
Abstract
The distribution of human immunodeficiency virus-1 (HIV-1) subtypes indicates difference from region to region and in risk groups acquiring the disease worldwide. Although subtype C is more in terms of total cases, subtype B is dominant in certain regions, especially in western and central Europe. Molecular epidemiological studies are essential for the control, effective treatment, and understanding in transmission routes of HIV-1 infection. This study aims to determine the molecular epidemiology and antiretroviral drug resistance profiles of HIV-1 in northern Cyprus. The study involved 71 naive HIV-positive patients diagnosed in northern Cyprus between 2016 and 2022. HIV-1 subtypes and circulating recombinant forms (CRFs) were identified by phylogenetic analysis (neighbor-joining method) of pol gene sequences. Drug resistance mutations were analyzed using the World Health Organization (WHO) lists of mutations for surveillance. The Stanford University HIVdb program was used to interpret drug resistance mutations. In our study, 40 of 71 samples were successfully sequenced. Subtype B of HIV-1 was dominant with a rate of 52.5%, followed by CRF02_AG (20%) and G (7.5%) subtypes. The rate of subtype B (71.4%) in northern Cyprus was significantly higher than in the other country of origin (p = .028). Antiretroviral drug resistance was found in 15% of the sequenced serum samples. Nucleoside/nucleotide reverse transcriptase inhibitor (NRTI), non-nucleoside nucleotide reverse transcriptase inhibitor (NNRTI), and protease inhibitor (PI) resistance rates were 10% (4/40), 7.5% (3/40), and 2.5% (1/40), respectively. According to the results, it is noteworthy that the dominant subtype circulating in northern Cyprus is the B subtype, and CRFs were detected at a higher rate than expected.
Introduction
Human immunodeficiency virus (HIV) infections remain a significant global public health problem. It has been recorded that 39.0 million (33.1 − 45.7 million) people globally were living with HIV in 2022. In addition, within 2022, it has been estimated that 630,000 (480,000–880,000) HIV-related deaths and 1.3 million (1–1.7 million) newly infected HIV cases were reported. 1,2
The most advanced stage of HIV infection-acquired immunodeficiency syndrome (AIDS)-can be caused by two genetically distinct lentiviruses named HIV type 1 (HIV-1) and HIV type 2 (HIV-2). Compared with the two, HIV-1 is the most severe public health issue worldwide and is categorized into four groups. These are M (Major), O (Outlier), N (Non-M, Non-O), and P (Putative). 3,4 The dominant group among these is M and is further divided into nine subtypes (A, B, C, D, F, G, H, J, and K).
Among these, the M, A, and F are further subdivided into A1, A2, A3, A4, A6, and F1 and F2, respectively. Also, recombinations between HIV-1 subtypes have led to the development of novel variants, such as circulating recombinant forms (CRFs) and unique recombinant forms (URFs). Currently, 132 CRF variants have been identified worldwide. 5 –7
Globally, subtype C is the most common (46.6%) of all HIV infections, followed by subtype B (12%) and subtype A (10%). Whereas most cases are subtype C in eastern and southern Africa, followed by A1 and D subtypes, where subtypes B (83%), C (3.9%), and A (1.9%) are the most prevalently observed dynamics in western and central European regions. 5 –7 Among these subtypes, HIV-1 subtype B plays a vital role in HIV-1 pandemics. 8
Although HIV-1 is more common and progresses more aggressively, HIV-2 is less contagious than HIV-1. HIV-2 consists of 10 groups (A, B, C, D, E, F1, F2, G, H, and I), of which only groups A and B are endemic. 4,9 To date, only two recombinant forms of HIV-2 have been described. One was CRF (CRF01_AB) isolated from three different patients, and URF was seen in only one patient. 10
Currently, available HIV antiretroviral treatments are divided into six groups according to their mechanism of action. These are nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), protease inhibitors (PIs), non-nucleoside nucleotide reverse transcriptase inhibitors (NNRTIs), entry/fusion inhibitors (FIs), integrase inhibitors, and C-C-chemokine receptor type 5 (CCR5) antagonists. HIV-1 is treated with the combined use of three or more active substances and combined antiretroviral therapy (cART). 11 However, long-term cART results in toxicity and leads to the emergence of drug-resistant HIV strains. 12
Owing to the increasing antiretroviral drug resistance, the World Health Organization (WHO) recommends monitoring the factors related to the emergence of drug resistance and developing HIV drug resistance prevention strategies. 13,14 WHO defines that pretreatment HIV drug resistance (PDR) is the resistance detected among people initiating cART or people with prior antiretroviral drug exposure initiating or reinitiating first-line cART. 15 It has been reported that the seroprevalence of PDR varies between 3.5% and 25.8% among various countries. 16
Cyprus is the third most oversized island in the Mediterranean. On the island, two communities live where Turkish Cypriots majorly populate the north side of Cyprus, Turkish Republic of northern Cyprus (TRNC), and Greek Cypriots majorly inhabit the southern side of the Cyprus, Republic of Cyprus. 17 Northern Cyprus is claimed to be among the countries with relatively low endemicity, according to research undertaken to identify HIV seroprevalence. 18 –20 Individuals diagnosed as HIV positive who are not citizens of northern Cyprus are deported under the state's legislation. This strategy aims to control the country's HIV prevalence. 18
Treatment of HIV-positive TRNC citizens is determined according to the HIV/AIDS diagnosis, follow-up, and treatment guidelines prepared by the Turkish HIV/AIDS platform. 21 Even though investigations on HIV seroprevalence have been undertaken in northern Cyprus, there has been no research on HIV-1 molecular epidemiology.
HIV is one of the mandatory national notifiable diseases in northern Cyprus. This is a policy that the government or ministry of health has pursued for many years, and the data need to be collected openly and shared with the public. However, except from the number of HIV-positive cases, no other information is being shared, such as gender, subtype, nationality, or the transmission route. Therefore, the study aimed to determine the molecular HIV-1 epidemiology and subtype distribution in northern Cyprus between 2016 and 2022 and reveal the circulatory dynamics of HIV antiretroviral resistance patterns.
Methods
Ethical approval
The study was approved by the Near East University (NEU) Scientific Research Ethics Committee with the decision number NEU/2020/77-1015. The study was conducted retrospectively. Hence, informed consent was not required from the patients.
Study design
Seventy-one anti-HIV 1/2 reactive (positive) serum samples were obtained from HIV-infected patients diagnosed in the NEU Hospital, Microbiology Laboratory, between the 2016 and 2022 period involved in the study. HIV-infected patients included in this study were categorized as HIV carriers according to the European AIDS Clinical Society guideline. 22 No exclusion and/or inclusion criteria were used for the participants and all detected patients were included in the epidemiological scale. However, reverse transcriptase (RT) and protease region sequences were studied together for each patient to ensure confidence in epidemiological analyses, patients who partially sequenced were not included in the analysis part.
Anti-HIV testing
Anti-HIV 1/2 testing was carried out using ARCHITECT HIV ag/ab Combo Reagent Kit (Abbott Laboratories, Wiesbaden, Germany) with the Abbott ARCHITECT i1000SR device, which is the fourth-generation chemiluminescent microparticle immunoassay (CMIA) technology. Samples of individuals with a signal cutoff (S/Co) ≥1 were considered reactive. Anti-HIV 1/2-positive samples were centrifuged and reanalyzed at least twice with the sample assay, and the reactive consensus samples were stored at −80°C until analysis. The tests followed the HIV/AIDS diagnosis treatment guidelines. 23
HIV-1 RNA quantitation
HIV-1 RNA was determined and quantitated using QIAsypmhony and Rotorgene Q/artus HIV-1 QS-RGQ v1 (QIAGEN GmbH, Hilden, Germany).
Sequence analysis
HIV-1 pol gene was sequenced by using the Sanger di-deoxy termination technique. The regions of HIV-1 reverse transcriptase, protease, and integrase composing of the codons from 1 to 240, 1 to 99, and 62 to 182, respectively, were sequenced to identify HIV-1 subtypes and drug resistance mutations, following the methodology outlined by Sayan et al. 3
HIV-1 complementary DNA (cDNA) was synthesized using a First Strand cDNA Synthesis Kit (Thermo Scientific, Inc., Fermentas, Lithuania). 11 The amplification protocol was 45 s each at 95°C, 55°C, and 72°C. A highly Pure Product Purification Kit (Roche Diagnostics) was used to purify all the polymerase chain reaction (PCR) products. The sequence was performed on the ABI PRISM 310 Genetic Analyzer with the DYEnamic ET Terminator Cycle Sequencing Kit (Amersham Pharmacia Biotech, Inc., Piscataway, NY).
The cycle sequencing (35 cycles) was performed at 95°C for 20 s, 50°C for 25 s, and 60°C for 120 s. Furthermore, Vector NTI v5.1 software (InforMax, Invitrogen, Life Science Software, Frederick, MD) was used to assemble the sequences obtained from the electropherogram.
HIV-1 phylogenetic analysis
The neighbor-joining method was carried out as a tree construction method. The phlogenetic tree constructed on CLC sequence viewer 8.0 (Qiagen, CLC bio A/S, Aarhus, Denmark) with Neighbore-Joinig method and Jukes–Cantor distance measure. All HIV-1 subtypes reference sequences provided from GenBank.
Drug resistance mutation analysis
Mutations that were present on RT, protease, and integrase domains were identified using the list of surveillance transmitted HIV drug resistance mutations (TDRMs) and the recently published surveillance drug resistance mutation list for integrase strand transfer inhibitor (INSTI) drug class with WHO HIV ResNet Working Groups. 24,25 Furthermore, the Stanford University HIVdb program (genotypic resistance interpretation algorithm) was used to interpret drug resistance mutations. 26
The sequences were submitted to the GenBank database with the submission ID numbers 2020/77-1015 and provided GenBank accession numbers: ON983131–ON983155.
Statistical analysis
Pearson chi-square or Fisher's exact tests measured the differences between two proportions. A one-way analysis of variance test was performed to determine the statistical differences in the groups' mean. Statistical analyses were performed using SPSS Demo Ver 22 (SPSS, Inc., Chicago, IL), and a p value <.05 was accepted to be statistically significant.
Results
Seventy-one HIV-infected antiretroviral-naive patients were involved in the study. Among these patients, 55 (77.5%) were men, and 16 (22.5%) were women, with a mean age of 29.62 ± 9.42 (range; 18–65 years). Of all the serum samples, only 40 (56.3%) could be sequenced; hence enabling HIV-1 subtypes to be determined. In total, 33 of 40 (82.5%) were men, and 7 of 40 (17.5%) were women for whom sequence analyses were performed, with a mean age of 29.65 ± 10.76 (range; 18–65 years). Moreover, 21 (52.5%) of them were from northern Cyprus, 6 (15.0%) were from Turkey, 1 (2.5%) from England, and 12 were (30.0%) from Africa. Table 1 indicates the clinical and epidemiological characteristics of HIV-1 patients.
Characteristics of the HIV-1-Infected Naive Patients Sequenced in Northern Cyprus
BSX, bisexual contact; DR, drug resistance; HIV, human immunodeficiency virus; HSX, heterosexual contact; MSM, men who have sex with men; NA, not available; NNRTI, non-nucleoside nucleotide reverse transcriptase inhibitor; NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; PI, protease inhibitor.
Subtype B was the most common among HIV-1-infected patients, with a rate of 52.5% (n = 21), followed by subtypes CRF02_AG (20%), G (7.5%), C (5%), A1 (2.5%), and F (2.5%). Three patients had both B and CRF02_AG subtypes. It was determined that 71.4% (n = 15) of individuals from northern Cyprus were infected with subtype B, whereas 1 patient had B and CRF02_AG subtypes. Figure 1 shows the phylogenetic analysis of isolates sequenced in our study.
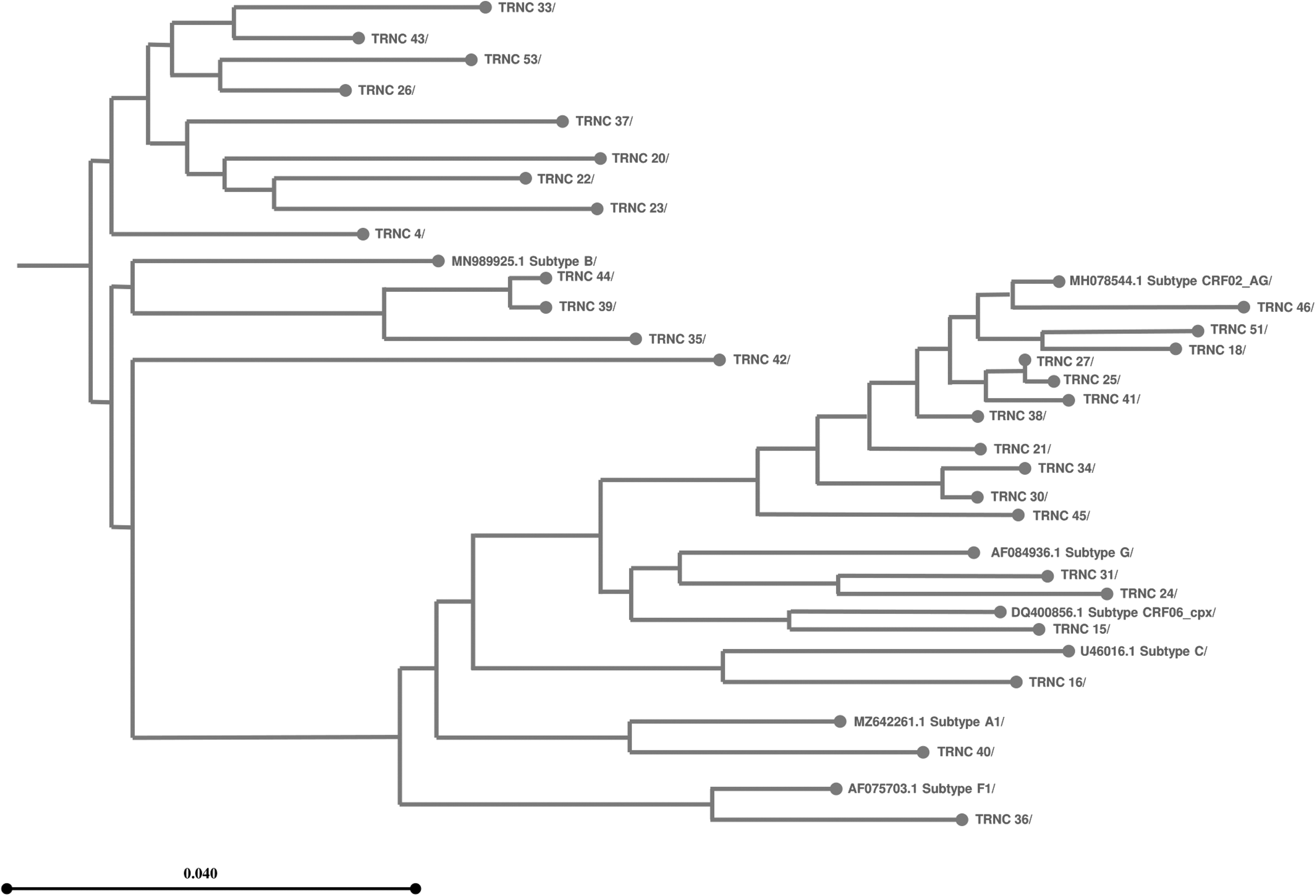
Phylogenetic tree of pol gene in the northern Cyprus isolated HIV-1 strains. The neighbor-joining method was carried out as a tree construction method. The phlogenetic tree constructed on CLC sequence viewer 8.0 (Qiagen, CLC bio A/S, Aarhus, Denmark) with Neighbore-Joinig method and Jukes–Cantor distance measure. All HIV-1 subtypes reference sequences provided from GenBank. Bootstrap support values were used in 1,000 replicates. HIV, human immunodeficiency virus.
The transmission routes of 22 of the sequenced HIV-1-infected naive patients were known. It was found that HIV-1 transmission frequently occurred in MSM (men who have sex with men; 54.5%, 12/22), followed by heterosexual transmission (40.9%, 9/22). No significant relationship was obtained between the transmission routes and age (p = .103). Furthermore, there was no significant association between HIV-1 subtypes and age (p = .819).
The incidence of subtype B in citizens of northern Cyprus was significantly higher than that of citizens of other countries (p = .028) (Table 1). In addition, it was observed that subtype B was lower in heterosexual patients than in others, and MSM-type transmission was found to be more common in subtype B (p = .036). In contrast, no correlation was found between the mean age of the infected patients with subtype B and those infected with other subtypes (p = .167). Furthermore, no association was found between gender (male, female) and drug resistance with subtype B infection (p = .592, p = .544, respectively) (Table 2).
Characteristics of Demographic and Laboratory Parameters Between Subtype B and Other Subtypes in the Study Group
Statistically significant (p < .05).
NRTI, NNRTI, and PI drug resistance mutations were analyzed in all sequenced samples. Antiretroviral drug resistance mutations were determined in six (15%) HIV-1-infected patients. According to this analysis, 12.5% (5/40) NRTI, 10% (4/40) NNRTI, and 2.5% (1/40) PI resistance-associated mutations were detected. Only one PI resistance mutation detected in our study belonged to a Nigerian patient (Table 1).
No significant differences were obtained between drug resistance mutations and gender in HIV-1-infected patients (p = .721). In addition, when each three-drug resistance of NRTI, NNRTI, and PI was compared with gender separately, it was seen that there was no significant relationship found; p = .552, p = .552, p = .825, respectively. The mean age of HIV-1-infected patients diagnosed with and without drug-resistance mutations was 27.33 ± 11.74 and 30.06 ± 10.72 years, respectively. In addition, no significant differences were obtained between the mean age of positive HIV-1-infected naive patients with and without drug resistance (p = .574).
The main limitation to this study was that the majority of the samples analyzed were not successfully amplified and sequenced. The lack of data from these samples could arise due to various factors such as sample degradation due to prolonged storage, technical issues specific to the assay, or the potential presence of HIV-2 infection in some of the samples collected for analysis.
Discussion
Molecular epidemiology analysis of HIV subtypes and transmission patterns helps clarify HIV subtype variability and the global spread of HIV. Investigation of the effect of these subtypes on antiviral treatment may also enable better treatment response. In this study, HIV-1 subtypes were identified that had never been elucidated in northern Cyprus previously. A total of 71 strains isolated from HIV-infected naive patients were analyzed, but only 40 of these could be sequenced for HIV-1. Our findings showed that subtype B was dominant over other subtypes in northern Cyprus during the given period.
Some previous studies were conducted in southern Cyprus. 27 –29 Kousiappa et al. studied 74 HIV-1-infected patients between 2007 and 2009 and analyzed subtypes with rates B (48.6%), A (18.9%), C (10.8%), CRF02_AG (8.1%), CRF11_cpx (2.7%), F1 (1.4%) CRF37_cpx (1.4%). 27 Similarly, another study determined that the prevalence of subtype B (41%) was the most prevalent, followed by A1 (19%). 28 In the study of Pineda-Pena et al., which included 355 HIV-1-infected patients, it was emphasized that subtype B was dominant, with a rate of 54% in southern Cyprus. 29
In similar studies conducted in southern Cyprus, dominant subtype results were obtained identically to this study. Only differences were observed between CRFs and non-B subtypes. In particular, it was noted that the number of CRF02_AG was significantly high (p ≤ .001), and the number of subtypes A was low (p = .025) in northern Cyprus (Table 3). The tourism dynamics in the southern Cyprus region are much higher than that in the northern part of the island and subtype. A is more common in the south, which may be due to Russian and Ukraine visitors in which subtype A is more dominant. 30,31
Comparison of HIV-1 Subtypes in Other Studies on Cyprus
Statistically significant (p < .05).
CRF, circulating recombinant form; URF, unique recombinant form.
In contrast, CRF02_AG was found to be significantly higher in northern Cyprus (Table 3). This could be attributed to the significant influx of students from the African continent, primarily for educational purposes. Northern Cyprus geographically receives immigration from many countries, especially from African countries. 32,33
It has been reported that the performance of algorithms used to determine non-B subtypes could be better and may show inconsistencies with phylogenetic analysis results, especially in identifying CRFs. 34 In this study, B/CRF02_AG recombinant variant was detected in three patients, but three showed branching in the CRF02_AG region due to phylogenetic analysis. It is reported that these recombinant variants circulating in west Africa and France are seen more frequently in homosexual men. 35 Although these patients were men, we did not have any information about their sexual behavior.
Another striking point in our study is that the G subtype was not found in southern Cyprus, but was detected in northern Cyprus. The most recent study on the molecular epidemiology of HIV-1 in southern Cyprus was published in 2018. For this reason, sequence analyses are of great importance in contributing to the literature with such studies. G subtype caused an outbreak in Russia between 1988 and 1990. However, in recent years, the G subtype has been rare in these regions. This subtype has reached the highest prevalence in some African countries, accounting for 5%–50% of HIV-1 infections.
Some G variants have spread from Africa to European countries, such as Portugal and Spain. In Portugal, the G subtype is considered the second most prevalent subtype after B. 36 –38 The fact that many people from Africa have come to our country in recent years to study and work explains the presence of the G subtype in this region.
Differences in HIV-1 subtypes may alter drug resistance and ART susceptibility. The diagnostic and follow-up efficiency of HIV tests varies according to groups and subtypes. As a result, determining HIV-1 subtypes through molecular epidemiology investigations is critical. 34 –39 The rate of overall antiretroviral drug resistance detected in our study was 15%, and the frequencies of NRTI, NNRTI, and PI drug resistance were 10%, 7.5%, and 2.5%, respectively. Our findings show that drug resistance is relatively higher in all three groups than in other studies conducted in Cyprus.
However, all detected mutations are low or potential low-level mutations (NRTI: L74I, M184E, K70R, M41L, T215P; NNRTI: Y181I, Y188T, E138A, L100V; PI: L89M). Although no significant PI-associated mutations were observed in the study of Kousiappa et al. in southern Cyprus in 2011, minor PI-associated mutations were detected in 52 (98%) of 53 HIV-1-infected patients. In addition, no NRTI and NNRTI mutations were found in the same study. 27 In a study published in 2018 in the southern Cyprus region, total drug resistance mutation was determined as 3.7%, whereas NRTI was 0.0%, NNRTI was 1.2%, and PI was 2.4%. 26
Therefore, we do not expect mutations in circulation to cause primary drug resistance. These are mutations produced by natural HIV-1 replications. All these results show that we need to follow the HIV-1 subtype circulation and the resistance mutations. This will be very helpful in identifying circulating HIV-1 from a molecular epidemiological point of view.
Conducting molecular epidemiological studies on HIV allows for determining genetic diversity, transmission routes, dynamics of the virus, and antiretroviral drug resistance. Unfortunately, there has been no molecular epidemiological study on HIV in northern Cyprus. Our data show that it will be easier to monitor the HIV-1 spread on the island in the coming years. Establishing a sequence database for HIV in island countries may be necessary and valuable. This will be very helpful in monitoring HIV circulation and possible CRF traffic, especially in divided island countries. In addition, detecting HIV-1 at a rate of ∼50% makes us think that HIV-2 may also be in circulation. Therefore, it would be beneficial to establish an infrastructure to monitor HIV-2 dynamics in Cyprus.
Conclusion
In conclusion, the study demonstrates that the dominant circulating HIV-1 subtype in northern Cyprus is subtype B. The reason for not being heterogenic may be due to the legal regulations in the country and the deportation of HIV-infected foreign nationals by the government. Therefore, the diversity of HIV-1 subtypes remains unchanged. Considering the cosmopolitan nature of the island, we also believe that individuals with positive anti-HIV tests but no detectable HIV-1 RNA should also be evaluated for HIV-2.
As can be understood from the results, economic, demographic, and even viral dynamics can differ in Cyprus, where two different communities live. Therefore, considering the island of Cyprus, creating a common sequence database may be more beneficial in following HIV-1 dynamics. Also, HIV-2 needs to be part of routine analysis, especially in cosmopolitan countries such as Cyprus.
Footnotes
Authors' Contributions
E.G., K.S., T.S., and M.S. designed the study. E.G. and A.A. collected and prepared the data. E.G., A.A., and N.S. performed routine laboratory tests and statistical analyses. M.S. performed the molecular tests. E.G., A.A., and N.S. drafted the article. K.S., M.S., and T.S. evaluated all data. All authors approved the final version of the article.
Author Disclosure Statement
The authors declare that they have no conflicts of interest regarding the publication of this article.
Funding Information
No funding was received for this study.