
Abstract
Integrase strand-transfer inhibitors (INSTIs) are associated with weight gain in women living with HIV (WLH). Relationships between drug exposure, baseline obesity, and INSTI-associated weight gain remain unclear. Data from 2006 to 2016 were analyzed from virally suppressed WLH enrolled in the Women's Interagency HIV Study, who switched/added an INSTI to antiretroviral therapy: [raltegravir (RAL), dolutegravir (DTG), or elvitegravir (EVG)]. Percent body weight change was calculated from weights obtained a median 6 months pre-INSTI and 14 months post-INSTI initiation. Hair concentrations were measured with validated liquid chromatography-mass spectrometry (MS)/MS assays. Baseline (preswitch) weight status evaluated obese (body mass index, BMI, ≥30 kg/m2) versus nonobese (BMI <30 kg/m2). Mixed models examined the drug hair concentration*baseline obesity status interaction for each INSTI. There were 169 WLH included: 53 (31%) switched to RAL, 72 (43%) to DTG, and 44 (26%) to EVG. Women were median age 47–52 years, predominantly Non-Hispanic Black, median CD4 counts >500 cells/mm3, >75% with undetectable HIV-1 RNA. Over ∼1 year, women experienced median increases in body weight: 1.71% (−1.78, 5.00) with RAL; 2.40% (−2.82, 6.50) with EVG; and 2.48% (−3.60, 7.88) with DTG. Baseline obesity status modified the relationship between hair concentrations and percent weight change for DTG and RAL (p's < 0.05): higher DTG, yet lower RAL concentrations were associated with greater weight gain among nonobese women. Additional pharmacologic assessments are needed to understand the role of drug exposure in INSTI-associated weight gain.
Background
Integrase strand-transfer inhibitors (INSTIs) are the mainstay of antiretroviral treatment (ART) for people with HIV (PWH). 1,2 INSTI use has been associated with body weight gain, particularly among women living with HIV (WLH), 3 –7 a group heavily impacted by the global AIDS epidemic, 8 but underrepresented in HIV research. 9 Among virologically suppressed PWH, body weight gain and obesity have been linked to diabetes mellitus, cognitive impairment, 10 and a 1.5-fold increased odds of ART nonadherence. 11
Demographic and clinical characteristics associated with INSTI-associated weight gain, including female sex, 4,7,12 older age, 4,13 and lower baseline body mass index (BMI), 13,14 also play prominent roles in drug pharmacokinetics. 15 –18 However, the role of ART pharmacokinetics in INSTI-associated weight gain remains unclear. Higher plasma concentrations of efavirenz and dolutegravir (DTG) have been associated with neuropsychiatric side effects, 19 –21 while higher atazanavir concentrations have been associated with hyperbilirubinemia 22 and metabolic and renal disorders. 23 However, plasma concentrations represent recent drug exposure and are influenced by short-term adherence changes. 24 Hair concentrations are measures of long-term ART adherence and strong predictors of virological outcomes. 25 –27 Higher hair concentrations of tenofovir and emtricitabine in the setting of HIV-1 pre-exposure prophylaxis were associated with creatinine clearance decline, 28 illustrating the utility of hair concentrations to predict toxicities.
Leveraging the Women's Interagency HIV Study (WIHS) cohort, we showed that WLH switching to or adding an INSTI [DTG, elvitegravir (EVG), or raltegravir (RAL)] to ART experienced significantly greater gain in body weight and other adiposity measures compared to women remaining on non-INSTI regimens, and the magnitude was greater in nonobese women (BMI <30 kg/m2). 13 In this analysis, we assessed the association between INSTI hair concentrations and body weight change in WLH and the potentially modifying effects of baseline obesity status.
Methodology
Study population
The study population consisted of WLH enrolled in WIHS, 29,30 a longitudinal cohort of WLH and at-risk HIV-seronegative cis-gender women from 10 U.S. sites: San Francisco, CA; Los Angeles, CA; Chicago, IL; Brooklyn, NY; Bronx, NY; Washington, DC; Chapel Hill, NC; Miami, FL; Birmingham, AL/Jackson, MS combined site; and Atlanta, GA. WIHS participants underwent semiannual study visits with clinical and medication histories, physical examinations, and specimen collection. Hair specimens were collected at each semiannual visit by uniformly trained research staff from participants who reported ART use for ≥1 month.
Eligibility criteria included WLH with self-reported ART use at five consecutive semiannual study visits who (1) switched from non-INSTI ART [defined as regimens, including a nucleoside reverse transcriptase inhibitor backbone plus non-nucleoside reverse transcriptase inhibitor (NNRTI), protease inhibitor, and/or entry inhibitors] to regimens, including an INSTI (DTG, RAL, or EVG), or added an INSTI to existing ART; (2) remained on same INSTI drug for ≥ two study visits; (3) were not pregnant; (4) had HIV-1 RNA <200 copies/mL at each of these visits; and (5) had hair collected in ≥1 postswitch/add visit. Since advanced disease stage (low CD4 count and high HIV-1 RNA viral loads) has been strongly associated with weight gain after ART initiation, 10,31 we excluded ART-naive women. The WIHS study protocol was approved by Institutional Review Boards at each site; only de-identified data were used.
Definitions of outcome and covariates
Sociodemographic and clinical data collected from WIHS visits occurring from 2006 to 2016 were used. The study visit at which INSTI use was first reported was considered the “switch/add” visit. Each participant contributed data from ≥2 study visits: one visit occurring a median of 6 (Q1: 5, Q3: 6) months preceding the switch/add visit (baseline) and ≥1 study visit occurring median 14 (12, 18) months after the switch/add visit (postswitch/add). At each visit, body weight (kilogram, kg) and height (meters, m) were measured using standard methods. 32 The primary outcome was percent body weight change [(postswitch/add minus baseline)/baseline × 100)] between visits.
BMI was calculated as weight (kg)/height (m). 2 Baseline obesity status, the modifier of interest, was defined as obese (BMI ≥30 kg/m2) versus nonobese (BMI <30 kg/m2) based on World Health Organization guidelines. 33 We selected additional covariates based on previous literature that suggested they were important confounders on the relationship between weight gain, ART pharmacokinetics, and/or hair drug concentrations, 4,7,12 –18,34,35 including age, race/ethnicity (Non-Hispanic Black vs. all other races/ethnicities), current smoking (yes/no), education attained (>high school diploma vs. less), annual income (0–$12,000, $12,001–$24,000, or >$24,000), NNRTI exposure at baseline (yes/no), HIV-1 viral load (undetectable vs. detectable, but <200 copies/mL), estimated glomerular filtration rate (eGFR) in mL/min using the chronic kidney disease epidemiologic collaboration, Chronic Kidney Disease Epidemiologic Collaboration, equation, 36 and self-reported hair bleaching.
Self-reported ART adherence was assessed in questionnaires where participants were asked how often over the last 6 months, they took their antiretroviral therapy as prescribed (summarized as ≥95% vs. <95%). No woman reported use of tenofovir alafenamide (TAF) containing ART.
Hair collection, processing, and analysis
INSTI use was first reported in WIHS in 2007; therefore, hair collected between 2007 and 2016 was used in these analyses. Collection procedures were standardized: ∼10–20 strands of hair from the occipital region were cut close to the scalp with the distal region labeled to denote directionality. Hair was stored in foil within a plastic bag containing a dessicant at room temperature until analysis. 37 To keep the time period consistent between participants, one centimeter portions of hair most proximal to the head (reflecting ∼1 month of growth) were analyzed for INSTI concentrations.
The University of North Carolina School of Pharmacy Clinical Pharmacology and Analytical Chemistry Laboratory, accredited by the College of American Pathologists (CAP) and Clinical Laboratory Improvement Amendments (CLIA), participates in the Clinical Pharmacoloogy Quality Assurance program and performed all hair analyses. Analytical methods for the measurement of hair DTG and RAL have been previously published by our group. 38,39 EVG hair concentrations were determined by a validated liquid chromatography-mass spectrometry method with stable isotopically labeled EVG-d6 as the internal standard. EVG was extracted from hair strands by sonication and incubation in methanol with 2% formic acid.
Following extraction, chromatographic separation was achieved under gradient conditions on a Waters Atlantis T3 (50 × 2.1 mm, 3 mm) analytical column. Compounds were detected on an AB Sciex API-5000 triple quadrupole mass spectrometer with electrospray ionization in positive ion mode. Calibration ranges were 5–10,000 pg/mL for DTG, 0.1–100 ng/mL for RAL, and 0.05–10 ng/mL for EVG. Hair concentrations below the limit of detection were input as lower limit of detection/2. Precision and accuracy criteria of 15% were met for calibration standards and quality control samples for all three assays.
Statistical analyses
Analyses were stratified by INSTI (DTG, RAL, and EVG) use. Demographic and clinical characteristics were summarized with counts (and percents) and medians (Q1, Q3) for categorical and continuous variables, respectively. For each INSTI, unadjusted linear regression models were created with compound symmetry covariance matrix for repeated measures. The dependent variable was percent body weight change from baseline, and independent variables included INSTI hair concentration, baseline obesity status, and INSTI hair concentration*obesity status. The interaction term with obesity status was decided a priori based on earlier work that suggested baseline BMI as an important modifier of INSTI exposure on weight change outcomes. 13 Additional covariates in our adjusted models included undetectable HIV-1 viral load, time since baseline, baseline: smoking status, NNRTI use, education level, race/ethnicity, income, age, and eGFR. Analyses were performed using SAS v9.4 software (Cary, NC) with alpha = 0.05. Model fit was assessed by residual plots.
Results
Demographic and clinical characteristics
One hundred sixty-nine WLH met eligibility criteria: 53 (31%) had switched to RAL, 72 (43%) to DTG, and 44 (26%) to EVG. Women were middle aged (median age range 47.0–51.5 years) and predominantly Non-Hispanic Black, and majority with education levels at or below high school diploma and annual incomes below $12,000. Overall, median CD4 lymphocyte counts were >500 cells/mm3, over three-quarters had undetectable HIV-1 RNA (<80 copies/mL), median time on ART was almost a decade, and over 80% reported ≥95% ART adherence. No woman reported use of hair bleach during the study. Baseline prevalence of obesity was high, ranging from 34% in the RAL group to 61% in the EVG group, Table 1.
Baseline Clinical and Demographic Characteristics Stratified by Integrase Strand-Transfer Inhibitor Drug
Limit of detection for HIV RNA viral load was 80 cop/mL. ART adherence was self-reported adherence of taking HIV medications as prescribed over the last 6 months, summarized as ≥95% versus <95%. Column percents may not total 100 due to rounding.
ART, antiretroviral therapy; BMI, body mass index; DTG, dolutegravir; eGFR, estimated glomerular filtration rate, calculated by Chronic Kidney Disease Epidemiologic Collaboration (CKD−EPI) equation; EVG, elvitegravir; INSTI, integrase strand-transfer inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; Q1, first quartile; Q3, third quartile; RAL, raltegravir.
Association between INSTI hair concentrations and body weight gain
Women experienced a median (Q1, Q3) +1.71% (−1.68, 4.96) increase in body weight with RAL, 2.40% (−2.82, 6.50) increase with EVG, and 2.48% (−3.60, 7.88) increase with DTG after a median 1.13, 1.09, and 1.24 years, respectively.
In multivariable-adjusted linear models for DTG, there was a significant interaction between obesity status and DTG hair concentrations (p = .0320). Higher DTG hair concentrations were positively associated with body weight gain in nonobese women and inversely associated with body weight gain in obese women, Figure 1a. Among nonobese women, those with DTG hair concentrations in the highest quartile experienced greater body weight gain than those with hair concentrations in the lowest quartile: +6.3% versus +3.4%, p = .0728. In obese women, there was no significant difference in body weight change between those with DTG hair concentrations in the highest versus lowest quartile: +1.1% versus +3.6%, p = .1888.
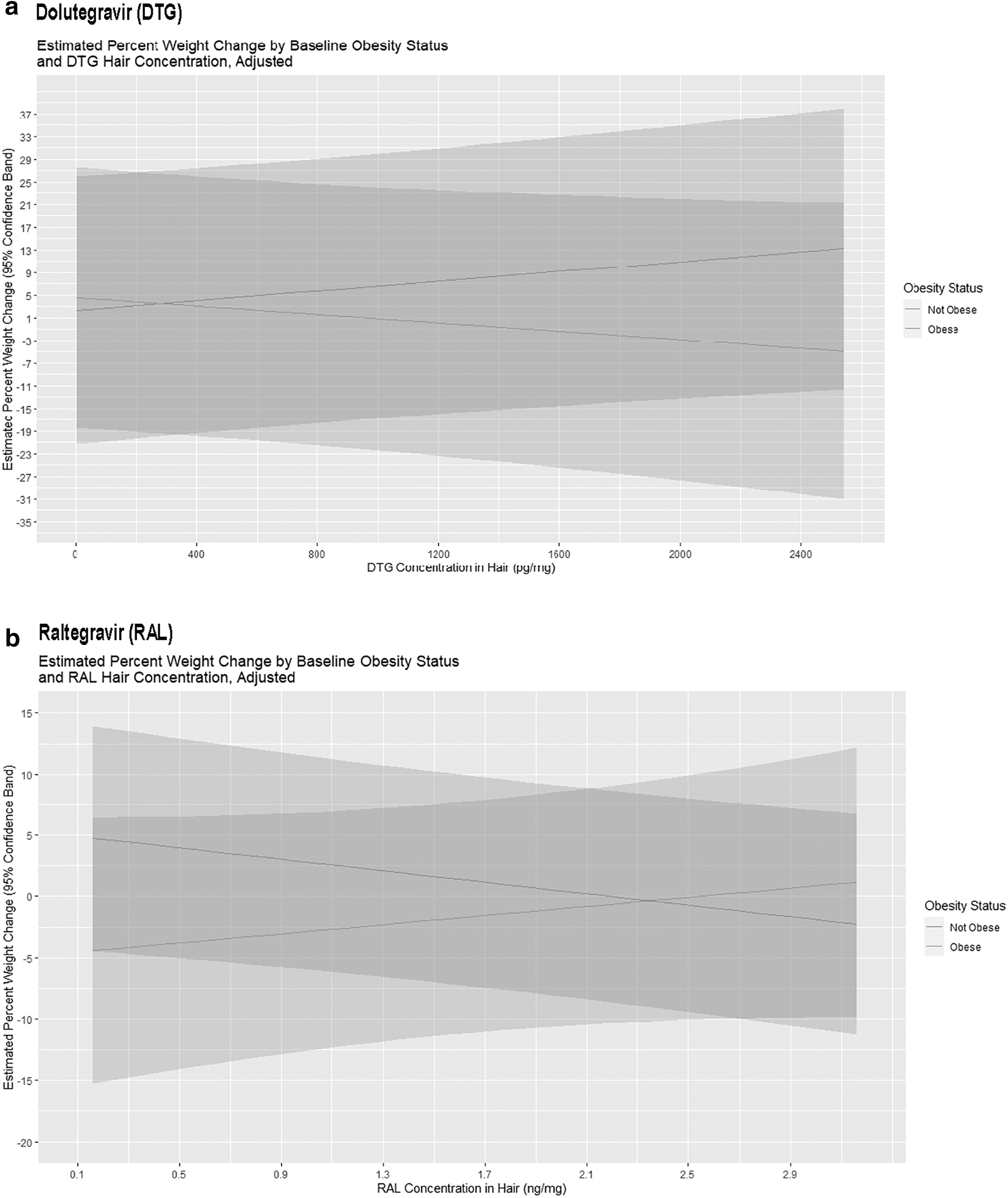
Estimated percent body weight change by baseline obesity status and INSTI hair concentration. Model-adjusted estimates of percent body weight change (y-axis) by baseline obesity status (grey line = nonobese; light grey line = obese) and INSTI hair concentration (x-axis). Models were adjusted for baseline: age, race/ethnicity, education, income, smoking status, non-nucleoside reverse transcriptase use, eGFR, undetectable HIV viral load, and time since baseline and were created separately for
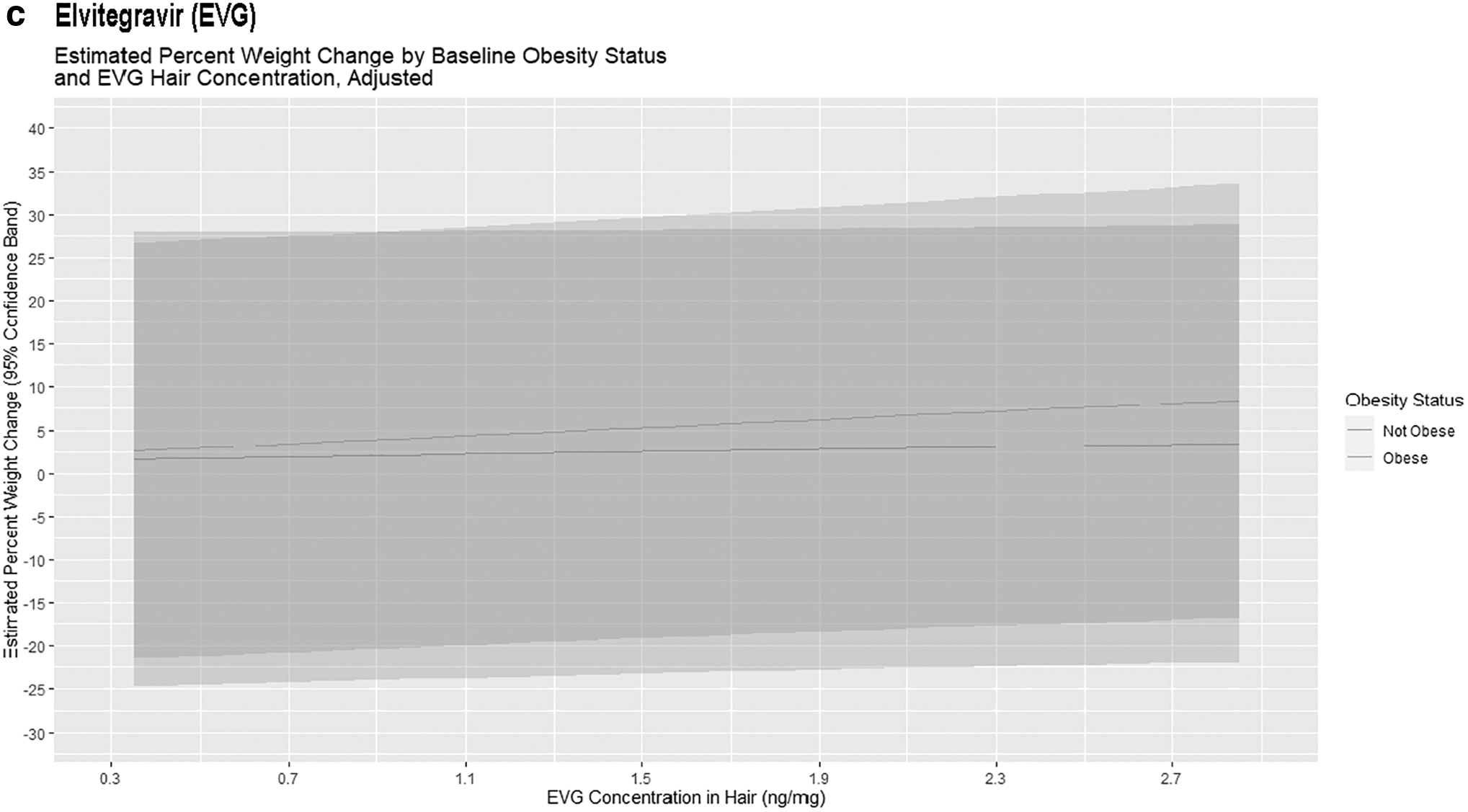
Significant interactions between obesity status and RAL hair concentrations were observed (p = .0401), but with opposite directionality: higher RAL hair concentrations were inversely associated with body weight gain in nonobese women, Figure 1b. Among nonobese women, those with RAL hair concentrations in the highest quartile experienced less body weight gain than those with hair concentrations in the lowest quartile: +1.6% versus +4.0%, p = .0222. Among obese women, there was no difference in body weight change between those with RAL hair concentrations in the highest versus lowest quartile: −1.9% versus −3.8%, p = .3113. No association was found between EVG hair concentrations and body weight change in either obese or nonobese women, Figure 1c.
Discussion
This study evaluated the relationship between body weight gain and INSTI drug exposure as measured by hair concentrations. In a diverse cohort of WLH who switched to INSTI-based ART, we found that obesity modified the relationship between INSTI drug exposure and body weight gain for DTG and RAL, but not for EVG. Furthermore, we found that body weight gain was associated with higher DTG hair concentrations, but lower RAL hair concentrations in nonobese women.
In pharmacokinetic studies, obesity has been associated with lower drug plasma concentrations for both RAL and DTG, but not for EVG. While a population pharmacokinetic study found no significant pharmacokinetic variability by body weight for EVG or its co-administered booster, cobicistat, 40 Madelain et al. found that median RAL trough concentrations (C12) were 44% lower for obese than nonobese populations, 17 and Zhang et al. found that female sex and lower body weight were associated with higher plasma DTG concentrations, either through effects on clearance or bioavailability. 41
To date, these weight-based differences in plasma drug exposure for RAL and DTG were not deemed to be clinically significant, as the primary outcome of interest was immuno-virologic response rather than side effects or toxicity. Nonetheless, our findings raise the possibility that higher DTG drug exposure could contribute to body weight gain, particularly in women with lower body weight before DTG initiation, and reintroduce the question of whether weight-based or sex-specific dosing for some ART may be warranted if the therapeutic window is high.
Mechanisms to explain INSTI-associated weight gain remain unclear, and theories currently include proadipogenic effects promoting mitochondrial dysfunction and insulin resistance, interference with the melanocortin signaling system resulting in appetite stimulation, as well as indirect effects from preswitch anchor drugs such as efavirenz that suppress weight. 42 The gut-brain axis, a complex system of peripheral appetite hormones and centrally mediated neuronal regulation, is critical to body weight homeostasis and often perturbed in obese individuals. 43
We were surprised to find that higher DTG concentrations, but lower RAL concentrations were associated with body weight gain in nonobese women. While the mechanisms driving body weight gain remain unknown, they could include INSTI-specific concentration-dependent effects on metabolic rate, adipocyte function, or appetite stimulation. 44 For example, higher RAL concentrations could be associated with appetite suppression or increased metabolic rate, which could explain the inverse relationship we see between RAL drug concentrations and body weight gain. While available sociodemographic and clinical characteristics of women switching to RAL and DTG were similar, it is also possible that there were unmeasured confounders, given the observational study design.
Our study has several strengths, including the analysis of data from a large well-characterized interval longitudinal cohort with standardized data and specimen collection and the use of hair ART concentrations, a robust measure of adherence and drug exposure. 26,28,37 However, our sample size was relatively small and consisted only of U.S. women; therefore, results may not be generalizable to men or the global population of WLH. Due to the time period in which this study was conducted, newer INSTIs such as bictegravir and cabotegravir were not assessed. Finally, while we did not measure hair concentrations of other drugs that women may have been taking, none of the women in our cohort reported TAF use, which limits potential confounding of the relationship between drug exposure and body weight gain.
To conclude, we found that obesity modifies the relationship between drug exposure and body weight gain for RAL and DTG in WLH. Additional larger pharmacokinetic studies of these and other INSTIs are necessary, particularly in women, to inform dosing strategies that maximize efficacy, while minimizing side effects and toxicity.
Footnotes
Authors' Contributions
C.D.L.: conceptualization, methodology, writing-original draft, visualization, supervision, and project administration; C.C.M.: methodology, formal analysis, data curation, writing-review and editing, and visualization; C.S.: investigation, resources, and writing-review and editing; S.D.W., F.P., J.E.L., J.W.M., D.G., A.L.F., A.A.A., D.K.-P., A.S., H.B., S.G.K., L.H.R., J.A.A., E.T.G., and I.O.: investigation and writing-review and editing; A.N.S.: conceptualization, methodology, writing-review and editing, and project administration.
Disclaimer
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH).
Author Disclosure Statement
C.D.L. has received funds from Theratechnologies, Inc., for consulting and as an advisory board member and institutional funds from Merck for research. A.A.A. has received personal funds from Merck and Gilead for consulting and institutional funding from Merck and Gilead for research.
Funding Information
This work was supported by the NIH/National Institute of Allergy and Infectious Diseases (NIAID) K23 AI124913 award to C.D.L. and NIH/National Institute of Mental Health (NIMH) R01 MH095683 to S.D.W. The Office of AIDS Research and NIH/National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) R01 DK125246 also supported this work (to C.D.L., C.C.M., J.A.A., and A.N.S.). Data in this article were collected by the WIHS, now the MACS/WIHS Combined Cohort Study (MWCCS). MWCCS (Principal Investigators): Atlanta CRS (I.O., A.N.S., and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos and A.S.), U01-HL146204; Brooklyn CRS (D.G. and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D'Souza, Stephen Gange and E.T.G.), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen and A.L.F.), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky), U01-HL146240; Connie Wofsy Women's HIV Study, Northern California CRS (Bradley Aouizerat and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels), U01-HL146333; Metropolitan Washington CRS (S.G.K. and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf and D.K.-P.), U01-HL146192; and UNC CRS (A.A.A.), U01-HL146194.
The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Human Genome Research Institute (NHGRI), National Institute on Aging (NIA), National Institute of Dental & Craniofacial Research (NIDCR), NIAID, National Institute of Neurological Disorders And Stroke (NINDS), NIMH, National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), and National Institute on Deafness and Other Communication Disorders (NIDCD), NIDDK. MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), P30-AI-050409 (Atlanta CFAR), P30-AI-050410 (UNC CFAR), and P30-AI-027767 (UAB CFAR).