significant progress has been made in improving the effectiveness of the tests currently used for HTLV-2. 15,23
Our findings from a significant number of positive samples demonstrate that the Multi-HTLV technique has a sensitivity of 97% for HTLV-1, slightly higher than that found by Umeki et al., using the LIA test, and the results commonly found by WB in this group of individuals. 11,18,19,24 In addition, the 94% sensitivity shown by Multi-HTLV in seropositive samples for HTLV-2 was similar to the sensitivity of LIA, which can vary from 94% to 97%, and highly superior to that of WB, which reaches ∼82% in this group of individuals. 11,18,19
Whereas the focus of this study was not on the specificity of the test itself, but rather on its accuracy in typing and comparison with molecular tests. Preliminary studies, conducted by our group and subsequently published, revealed an accuracy rate close to 98%. This rate is superior to both WB and Immunoassay Luminex Assay (LIA), as observed in a large sample size. 11,17,18
It is worth mentioning that due to the typing accuracy presented by Multi-HTLV in this study (98% for HTLV-1 and 91% for HTLV-2), the perfect concordance between its results and qPCR technique ranged from 95% for HTLV-1-positive samples to 86% for HTLV-2-positive samples. As to validation, 2% and 8% of the samples from these groups, respectively, yielded positive validation, but with discordant typing. Although the accuracy values calculated here demonstrate a negative effect on the performance of this immunoassay, when WB and LIA are compared with the same molecular techniques, they present similar or even lower typing than Multi-HTLV. 17 –19
These results demonstrate that the Multi-HTLV technique represents a great advance in the reduction of false-negative, discrepant, or inconclusive results in positive samples. Furthermore, the new profiles found in this study can be added to diagnostic algorithms to decrease these inconsistencies and further increase the accuracy of this test. 21
From many points of view, HTLV-2 is more stable than HTLV-1 or other RNA viruses. 25 Studies indicate that this typing difficulty, or even false-negative serology, is directly related to the low number of viral copies added to the long persistence of the characteristic latency of this virus, leading to low antibody stimulation and the gradual decline of specific antibodies. 26,27 However, the use of serology for the diagnosis of this infection is still recurrent, as most molecular assays have been developed internally and do not have commercial protocols available or validated by the National Health Surveillance Agency (ANVISA), which makes it difficult to implement a decentralized method or suitability to the usual diagnostic algorithm. 20
The molecular qPCR technique performed in this study showed better accuracy for the diagnosis of HTLV-1/2 compared with Multi-HTLV, especially in rare individuals who are coinfected with HTLV-1 and HTLV-2. However, the multiparametric nature of this assay, together with its ease of execution and cost, opens new avenues for studying the specific serological signatures of each patient and monitoring disease evolution. In addition, this tool showed a high level of competitiveness among other confirmatory serological techniques available on the market, and can be used as an alternative, especially in cases with discrepant results.
Approximately 80% of samples with doubtful qPCR results were correctly diagnosed using this methodology. Furthermore, all HTLV-2-positive samples with false-negative results during qPCR were correctly identified by Multi-HTLV. However, it is worth mentioning that due to the low representativeness of the discrepant samples included in this study, better analyses in more significant groups may prove essential for improving the effectiveness of this test.
Conclusions
The data from our study showed that the Multi-HTLV assay is reliable, easy to perform, and can be used in locations without infrastructure for molecular testing. This assay is a potential alternative that fills the gap generated by samples with discrepant results in molecular assays, as well as open new avenues to study the specific serological signatures of each patient and follow the evolution of the disease. In addition, it will enable early treatment, better assistance from health services, and better quality of life for those infected with HTLV-1.
Footnotes
Acknowledgments
We are immensely grateful to all patients who agreed to participate in the study, to the support of this research by the Coordination for the Improvement of Higher Education Personnel (CAPES) scholarship, and the Faculty of Medicine of the University of São Paulo.
Authors' Contributions
V.Â.F. contributed to writing original draft, methodology, review, and editing. S.V.K. was involved in writing original draft, review, and editing. F.D.S. carried out methodology and editing. P.D.L.J. took charge of methodology and editing. M.E.J.H. and A.C.P.O. were involved in methodology and review. J.S. carried out methodology and editing. M.Z. and F.S. carried out review and editing. J.C. was in charge of supervision, writing conceptualization, review, and editing.
Author Disclosure Statement
The authors M.Z. and F.S. are employed by InfYnity Biomarkers; however, this does not impact their adherence to a strict scientific code of ethics in conducting this study. Furthermore, the remaining authors declare that they have no affiliations or involvement with any organization or entity with a financial interest in the subject matter or materials discussed in this article. It is important to note that this study did not receive and will not receive any support or funding from InfYnity Biomarkers.
Funding Information
This study was supported by São Paulo Research Foundation (No. 2016/03025-2); scholarship to V.A.F. by CAPES (No. 33002010060P2) and Foundation of Faculty of Medicine of the University of São Paulo.