
Abstract
A silent spread of human T cell lymphotropic virus type 1 (HTLV-1) has been occurring for thousands of years, with a high prevalence in some regions due to the sexual and vertical transmission and formation of family clusters. The time from HTLV-1 infection until the onset of virus-associated diseases is extremely long, approximately one to three decades. In this study, we evaluated intrafamilial HTLV-1 transmission and associated diseases in 1,204 individuals enrolled and followed up by the GIPH cohort between 1997 and 2017. The family groups (n = 43) were composed of 279 individuals who were tested for HTLV-1/human T cell lymphotropic virus type 2 (HTLV-2) and were classified as two groups according to the index case: blood donor (blood donors referred to the GIPH cohort) and nondonor (individuals referred to the GIPH cohort by other health services). The observed rates of HTLV-1 transmission and associated diseases among the relatives were high. Of 236 family members and sexual partners tested for HTLV, 104 (44.1%) were confirmed as having HTLV infection, with 36.7% of relatives whose index case was blood donors and 56.9% of relatives with nondonor index cases. At least one case of HTLV-1-associated myelopathy was observed in 42.9% of the families with intrafamilial transmission of HTLV-1. Brazil is an endemic area for HTLV-1/2 and has implemented mandatory universal screening of blood donors for HTLV-1/2 since 1993. However, the lack of public health services offer diagnosis for HTLV to the general population and pregnant women in the country makes it difficult to identify infected people, and contributes to the silent spread of the virus.
Introduction
Human T cell lymphotropic virus type 1 (HTLV-1) is responsible for a chronic infection in humans. The two main routes of HTLV-1 transmission, currently, are sexual and breastfeeding, possibly contributing to the infection rates in families. 1,2 Approximately 10% of infected individuals develop chronic diseases associated with HTLV-1. 3
The diversity of diseases associated with HTLV-1 is characterized by inflammatory (HTLV-associated myelopathy, uveitis, arthritis, polymyositis, and dermatitis) and neoplastic [adult T cell leukemia/lymphoma (ATLL)] processes. 3 The interaction between the virus and immune response of the infected individual seems to determine the predisposition to the development of diseases associated with HTLV-1, as well as their diversity and severity. 3
HTLV-1-associated myelopathy (HAM) is a chronic and disabling disease, generally, with slowly progressive evolution whose clinical manifestations commonly start in the third and fourth decades of the individual's life. Carriers of the disease develop impaired gait, neurogenic bladder and bowel, sexual dysfunction, and low back and lower limb pain. 4 These clinical manifestations demonstrate a topographic anatomical involvement at the thoracic spinal cord level. 5 However, pathological studies have shown that HTLV-1 affects other segments of the central nervous system and peripheral nervous system. 4
ATLL occurs after a long period of infection (four to six decades), with different clinical presentations and severity forms: indolent, chronic, lymphomatous, and leukemic. 6 HTLV-1-associated infectious dermatitis clinically presents as eczematous, chronic, and recurrent skin lesions that occur in body regions, such as behind the ear, cervical, perioral, nasal, and scalp, and are associated with secondary infection by Staphylococcus aureus and/or Streptococcus beta haemolyticus in children and adolescents. 7 ATLL and infectious dermatitis may have a severe outcome of poor prognosis.
The pathophysiology of HTLV-1-associated diseases remains unclear; however, it has been considered that the host's risk factors favor disease triggering. 8 The cohort studies of HTLV-1 carriers are important to understand the outcomes of HTLV-1 infection, whereas the study of family groups allows exploring the means of transmission of viral infection and host factors associated with the risk of transmission and illness. This study presents an assessment of cases on vertical and sexual transmission, prevalence of infection, and development of HAM and ATLL in family clusters of HTLV-1 carriers followed up by the GIPH (Interdisciplinary HTLV Research Group) cohort. Our findings demonstrated a high prevalence of HTLV-1 infection in family clusters and the need for improvement in public health programs to prevent vertical and sexual transmission of the virus.
Materials and Methods
Ethics statement
All procedures performed in the study, involving human participants, were approved by the Research Ethics Committee of the Hemominas Foundation, according to the 1964 Helsinki Declaration and its subsequent amendments. Informed written consent was obtained from all participants included in this study.
Study design
This is a prospective open cohort study.
Study population
The GIPH cohort followed up HTLV-1/2-positive blood donors from the Hemocentro de Belo Horizonte, Fundação Hemominas, Minas Gerais, Brazil, from 1997 to 2017. The relatives of blood donors and individuals referred from other services (nondonor group) with positive serology for HTLV-1/2 as well as blood donors with negative serology for HTLV-1/2 and other infections participated as a control group. The index cases of male blood donors and nondonor denied sexual relations with another man. A total of 1,204 individuals agreed to participate in the study during this period. 9
In this study, only family groups with evidences of HTLV vertical transmission were analyzed. Individuals with HTLV-1 intrafamilial transmission were included in the calculation for prevalence of observed diseases. A family with a history of HTLV-2 transmission was excluded from the calculation of the prevalence of associated diseases as it differed from other families and due to the low prevalence of diseases associated with HTLV-2.
Complementary tests
Testing for HTLV-1/2 was performed using the serological and/or molecular tests. The serological tests included screening tests using enzyme-linked immunosorbent assays (from 1997 to 2011) or chemiluminescence tests (from 2012) and western blot as a confirmatory test. In addition, the molecular in-house nested polymerase chain reaction (PCR) or real-time PCR tests were used to confirm HTLV-1 or HTLV-2 infection. 10 –12
To detect proviral load in blood, the blood was centrifuged at 3,000 g for 5 min to obtain the buffy coat layer and the cell pellet was used to obtain DNA. The DNA was extracted using the QIAamp DNA Blood Kit (Qiagen GmbH, Hilden, Germany) following the manufacturer's instructions. The quantification of proviral load was performed by real-time PCR using SYBR Green. Real-time PCR was performed on the ABI Prism 7300 Sequence Detector System (Applied Biosystems). The proviral charge value was calculated as [(mean number of copies pol/mean number of albumin copies/2)] × 10,000 and expressed as the number of proviral copies/10,000 cells. 13
Analysis of family clusters
We initially identified index cases who had family members tested for HTLV-1/2 to construct the heredograms. Vertical transmission was considered when the mother, sons, daughters, and/or sibling tested positive for HTLV. The family clusters were classified as positive (at least individual with positive result) and negative (all individuals with negative result). In addition, the family clusters were divided according to their index case, such as blood donor or nondonor group (patients who were referred from other services). A pedigree chart was constructed using Progeny Genetics (genetic pedigree and clinical data management software). Figure 1 shows the flowchart of the excluded GIPH cohort members and systematics of the sample studied (Fig. 1).
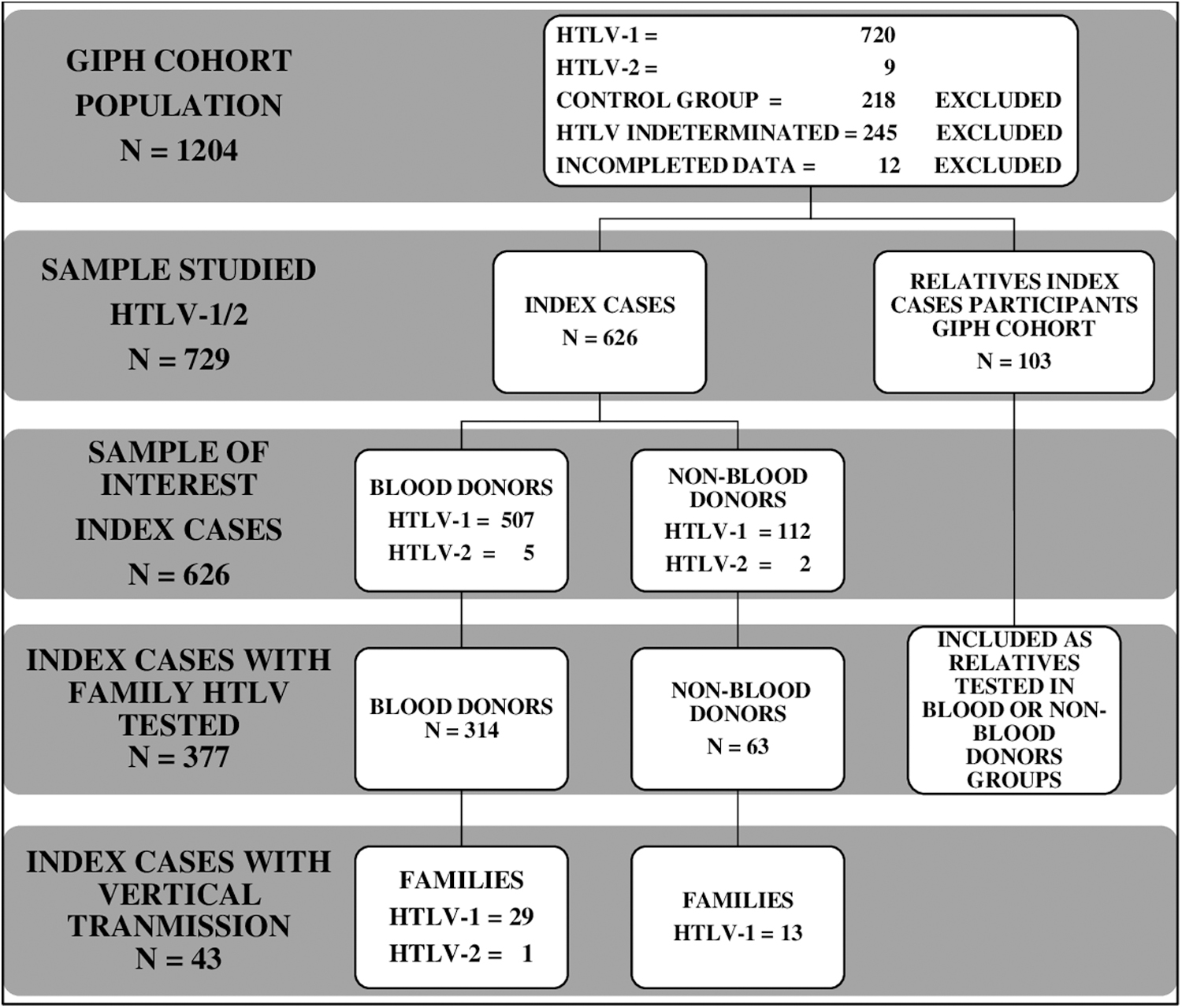
Flowchart of the GIPH cohort members and systematization of the sample studied.
Statistical analysis
The descriptive analysis of the data included the distribution of frequency and percentage of categorical variables. The central tendency measures (mean and median) and dispersion measure [standard deviation (SD)] were described. Comparative analysis between the groups used the t-test for quantitative variables with normal distribution and the Mann–Whitney or Kruskal–Wallis test for nonparametric data. Statistical significance was considered when p ≤ .05. Statistical analysis was performed using the free software foundation PSPP 1.6.2.
Results
Of the 1,204 participants, 720 (59.80%) were confirmed as HTLV-1 positive, 9 (0.75%) were confirmed as HTLV-2 positive, 245 (20.33%) were confirmed as HTLV indeterminate, 218 (18.09%) were included in the control group, and 12 (1%) were excluded because of incomplete data.
We identified 43 families with vertical transmission; 42 (97.7%) had HTLV-1 infection, and 1 (2.3%) had HTLV-2 infection. Among these 43 families, 6 had individuals of three generations who were tested positive for HTLV, and intrafamilial viral transmission through the three generations was evident in 5 (83.3%) families. Figure 2 shows three families infected by HTLV-1 with a high prevalence of associated diseases and the Pedigree chart of family number 37 with transmission of HTLV-1 over three generations (Fig. 2).

Pedigree chart of three families infected by HTLV-1 with high prevalence of associated diseases. One member of family 9 had HAM/TSP and ATLL. Family 37 presented HTLV-1 transmission for three generations. ATLL, adult T cell leukemia/lymphoma; HAM, human T cell lymphotropic virus type-1-associated myelopathy; HTLV-1, human T cell lymphotropic virus type 1.
Among 512 HTLV-positive blood donors and 114 individuals with HTLV referred from other services (nondonors) who were followed up by the GIPH cohort, 314 (61.32%) and 63 (55.26%), respectively, had family members and/or sexual partners tested for HTLV-1/2.
In the family groups, the index cases were predominantly of women, mainly in the nondonor group (Table 1). The index cases of the nondonor group had a higher mean age than those of the blood donor group (p = .03). The mean age at the time of diagnosis of HTLV-1/2 infection of the index cases and their relatives was relatively high (34.69 years; SD: 16.62; 3–70 years). No statistically significant difference was noted in the mean age at the time of diagnosis of HTLV-1/2 infection between the index cases and their relatives (p = .653), males and females (p = .899), and families of blood donors and nondonors (p = .750). The follow-up time of the individuals ranged from 0 to 18.37 years, with mean times of 8.2 and 4.6 years in those of the donor and nondonor groups, respectively (p = .09) (Table 1). Among the index cases, one member of the donor group and the nondonor group underwent only the first medical appointment and did not return for follow-up appointments.
Demographic Data and Follow-Up Time of Human T Cell Lymphotropic Virus Type 1-Positive Blood Donors and Nondonors Considered Index Cases to Constructed Family Clusters
SD, standard deviation.
The index cases with vertical transmission had 236 family members and sexual partners tested for HTLV, of whom 104 (44.1%) were confirmed as having HTLV infection (Table 2). The prevalence rates of HTLV among the tested family members of the blood donor and nondonor groups were extremely high, being 36.7% and 56.9%, respectively. Considering the relationship between the index cases with vertical transmission and the individuals of the blood donor and nondonor family groups, the prevalence rates of HTLV were 44.4% and 62.5% in sexual partners, 36.8% and 44.4% in sons/daughters, and 21.9% and 63.2% in siblings, respectively. Table 2 summarizes data from other family members tested (Table 2).
Ratio of Human T Cell Lymphotropic Virus Infection Among Family Members of Human T Cell Lymphotropic Virus Type 1/2-Positive Blood Donors and Nondonors
All index cases had HTLV-1 infection, except one index case of the blood donor group acquired HTLV-2 infection, his sexual partner and his daughter.
HTLV-1, human T cell lymphotropic virus type 1.
Considering the 42 family groups with HTLV-1-infected individuals, 32 (76.2%) had members with diseases associated with HTLV-1, representing 75.9% (22/29) of the blood donor families and 84.6% (11/13) of the nondonor families (Table 3). HAM was observed in 19 (45.2%) of the total families, accounting for 11 (37.9%) and 8 (61.5%) of the donor and nondonor families, respectively. ATLL was observed only in two (4.8%) of the total families, accounting for one (3.4% and 7.7%, respectively) in donor and nondonor families each. Some families had more than one member with HAM and/or ATLL: family 9 had two members with HAM and one member with ATLL; family 32 had two members with HAM; and family 37 had four members with HAM. The pedigree chart of these families with the highest rate of serious HTLV-1-associated diseases is shown in Figure 2.
Diseases Observed in the Human T Cell Lymphotropic Virus-1-Positive Blood Donor and Nondonor Family Groups
Represents one report and btwo reports from relatives with a clinical picture suggestive of HAM or ATLL.
Other diseases: AR, rheumatoid arthritis; D, depression; F, fibromyalgia; I, ichthyosis; RP, rheumatic polymyalgia; SC, seratoconjunctivitis sicca; U, uveitis; V, vitiligo. ATLL, adult T cell leukemia/lymphoma; HAM, human T cell lymphotropic virus type-1-associated myelopathy.
Table 4 shows the available data of HTLV-1 proviral load of 54 individuals, and for statistical analysis, considered as the highest proviral load quantified during follow-up. The HTLV-1 proviral load levels were not statistically significant on comparing male and female individuals, groups of mothers with positive or negative sons/daughters, positive or negative sexual partners, and families with HAM/ATLL and other disease (Table 4).
Human T Cell Lymphotropic Virus-1 Proviral Load Quantified in Individuals Belonging to Several Family Groups
HTLV-1 proviral load: proviral copies/10,000 cells.
Including HAM and/or ATLL.
Discussion
A silent spread of HTLV-1 has been occurring for thousands of years, with a high viral prevalence in some regions due to sexual and vertical transmission and formation of family clusters. In the endemic region of Argentina, Frutos et al. observed the prevalence of HTLV-1 infection in 31.5% of the relatives of the index cases. 1 A study on HTLV-1 pregnant women observed a prevalence of HTLV-1 infection in 32.6% of the relatives in 43 families. 14 We observed an infection rate of 36.7% among the family members from the blood donor group, which was extremely similar to that observed by Frutos et al. and Mello et al.. However, the rate of HTLV-1 infection in family members from the nondonor group was extremely high (56.9%). Because the percentage of family members tested in the blood donor group was higher (61.9%) than that in the nondonor group (56.3%), the difference in the rate of HTLV-1 infection in these groups should not be due to participant bias but rather due to the characteristics of the groups. The demographic data of the index cases between the donor and nondonor groups did not differ statistically with regard to sex and follow-up time; however, they did differ with respect to the mean age.
The index cases of the nondonor group had a higher mean age, suggesting a longer exposure time to HTLV-1 infection, which potentially influenced the viral transmission and associated disease rates.
The GIPH cohort did a previous study that analyzed the HTLV-1 prevalence in family clusters after 7 years and observed 25.9% of the index cases and their family members tested positive for HTLV-1 infection: mothers (36.6%), sons/daughters (17.5%), and sexual partners (35.9%). 2 This study observed an increase in the prevalence of intrafamilial HTLV infection with the enrollment of new participants and their relatives. Twenty years after the GIPH cohort study, the rate of HTLV-1 infection in family clusters of the blood donors' index cases was mothers (88.5%), sexual partners (50.0%), and sons/daughters (40.5%) (Table 2). The group of the nondonor index cases had an even higher rate of infection in siblings (63.2%), sexual partners (62.5%), and sons/daughters (44.4%) (Table 2).
It is estimated that HTLV-1 vertical transmission occurs in 3,024 cases/year and development throughout life of ATLL and HAM is estimated in 120–604 and 8–272, respectively. 15 Vertical transmission has a critical impact on the outcome of HTLV-1 infection. Bartholomew et al. observed that the rates of HTLV-1 vertical transmission in patients with HAM and ATLL were 33% and 97.2%, respectively. 16 Infectious dermatitis and juvenile HAM are exclusively attributed to vertical transmission. 17,18 These data suggest that HTLV-1 vertical transmission is a more potent risk factor for the development of HTLV-1-associated diseases than sexual transmission.
The risk factors associated with HTLV-1 vertical transmission include breastfeeding for >12 months, maternal proviral load of >100 copies/10,000 cells, maternal age of >26 years, and a history of two or more vertically infected children in the family, noted by Paiva et al. 19 They observed that the mother-to-child transmission rate was 14.2% in 134 families studied; however, seven families concentrated 48.8% of the positive cases, indicating that other factors should also be important to favor vertical transmission. 19 We observed a much higher overall rate (40.5%) of HTLV-1 mother-to-child transmission, 36.8% in the blood donor group, and 44.4% in the nondonor group. This increased rate may be due to the data that were obtained by a cohort study, which allows the occurrence of events over the follow-up time, differing from cross-sectional studies.
A high HTLV-1 proviral load has been associated with the risk of mother-to-child transmission. 19 We observed that infected mothers with HTLV-1-positive sons/daughters or couple with both infected sexual partners had a higher median proviral load than those with negative sons/daughters or couples with only one infected sexual partner, although the difference was not significant. However, we observed a trend of high proviral burden to be associated with the risk of HTLV-1 transmission and disease development. The HTLV-1 proviral load levels were also insignificantly different between family groups that had individuals with or without diseases, including HAM and/or ATLL. The lack of significant difference of proviral load between these comparison groups may be due to the small number of participants with available data.
From the 30 families from the blood donor group, 26.2% had HTLV-1 infection in at least three generations, and 36.7% had HAM or ATLL, which impaired the personal and family's quality life and affects social and economic conditions. This effect may be even more significant in some families with several members that become ill. It was interesting to observe that the blood donor index cases were asymptomatic when they enrolled by the GIPH cohort study. When HTLV-1 infection was detected, however, they already had family members that were sick. Families from the nondonor group had a higher prevalence of HTLV-1-associated diseases (66.7%); perhaps, because they were referred to the GIPH cohort study based on their diagnosis or suspicion of HTLV-1-associated diseases.
Epidemiological studies show a low incidence of diseases associated with HTLV-1. The time from HTLV-1 infection until the onset of virus-associated diseases is, generally, extremely long, approximately one to three decades. However, considering that the majority of investigations on HTLV have been performed from cross-sectional studies or from cohorts with a short follow-up period, the incidence of diseases associated with HTLV-1 may be underestimated. This leads us to consider the importance of follow-up over time for chronic infections, such as those caused by HTLV-1. The incidence of HAM/tropical spastic paraparesis in our cohort was 5.3 per 1,000 HTLV-1-seropositive cases per year (95% confidence interval: 2.6–10.9) at a mean follow-up of 7 ± 4 years. 20 It was interesting to observe that the prevalence of diseases associated with HTLV-1 was significantly higher in some family groups, suggesting that host-associated factors contribute to the outcome of viral infection. The study of family groups infected by HTLV-1 with and without associated diseases can help determine protective or risk conditions.
In conclusion, the vertical and sexual transmission of HTLV-1 is high among families based on our cohort, and it has not declined in the last years. The age at diagnosis of HTLV-1 infection was high and similar in all groups analyzed in relation to sex, index cases and their relatives, and donor and nondonor groups. This fact demonstrates that the majority of infected individuals who are asymptomatic and unaware of the infection are already at reproductive age and at risk of vertical and sexual transmission. Despite the increase in scientific knowledge about the HTLV-1 infection in recent decades, it seems that no impact has been observed in mitigating vertical and sexual transmission of HTLV-1 in Brazilian individuals. More than 40 years after the identification of HTLV-1, this infection remains neglected. The identification of virus carriers by screening candidates for blood donation can be a strategy to identify new carriers by testing their family members and contribute to eliminating the silent spread of HTLV-1. Brazil is considered an endemic area for HTLV-1/2 and has implemented mandatory universal screening of blood donors for HTLV-1/2 since 1993.
Despite this, few public health services in the country offer the diagnosis for HTLV to the general population and pregnant women.21
Footnotes
Acknowledgments
The authors thank all participants and collaborators who contributed to the formation and conduct of the GIPH Cohort.
Authors' Contributions
L.C.F.R.: design of the work; acquisition of data; analysis and interpretation of data; drafting the article; and revising the article. G.G.R.F.: acquisition of data; analysis and interpretation of data; drafting the article; and revising the article. M.A.R.: analysis and interpretation of data; and revising the article. M.L.M.: project administration; supervision; analysis and interpretation of data; and revising the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project was developed with financial resources from the research service of the Fundação Hemominas-Belo Horizonte. The Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG) financed a scientific initiation scholarship for a university student.