
Abstract
Omega-6 (n-6) and omega-3 (n-3) polyunsaturated fatty acids (PUFAs) are vital for fetal metabolic programming and immunomodulation. Higher n-6:n-3 ratios, reflecting a proinflammatory eicosanoid profile, are associated with adverse perinatal outcomes. Limited data exist, however, on n-6 and n-3 PUFAs specifically in the context of HIV and pregnancy. Our objective was to assess HIV clinical factors associated with PUFA signatures in pregnant persons with HIV (PWH). In this observational cohort, third trimester plasma PUFA concentrations (six n-6 PUFAs, four n-3 PUFAs) were measured, each as a percent of total fatty acid content, via esterification and gas chromatography in pregnant PWH enrolled from 2009 to 2011 in the Nutrition substudy of the Pediatric HIV/AIDS Cohort Study. PUFA ratios (n-6:n-3) were calculated. Exposures assessed were first/second trimester CD4 count (<200 vs.
Introduction
Increased metabolic demands in pregnancy necessitate optimal nutritional intake to mitigate metabolic stress and prevent adverse maternal, neonatal, and childhood outcomes. 1 –3 Long-chain polyunsaturated fatty acids (PUFAs) are of particular importance as they cross the placenta and affect fetal inflammatory, metabolic, and vascular profiles. 4,5 Among >20 types of PUFAs, the omega-6 (n-6) and omega-3 (n-3) PUFAs are called “essential fatty acids (FAs)” because they cannot be synthesized endogenously and can only be introduced through dietary consumption. 6 Maternal and fetal PUFA concentrations are closely correlated. 5 An imbalance in the ratio of n-6 to n-3 PUFA concentrations in maternal plasma can perturb placental development and transplacental transfer of PUFAs, which subsequently affects fetal neuroendocrine function, energy metabolism, and metabolic programming. 7
Linoleic acid (LA; n-6 FA) and alpha-linolenic acid (ALA; n-3 FA) are the main essential PUFAs obtained through diet that are subsequently converted to their biologically active metabolites. LA is converted to arachidonic acid (AA; n-6), the main precursor of proinflammatory eicosanoids (i.e., prostaglandins, prostacyclins, leukotrienes, and thromboxanes; Fig. 1). ALA is converted to eicosapentaenoic acid (EPA; n-3) and docosahexaenoic acid (DHA; n-3), the main precursors to anti-inflammatory eicosanoids. 7 The ratios of proinflammatory to anti-inflammatory eicosanoids influence numerous cell and tissue functions. Higher maternal plasma concentrations of n-6 relative to n-3 PUFAs have been associated with adverse maternal, neonatal, and childhood outcomes. 8 –10
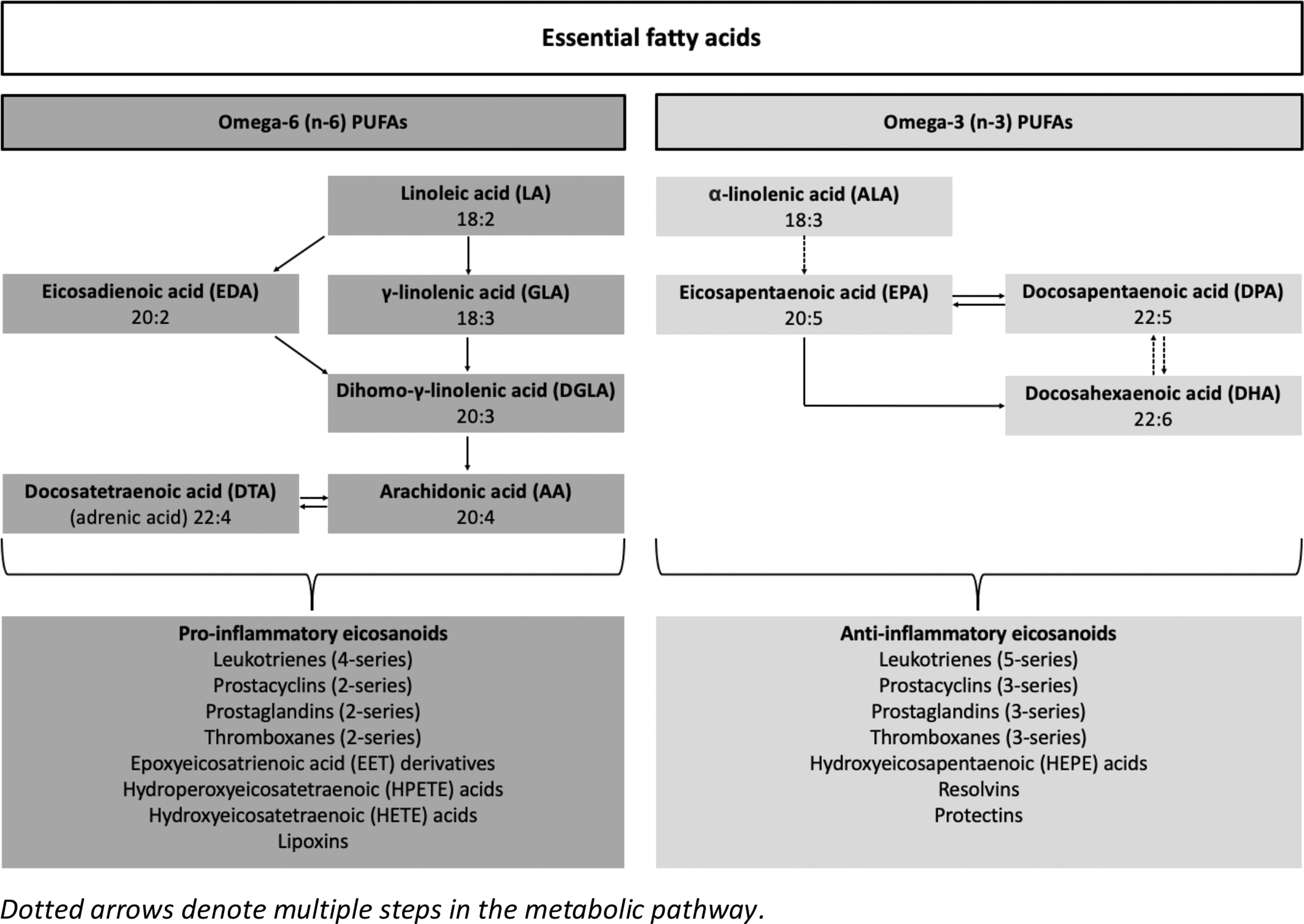
Relationship of n-3 and n-6 PUFAs with inflammatory eicosanoids. n-3, omega-3; n-6, omega-6; PUFAs, polyunsaturated fatty acids.
Pregnant persons with HIV (PWH) and their offspring represent a particularly important population at increased risk for metabolic pregnancy complications. The combination of chronic inflammation and oxidative stress associated with HIV infection, exposure to antiretroviral therapy (ART), and suboptimal dietary intake associated with lower socioeconomic status contributes to altered metabolic and cardiovascular profiles. 11 –14 Evaluation of PUFA concentrations in PWH has been very limited in scope, although increased n-3 PUFA concentrations are associated with reduced inflammatory profiles in nonpregnant adults with HIV. 15,16 Improved maternal diet quality has been investigated as a strategy in Sub-Saharan Africa to improve the health of PWH, who are more likely to experience preterm birth and low birthweight; yet, there remains a paucity of data regarding PUFAs specifically in pregnant PWH in high-income countries, where they have a markedly different dietary experience. 17,18
Therefore, we sought to compare third-trimester plasma PUFA concentrations in pregnant PWH in the United States by maternal HIV immunosuppression status, HIV viremia status, and ART class, hypothesizing that higher concentrations of n-6 relative to n-3 would be identified among those with greater immunosuppression, higher viral load (VL), or receipt of protease inhibitor (PI)-based ART.
Materials and Methods
Study population
The Surveillance Monitoring for ART Toxicities Study (SMARTT) of the Pediatric HIV/AIDS Cohort Study (PHACS) Network has been enrolling pregnant PWH and their children at 22 sites across the United States, including Puerto Rico, since 2007. The Nutrition sub-study (R01HD060325) of SMARTT enrolled PWH predominately in the third trimester of pregnancy from 2009–2011 at 15 of the 22 clinical sites; the sub-study obtained blood samples in the third trimester. 14 Among those enrolled in the Nutrition substudy, pregnant PWH with multiple gestations, a history of bariatric surgery, no valid dietary recall, and incomplete data were excluded from this analysis. The institutional review board at each recruitment site, the University of Miami Human Subjects Research Office, and the Harvard T.H. Chan School of Public Health approved the SMARTT protocol and the Nutrition substudy. Participants provided written informed consent.
Data collection
Information on sociodemographic characteristics, obstetric history, and other clinical characteristics were collected through interview and medical record review. Additional data abstracted from the medical chart included prepregnancy maternal body mass index (BMI), trimester of prenatal care initiation, gestational age at blood draw [calculated from the date of the last menstrual period (LMP) or prenatal ultrasound if LMP was not known], earliest HIV RNA VL, CD4 count, and ART drug class in the first/second trimester, and timing of ART initiation and ART class.
Assessment of third trimester PUFA concentrations
PUFA concentrations were assessed from plasma specimens obtained in the third trimester of pregnancy and stored at −70°C until they were sent to the Department of Nutrition at the Harvard T.H. Chan School of Public Health for analysis. Maternal plasma concentrations of individual PUFAs were measured, each as a percentage of total FA content, via esterification and gas chromatography. 19 The six n-6 PUFAs and four n-3 PUFAs measured are given in Figure 1. The plasma concentrations of all n-6 PUFAs were summed, as were the plasma concentrations of all n-3 PUFAs.
Total lipids were extracted from plasma by previously defined processes. 19 FAs were transmethylated with methanol and sulfuric acid. 20,21 After esterification, samples were evaporated, and the FA methyl esters were redissolved in iso-octane. FAs were separated using an Agilent Model GC 6890 FID gas chromatograph with 7673 autosampler injector (Palo Alto, CA), splitless injection port at 240°C, and a constant flow hydrogen carrier gas at 1.3 mL/min. One microliter of sample was injected into a fused silica capillary cis/trans column SP2560, a 100 m × 0.25 mm internal diameter × 0.20 μm film (Supelco, Belefonte, PA). Peak retention times were identified by injecting known standards, and purity ranges were all >99% (NuCheck Prep, Elysium, MN), using Agilent Technologies ChemStation A.08.03 software for analysis. Forty-two FAs were identified with this methodology.
The coefficient of variations for selected n-3 PUFAs were as follows: ALA 6.5%, EPA 5.2%, and DHA 5.1%. For n-6 PUFAs, CVs were 3.6% for LA and 2.7% for AA.
Twenty four–hour dietary recalls
At the entry visit, participants received a prepaid cell phone for the purpose of collecting dietary intake information. Trained nutritionists at the University of Miami conducted the cell phone interviews centrally during the third trimester of pregnancy. Twenty four–hour dietary recalls were obtained in accordance with the multiple pass dietary recall method asking about all foods and beverages consumed on three separate occasions including two weekdays and one weekend day over a 2-week period. 22 All recall periods were separated by at least 1 day. Nutritional supplement use was collected at the end of the first 24-h recall covering the previous 30 days. Data were analyzed with the Nutrition Data System for Research (NDSR) version 2010 and 2011 (Nutrition Coordinating Center, University of Minnesota). Each 24-h recall was reviewed for reliability, and any concerns clarified and documented. Interviewers interpreted reliability of answers to the 24-h recall by taking into account participants' engagement during the interview. Those participants with unreliable data were encouraged to re-engage with follow-up recalls subsequently performed.
The team of three nutritionists carried out a protocol for quality assurance suggested by NDSR, with the validity of outlying values for energy, macronutrients, and key micronutrients assessed. We excluded data deemed invalid/unreliable. The average of all valid recalls was calculated for each nutrient. In addition, household food security was assessed with the U.S. Household Food Security Module Six-Item Short Form. 23
Statistical analysis
The primary exposures of interest included: (1) HIV immunosuppression (defined as CD4 count, <200 vs.
Frequency distributions were produced for baseline sociodemographic and clinical factors. Distributions were plotted for continuous variables to check for outliers. Data were transformed if assumptions of normality were not met. When necessary, the data management center was queried to verify values and update missing values when possible. For missing exposures, missing indicators were used in the models, but missing outcomes were not imputed.
Maternal characteristics and plasma concentrations of all n-6, all n-3, and individual PUFA concentrations including AA, DHA, and EPA were compared by CD4 strata, HIV strata, and ART drug class using Wilcoxon rank-sum or Fisher's exact tests as appropriate. In addition, we plotted maternal dietary intake of n-6, n-3, and n-6:n-3 ratio by maternal plasma concentrations of these measures.
Linear regression models using generalized estimating equations were fit with the robust variance estimator to estimate mean differences [95% confidence intervals (CIs)] in n-6:n-3 and AA:EPA+DHA ratios by first/second trimester CD4 count, HIV VL, and PI-based versus other ART, unadjusted and adjusted for potential confounders. Potential confounders considered in adjusted analyses included age, education, tobacco use, prepregnancy or early pregnancy BMI, PI-based versus non–PI-based ART, and gestational age at blood draw. A category for missing data was included in the variable for BMI. Mean differences and the 95% CIs were reported.
With a sample size of 264 individuals in this secondary analysis of the SMARTT Nutrition substudy, a priori we estimated >80% power to detect a minimum difference of 0.8, 0.5, and 0.5 in the n-6:n-3 ratio when assessed according to CD4 count, HIV VL, and ART drug class exposure, respectively. All statistical calculations were performed using SAS Version 9.4 (SAS Institute, Cary, NC).
Results
Among 317 maternal–infant pairs enrolled into the Nutrition substudy across 15 clinical sites, 296 had laboratory evaluation of PUFA concentrations in maternal plasma and met inclusion criteria for this analysis. Thirty-two maternal–infant pairs were excluded, and the remaining 264 maternal–infant pairs were included in the analysis (Fig. 2).
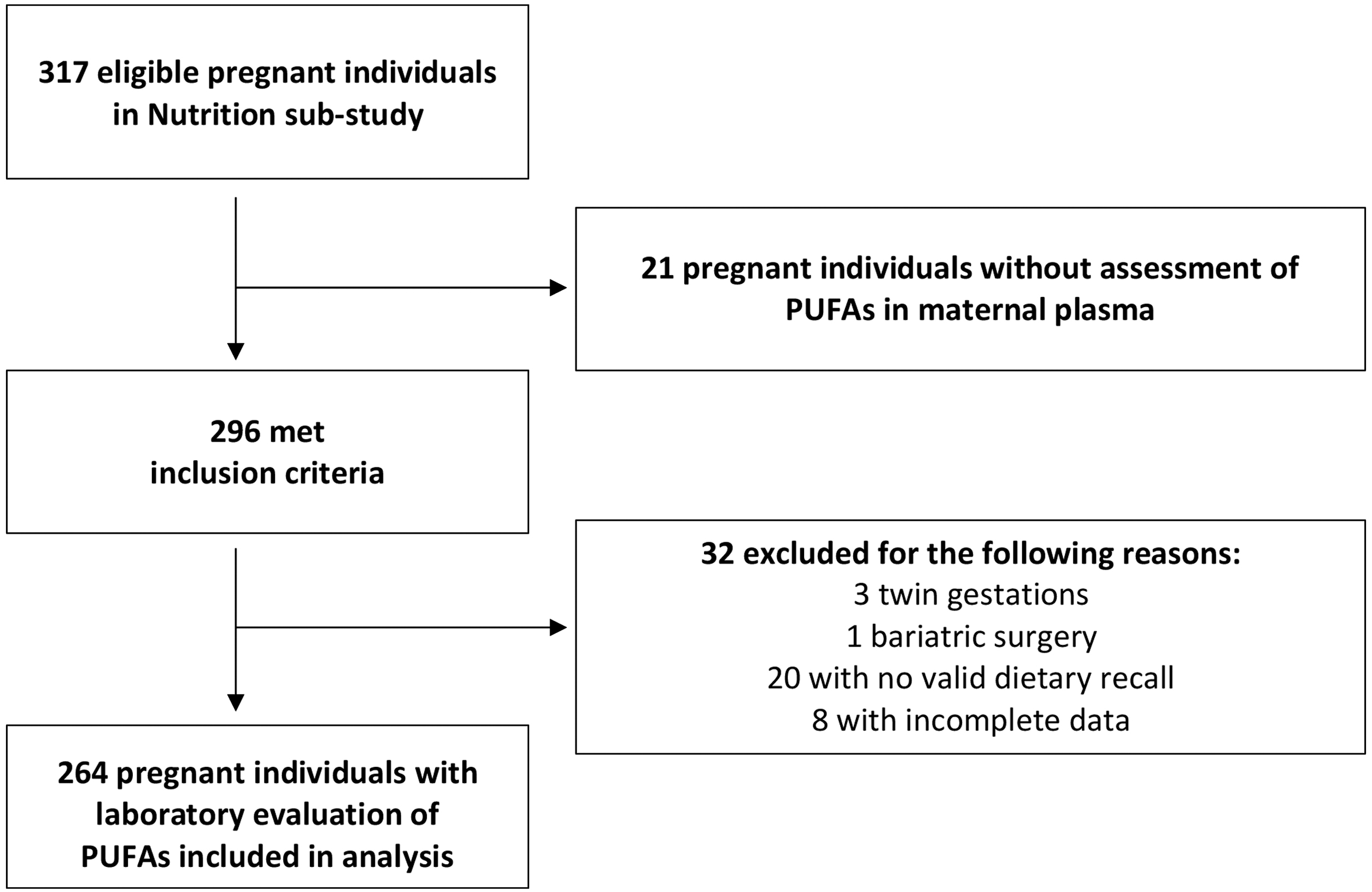
Flow chart demonstrates inclusion and exclusion of participants in the analytic cohort.
The majority of individuals had a household income <$10,000 (58%), self-identified as Black (69%), and of those with available prepregnancy BMI, 66% were considered overweight or obese prepregnancy (Table 1). Overall, 35% reported food insecurity (25% low and 13% very low food security). Eighty percent individuals received their HIV diagnosis before the current pregnancy, and 69% had used ART before pregnancy; 94% received ART by the second trimester with a predominance of PI-based ART (84%). Fifty-six percent had VL ≥400 copies/mL in the first/second trimester, although only 12% had CD4 < 200 cells/mm3. Gestational age at which blood specimens for PUFA assays were collected ranged from 24 to 40 weeks with a median (interquartile range, IQR) of 32 (30–36). Of note, ART regimens assessed in this population included predominately PI-based and non-nucleoside reverse transcriptase inhibitor–based ART with a backbone of two nucleoside reverse transcriptase inhibitors, primarily tenofovir disoproxil fumarate plus either emtricitabine or lamivudine.
Participant Characteristics at Enrollment
Missing data: maternal age at LMP (n = 3), race (n = 9), education (n = 4), annual household income (n = 26), marital status (n = 3), illicit drug use (n = 3), alcohol use (n = 3), tobacco use (n = 3), maternal prepregnancy BMI (n = 51), trimester of prenatal care initiation (n = 3), HIV diagnosis before current pregnancy (n = 3), trimester of ART initiation (n = 3), Zidovudine at first ART use (n = 17), PI use (n = 3), earliest CD4 count (n = 15), earliest HIV VL (n = 21).
ART, antiretroviral therapy; BMI, body mass index; IQR, interquartile range; LMP, last menstrual period; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; VL, viral load.
Overall, the median (IQR) third-trimester n-6 and n-3 PUFA concentrations and n-6:n-3 ratios were 37.37 (15.04–46.72), 2.80 (1.32–8.62), and 12.99 (1.75–23.15), respectively. n-6 and n-3 PUFA concentrations and n-6:n-3 ratios were generally similar by both first/second trimester and third trimester CD4 count (Table 2). In contrast, although median differences in n-6 PUFA concentrations were small by HIV VL status with no detectable difference in the first/second or third trimesters, median n-3 concentrations were lower in pregnant PWH with VL ≥400 copies/mL, compared with those with VL <400 copies/mL, for EPA, DHA, EPA+DHA, ALA+EPA+DHA, and all n-3 combined across gestation periods. Although ALA concentrations were similar by VL status in the first/second trimester, we identified a difference in ALA by third trimester VL status (Table 3).
Fatty Acid Concentrations as a Percent of Total Fatty Acid Content (%) and Ratios by CD4 Count
n-6 fatty acids included linoleic, gamma linolenic, eicosadienoic, dihomo-gamma-linolenic, arachidonic, and adrenic (docosatetraenoic) acid.
n-3 fatty acids included alpha-linolenic, docosapentaenoic, eicosapentaenoic, and docosahexaenoic acid.
AA, arachidonic acid; ALA, alpha-linolenic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; IQR, interquartile range; LA, linoleic acid; n-3, omega-3; n-6, omega-6.
Fatty Acid Concentrations as a Percent of Total Fatty Acid Content (%) and Ratios by HIV Viral Load Status
n-6 fatty acids included linoleic, gamma linolenic, eicosadienoic, dihomo-gamma-linolenic, arachidonic, and adrenic (docosatetraenoic) acid.
n-3 fatty acids included alpha-linolenic, eicosapentaenoic, docosapentaenoic, and docosahexaenoic acid.
Furthermore, we observed a higher median n-6:n-3 PUFA ratio in PWH with VL ≥400 copies/mL compared with those with VL <400 copies/mL in both the first/second trimesters (13.53 vs. 11.98, p < .01) and third trimester (14.12 vs. 12.81, p < .01), including when the data were transformed logarithmically.
No differences were detected for all n-6 and all n-3 PUFA concentrations by ART class (Supplementary Table S1), including specifically by PI-based versus non–PI-based ART (Table 4).
Fatty Acid Concentrations as a Percent of Total Fatty Acid Content (%) and Ratios by Protease Inhibitor–Based Versus Nonprotease Inhibitor Antiretroviral Therapy at Last Menstrual Period or in the First/Second Trimester
n-6 fatty acids included linoleic, gamma linolenic, eicosadienoic, dihomo-gamma-linolenic, arachidonic, and adrenic (docosatetraenoic) acid.
n-3 fatty acids included alpha-linolenic, docosapentaenoic, eicosapentaenoic, and docosahexaenoic acid.
In models evaluating differences in the n-6:n-3 and the AA:EPA+DHA ratios adjusted for age, education, tobacco use, prepregnancy BMI, and PI-based versus non–PI-based ART, both n-6:n-3 (mean difference 1.60; 95% CI = 0.79–2.48) and AA:EPA+DHA (mean difference 0.51; 95% CI = 0.26–0.76) ratios were higher in PWH with VL ≥400 copies/mL compared with <400 copies/mL in the first/second trimester (Table 5). Adjusting for gestational age at blood draw did not alter the results observed with respect to VL status, and therefore this covariate was not included in the final models. We did not detect differences in n-6:n3 or AA:EPA+DHA ratios by CD4 count in the first/second trimester after adjusting for the same above potential confounders.
Estimated Mean Difference in Third-Trimester n-6:n-3 Ratios by CD4 Count and HIV Viral Load Status in the First/Second Trimester
Adjusted for maternal age at conception, educational level, tobacco use in the first trimester, body mass index, and PI-based versus non-PI antiretroviral therapy.
n-6 fatty acids included linoleic, gamma linolenic, eicosadienoic, dihomo-gamma-linolenic, arachidonic, and adrenic (docosatetraenoic) acid. n-3 fatty acids included: alpha-linolenic, docosapentaenoic, eicosapentaenoic, and docosahexaenoic acid.
CI, confidence interval; PI, protease inhibitor.
Consumption of any type of nutritional supplement was evident in 95% of PWH, but no participant reported intake of n-3 or n-6 supplements. Weak correlations were identified between dietary intake of n-3 and plasma n-3 concentrations (rho = 0.10, p = .08) and between n-6:n-3 ratio calculated from recalls and plasma n-6:n-3 ratio (rho = 0.16, p = .008), but no correlations were identified between dietary intake of n-6 and plasma n-6 concentrations (rho = −0.02, p = .70) (Supplementary Fig. S1).
Discussion
In this U.S. cohort of pregnant PWH, third trimester n-6:n-3 ratios were elevated overall. PWH with viremia in pregnancy had higher n-6:n-3 ratios, which is associated with a propensity for inflammation. However, we did not detect differences in n-6:n-3 ratios by HIV immunosuppression or ART class, or a strong correlation with dietary intake.
A dearth of literature exists regarding plasma concentrations and ratios of n-6 and n-3 PUFAs, and their association with HIV clinical factors in pregnancy. One small Canadian study identified high concentrations of AA in the third trimester of pregnancy in PWH, a 78% increase compared with HIV-seronegative pregnant persons, although they also identified high concentrations of DHA and EPA in maternal plasma. 24 This study did not comment on the PUFA concentrations in pregnant PWH with respect to their VL status and did not report on n-6:n-3 ratios. Otherwise, studies related to PUFAs in pregnant PWH have principally evaluated the association of n-3 and other lipid-based supplementation with clinical outcomes among African populations, but these also do not report n-6:n-3 ratios or their association with HIV immune status, VL status, or ART class. 18,25
In pregnancies unaffected by HIV, the n-6:n-3 ratio in maternal plasma was as low as 6.1 (±1.7) in a cohort from the Netherlands and as high as 29.5 (±11.7) in a cohort from Spain. The wide range between studies may be partially explained by potential differences in techniques for measuring FA metabolites or simply differences in populations. 9,26 –29 Comparatively, in our U.S. cohort of pregnant PWH, the median n-6:n-3 ratio, 12.99, falls within this range, yet is notably more than double the recommended 6:1 ratio for optimal health. 30 –33 Among available literature regarding PUFA ratios in HIV-seronegative pregnant persons, most generalizable to our study is an urban cohort of HIV-seronegative pregnant persons in the U.S., 34 in which the median n-6:n-3 PUFA ratio measured in the third trimester was 11.7 (IQR, 9.9–12.3), less than that identified in our cohort of PWH.
It is important to note that previously published reference ranges of PUFA concentrations in pregnancy, among individuals without HIV, have heterogeneous units of measure reported and may vary based on the specific laboratory assay used. 26,35,36 Thus, reference ranges for PUFA concentrations in pregnancy have not been standardized, limiting our ability to compare our findings among pregnant PWH with the general population of pregnant persons.
We found VL ≥400 copies/mL to be associated with higher n-6:n-3 PUFA ratios compared with those with controlled viremia. This was not surprising given that viremia is known to be associated with oxidative stress and general inflammation. 12,37 Ongoing viral replication creates an imbalance in n-6:n-3 PUFA ratios at the cellular level such that pro-oxidant and proinflammatory n-6 profiles exceed the antioxidant and anti-inflammatory defenses of n-3 PUFAs, as observed in our cohort. Viral protein replication induces oxidative stress by causing endothelial dysfunction, mitochondrial dysfunction, escalation of reactive oxygen species production, and lipid peroxidation, which leads to a proinflammatory PUFA milieu. 11,12,38 –40 HIV viral particles also induce inflammation as potent activators of toll-like receptors (TLRs). 41 TLRs are a family of pattern-recognition receptors that recognize conserved molecules from pathogens, such as lipopolysaccharide (LPS), initiate innate immune responses, and induce systemic inflammation. 42 TLRs are also linked to eicosanoid metabolism. 41
HIV viral replication results in disruption of mucosal-associated lymphoid tissues and translocation of microbial products across the intestinal mucosa into the peripheral circulation, producing high levels of plasma LPS recognized by these TLRs, which induce rapid activation of AA metabolism and upregulate the proinflammatory n-6 metabolic pathway. 41,43
However, we did not detect an association between ART class and CD4 count with PUFA ratios. Our findings suggest that if VL decreases, n-6:n-3 PUFA ratios also decrease, shifting the balance toward a less inflammatory profile, irrespective of the ART regimen used to achieve viral suppression. CD4 count alone has also been shown to have limited utility as a proxy of ongoing inflammation. 44,45
A high n-6:n-3 ratio in pregnancy is not a benign process and may be considered a marker of excessive inflammation and oxidative stress that exceeds the physiologic upregulation of antioxidant defenses of pregnancy. A balance of n-6 relative to n-3 PUFAs is important for general maintenance of normal inflammatory responses and immune homeostasis between pro- and anti-inflammatory eicosanoids, cytokines, and other signaling molecules, as well as between the generation of reactive oxygen species and antioxidant defenses. 46 The imbalance in n-6:n-3 PUFAs, and associated dysregulation in cellular metabolism and redox balance, can lead to abnormal placentation and endothelial dysfunction underlying a number of disease processes in pregnancy (e.g, preeclampsia, fetal growth restriction, preterm birth, gestational diabetes). 4,47,48
Our study fills a critical knowledge gap in elucidating HIV clinical factors associated with PUFA concentrations and ratios observed in pregnant PWH. This population is at high risk of nutritional deficiencies, making it important to understand whether there are imbalances in n-6:n-3 ratios. However, we could not infer causality from this analysis as we did not have PUFA measures available from early in pregnancy to evaluate changes in pregnancy related to the exposure measures. We also do not know the PUFA concentration prepregnancy. Although we did not assess PUFA concentrations and ratios longitudinally throughout pregnancy, we surmise that PUFA measures assessed in the third trimester would reflect the preceding weeks to months of nutritional exposures, and prior longitudinal studies in pregnancy have demonstrated relative stability of PUFA concentrations and ratios from early to late gestation. 34,49
Overall, the clinical impact of the differences detected in n-6:n-3 ratios remains unclear from this analysis alone. Evaluation of integrated HIV DNA copy numbers in peripheral blood mononuclear cells, which were not available for measurement, may be important areas for future investigation to substantiate our findings. Absence of an HIV-seronegative comparison group represents an additional limitation. We also lacked participants who received integrase strand transfer inhibitors, which limit generalizability to current clinical practice. Future evaluation in this population would benefit from comparison of PI-based therapy, historically associated with lipid and glucose dysregulation, to contemporary regimens. 50
In addition, standardized reference ranges for measuring PUFAs in pregnant PWH remain unknown, and variation in PUFA concentrations may be influenced by regional dietary habits, genetic predisposition, sociodemographic characteristics, and comorbidities. We do not have data on other potentially confounding comorbidities beyond obesity status, but we did adjust for BMI as a surrogate marker for other comorbidities related to metabolic syndrome. Similarly, further evaluation of the association of inflammation, via measurement of inflammatory cytokines, LPS, and TLRs, with PUFA signatures in pregnant PWH would be warranted.
Conclusions
In conclusion, we identified a relative imbalance of plasma n-6 PUFAs relative to n-3 PUFAs in pregnancies affected by HIV. Viremic pregnant PWH have PUFA signatures that exhibit higher n-6:n-3 ratios, reflecting a proinflammatory eicosanoid milieu. Given the complex interplay of HIV infection with pregnancy physiology, longitudinal studies focused on evaluating the effects of these proinflammatory PUFA signatures on perinatal outcomes in pregnant PWH and their offspring are necessary. Future studies should also evaluate the implications of these proinflammatory PUFA signatures on the long-term metabolic health of PWH following pregnancy and their offspring. Finally, interventional trials should also evaluate the feasibility and potential benefits of dietary alterations and/or nutritional supplementation to improve the relative balance of n-6:n-3 PUFA ratios in pregnant PWH.
Footnotes
Acknowledgments
The authors acknowledge the PHACS Metabolic Working Group for their support of this research, and provision of, access to and use of study data for mother–infant/children pairs of pregnant PWH and their HEU infants from the Dynamic Surveillance Cohort in the Nutrition substudy of the SMARTT study protocol.
The authors thank the participants for their participation in PHACS, and the individuals and institutions involved in the conduct of PHACS. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), Office of the Director, National Institutes of Health (OD), National Institute of Dental and Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), and National Heart, Lung, and Blood Institute (NHLBI) through cooperative agreements with the Harvard T.H. Chan School of Public Health (HD052102) (Principal Investigator: George R Seage III; Program Director: Liz Salomon) and the Tulane University School of Medicine (HD052104) (Principal Investigator: Russell Van Dyke; Co-Principal Investigator: Ellen Chadwick; Project Director: Patrick Davis), and through Harvard T.H. Chan School of Public Health for the PHACS 2020 (P01HD103133) (Multiple Principal Investigators: Ellen Chadwick, Sonia Hernandez-Diaz, Jennifer Jao, Paige Williams; Program Director: Liz Salomon).
Data management services were provided by Frontier Science (Data Management Center Director: Suzanne Siminski), and regulatory services and logistical support were provided by Westat, Inc. (Project Directors: Julie Davidson, Tracy Wolbach).
The following institutions, clinical site investigators, and staff participated in conducting PHACS SMARTT in 2020, in alphabetical order: Ann and Robert H. Lurie Children's Hospital of Chicago: Ellen Chadwick, Margaret Ann Sanders, Kathleen Malee, Yoonsun Pyun; Baylor College of Medicine: Mary Paul, Shelley Buschur, Chivon McMullen-Jackson, Lynnette Harris; BronxCare Health System: Murli Purswani, Marvin Alvarado, Mahoobullah Mirza Baig, Alma Villegas; Children's Diagnostic and Treatment Center: Lisa-Gaye Robinson, James Blood, Patricia Garvie, Dia Cooley; New York University Grossman School of Medicine: William Borkowsky, Nagamah Sandra Deygoo, Jennifer Lewis; Rutgers—New Jersey Medical School: Arry Dieudonne, Linda Bettica, Juliette Johnson, Karen Surowiec; St. Jude Children's Research Hospital: Katherine Knapp, Jamie Russell-Bell, Megan Wilkins, Stephanie Love; San Juan Hospital Research Unit/Department of Pediatrics, San Juan Puerto Rico: Nicolas Rosario, Lourdes Angeli-Nieves, Vivian Olivera; SUNY Downstate Medical Center: Stephan Kohlhoff, Ava Dennie, Jean Kaye, Jenny Wallier; Tulane University School of Medicine: Margarita Silio, Karen Craig, Patricia Sirois; University of Alabama, Birmingham: Cecelia Hutto, Paige Hickman, Julie Huldtquist, Dan Marullo; University of California, San Diego: Stephen A. Spector, Veronica Figueroa, Megan Loughran, Sharon Nichols; University of Colorado, Denver: Elizabeth McFarland, Christine Kwon, Carrie Chambers; University of Florida, Center for HIV/AIDS Research, Education and Service: Mobeen Rathore, Jamilah Tejan, Beatrice Borestil, Staci Routman; University of Miami: Gwendolyn Scott, Gustavo Gil, Gabriel Fernandez, Anai Cuadra; Keck Medicine of the University of Southern California: Toni Frederick, Mariam Davtyan, Guadalupe Morales-Avendano; University of Puerto Rico School of Medicine, Medical Science Campus: Zoe M. Rodriguez, Lizmarie Torres, Nydia Scalley.
The authors also posthumously recognize significant contributions by Tracie L. Miller, PhD. Finally, the authors acknowledge Dr. Hannia Campos and the FAs Biomarker Laboratory at the Harvard T.H. Chan School of Public Health for the processing of study samples.
Authors' Contributions
S.A.F.: conceptualization (equal); methodology (equal); visualization (lead); writing—original draft (lead). J.J.: conceptualization (equal); methodology (equal); writing—review and editing (equal). L.M.Y.: conceptualization (equal); methodology (equal); writing—review and editing (equal). L.S.: writing—review and editing (equal). E.G.C.: conceptualization (equal); writing—review and editing (equal); supervision (lead). D.L.G.: conceptualization (equal); methodology (equal); data curation (lead); formal analysis (lead); visualization (supporting); writing—original draft (supporting); writing—review and editing (equal). All authors critically revised the article for important intellectual context. All authors read and approved the final article and agree to be accountable for the accuracy and integrity of this work.
Disclaimer
The conclusions and opinions expressed in this article are those of the authors and do not necessarily reflect those of the National Institutes of Health or U.S. Department of Health and Human Services.
Authors' Confirmation of Consent for Publication
All authors consent to publication of this data.
Ethical Approval and Consent to Participate
Institutional Review Board approval was obtained from the Harvard Longwood Campus Institutional Review Board.
Data Sharing
Data described in the article is not available at this time because of confidential data and current lack of a deidentified dataset.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The PHACS network is supported by the Eunice Kennedy Shriver NICHD, Office of The Director, National Institutes of Health (OD), NIDCR, NIAID, NINDS, NIDCD, NIMH, NIDA, NCI, NIAAA, and the NHLBI through cooperative agreements with the Harvard T.H. Chan School of Public Health (HD052102), Tulane University School of Medicine (HD052104), and Harvard T.H. Chan School of Public Health for the PHACS 2020 Network (P01HD103133). The study authors have no additional sources of funding relevant to this study to disclose.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.