
Abstract
Data on persons with perinatally acquired HIV infection in the Caribbean are limited; thus, a chart review was conducted among these clients at an adult HIV treatment clinic in Trinidad over the period January 01, 2011–June 30, 2023. Sociodemographic, clinical, and laboratory data were extracted and analyzed using RStudio version 2021.09.0. Fifty-four study participants were followed up, age range 18–29 years, and there were 27 (50%) males. Eighteen participants (33.3%) were institutionalized until the age of 18 years, while 36 (66.7%) lived with caregivers/relatives and attended outpatient pediatric clinic. The transition from the sheltered environment of pediatric care to the adult HIV clinic was turbulent for some participants as they experienced HIV-related stigma, which may result in poor HIV outcomes. At the initial clinic visit, 28 (51.9%) study participants were virally suppressed (HIV viral load <1,000 copies/mL), which included 12 (66.7%) of 18 who were institutionalized as compared to 16 (44.4%) of 38 who lived with caregivers/relatives (p = 0.387). Data from their last clinic visit showed 31 (57.4%) participants were virally suppressed; 13 (24.1%) were lost to follow-up from care, and there were 6 (11.1%) deaths; 29 (53.7%) were on antiretroviral therapy single-tablet regimens (STRs) and 25 (46.3%) on complex multiple-tablet regimens (MTRs). Institutionalized clients and those on STRs were more likely to be virally suppressed than those living with relatives (p = 0.043) and those on MTR (p < 0.001), respectively. Reported deaths were higher among clients who lived with caregivers/relatives and those on MTR. Participants of younger age were less likely to achieve viral suppression (p = 0.02). Comprehensive programs that include STRs, the engagement of caregivers/relatives and health workers, life skills, and enhanced psychosocial interventions for youths living with perinatally acquired HIV are important to support the transition to adult care and reduce the complex challenges of living with a stigmatizing disease.
Introduction
According to the World Health Organization (WHO), in 2022, an estimated 39 million people were living with HIV (PLHIV) globally, of which 1.5 million were children aged 0–14 years old, 1 many of whom may have perinatally acquired HIV infection, which is classically defined as the transmission of HIV from a pregnant person living with HIV (PLHIV) to their child during pregnancy, labor, and delivery or via breastfeeding. 2 The estimated global rate of perinatally acquired HIV is 3.8% 3 ; however, in the Caribbean, based on the UNAIDS 2023 Epidemiological Estimates, there are 330,000 individuals living with HIV, of whom 1,500 are children aged 0–14 years old. 4,5
Pregnant women living with HIV who receive antiretroviral therapy (ART) and maintain a suppressed viral load (VL) have a risk of vertical transmission of HIV of <1%. 5 –7 The WHO defines viral suppression 7 as having a HIV VL <1,000 copies/mL, whereas the Centers for Disease Control uses a value of <200 copies/mL. 8
A study conducted by Xia et al. 9 among 1,596 persons with perinatally acquired HIV living in New York City showed that 61% of the study population were virally suppressed. 9 There were significant differences in viral suppression by ethnicity and age in the multivariable analysis with Black (59%) patients being least likely to be virally suppressed compared to White (75%), Hispanic (62%), and other races (79%). Additionally, when subcategorized by age, 73% of children aged 0–12 years were virally suppressed, along with 58% of adults aged 20–29 years and 56% of adults aged 30–39 years. 9
A global analysis of 38,187 adolescents living with perinatally acquired HIV among 51 countries, included 903 from South America and the Caribbean. 10 The study highlighted that the mortality rates of perinatally acquired HIV were highest in South America and the Caribbean at 4.4%, but the lost-to-follow-up rates were the lowest at 4.8%. 10 Comparatively, Europe had the lowest mortality rates (0.8%), while sub-Saharan Africa had the highest lost-to-follow-up rates at 13.2%. 10
The Republic of Trinidad and Tobago (T&T) are the southmost islands of the Caribbean and encompass a dual island nation with a population of approximately 1,405,646 persons (2022 mid-year estimate). The ethnic configuration of the population comprises persons of East Indian origin (35.4%), persons of African descent (34.2%), mixed races (23.8%), and 8.4% of other ethnic groups (Asian, European, Middle Eastern). The first cases of AIDS in T&T were reported among gay/bisexual men in 1983, 11 among women in 1985 12 and the first case of pediatric AIDS was reported in 1986. 13 In 1990, Henry et al. 14 studied the first 21 cases of pediatric AIDS in T&T and reported that most children presented to care within the first 12 months of life, the majority were of African origin, and the approximate time between presentation and death was four and a half months. 14 A residential home for orphaned children living with HIV/AIDS (Cyril Ross Home) with a capacity for 35 children was commissioned in 1994 and operated under the auspices of the Society of St Vincent de Paul 15 as parents died with AIDS and family members were unable/unwilling to take care of these children. At the Cyril Ross Home, medical care (treatment of opportunistic infections) was provided by a physician, and the psychosocial needs of the children were provided by the caring staff but unfortunately, there were a large number of deaths among the children as no ART was available. However, in 2002, ART subsidized by the government 16 became available and transformed HIV into a chronic manageable disease. It is estimated that there are 12,000 PLHIV in Trinidad and Tobago and the coverage of people of all ages receiving ART is 60%. 17
There is a lack of data on persons living with perinatally acquired HIV within the Caribbean region, and through this research study, we hope to provide more information on persons with perinatally acquired HIV in Trinidad, their demographics, rates of viral suppression, mortality, and transition to adult HIV care.
Methods
Background
The Medical Research Foundation of Trinidad and Tobago (MRFTT) has approximately 5,130 HIV patients registered in care as of June 30, 2023 and is the largest adult treatment center for HIV/AIDS in the English-speaking Caribbean. 18 Since its formation in 1997, the MRFTT has provided clinical care for persons diagnosed with HIV/AIDS in Trinidad and Tobago, and persons with perinatally acquired HIV infection are referred to the MRFTT from the Pediatric Outpatient HIV Clinics throughout the country once they have attained the age of 18 years. The first patient with perinatally acquired HIV infection joined the MRFTT in 2011. As part of the routine standard of care at the HIV clinic, data are collected on all patients at initial visit using the predesigned pro-forma surveillance form and including sociodemographic information and clinical and laboratory data. Serological tests including HIV VL and CD4 counts are done at initial clinic visits and follow-up visits.
Study design and participants
The MRFTT has an electronic medical records system named CELLMA. A list of patients diagnosed with perinatally acquired HIV who attended the HIV clinic during the period January 01, 2011–June 30, 2023, was generated using CELLMA.
Inclusion criteria
Age 18 years and older
Patients attending the MRFTT with a diagnosis of perinatally acquired HIV infection
Exclusion criteria
Age under 18 years old
HIV seronegative individuals
Patients attending the MRFTT who have not been diagnosed with perinatal HIV infection
Between September 01 and 30, 2023, a chart review was conducted on persons enrolled with perinatally acquired HIV over the period January 01, 2011–June 30, 2023. Demographic information included gender, sexual orientation, ethnicity, employment status, and income level, if participants were institutionalized or lived with caregivers/relatives as children/adolescents, support systems, marital status, number of offspring, condom usage, and ART regimens were gathered from their unique patient profiles. In addition, data were abstracted from client charts to obtain the laboratory records of participants including the CD4 count and HIV VL at the initial clinic visit and subsequent visits. The most recent VL and CD4 counts for each participant were obtained based on the last available records. Each study participant’s current ART regimen was determined based on their last collected prescription.
The study participant’s clinical outcome was categorized as either virally suppressed, virally unsuppressed, deceased, transferred from care, or defaulted from care as defined in Table 1. VLs from the MRFTT laboratory recorded as undetectable are quantitively <40 copies/mL and have been approximated to 0 for numeric variable analysis.
Clinical Outcome Definitions
WHO definition of viral suppression was adopted for viral suppression. 7
Definition derived from the existing medical literature 16 and for the study, a period of 1 month was used to assign participants to this group in addition to having unsuccessful attempts to contact patients via patient tracers.
WHO, World Health Organization.
Data analysis
Data from the electronic medical records were anonymously transcribed to a secure offline data sheet and were then transferred to RStudio version 2021.09.0 for analysis of data.
Summarization of numerical variables was done utilizing mean, median, standard deviation, and interquartile range.
Descriptive analyses were utilized to summarize the sociodemographic variables of the participants about their relevant outcomes. The binary variable for “single-tablet regime” was created for those participants who were noted to be on a regime wherein the ART for a single day equated to one tablet. An additional binary variable was created for whether or not participants were inhabitants of the Cyril Ross Home up till age 18 years.
Analyses were done using the outcomes “Virally Suppressed,” “Transferred,” “Migrated” and a “Nonvirally Suppressed” category created by combining the “Virally Unsuppressed”, “Loss to Follow-up,” and “Deceased” categories. The effect size, test statistic, and its corresponding confidence intervals were included for relationships between variables, wherein a 2 × 2 contingency table was developed. These parameters were omitted for relationships that produced more complex tables.
The Mann–Whitney U test was used to test for the relationship between the continuous age variable and the clinical outcome. The Mann–Whitney U test was selected due to the binary categories of the outcome variable, the likely non-normality of the data due to the limited dataset, and the independence of the observations. 19
Fisher’s exact test was used for the analysis of the categorical variables in light of the low number of expected cell frequencies (having more than 80% less than five observations per cell), limited observations per degree of freedom, and the limited sample size. 20 Post hoc analyses of significant results were not done due to its limitations in evaluating comparisons greater than 2 × 2 tables. Logistic regression was not performed in light of the relatively small sample size and high number of exposure variables.
Results
Describing the population of perinatally infected patients
Over the period January 01, 2011–June 30, 2023, there were 54 adults identified as having perinatally acquired HIV enrolled in care at MRFTT, 27 (50%) males and 27 (50%) females, age range 18–29 years, mean age 23.8 years old (Table 2).
Baseline Characteristics of the Study Population at Initial Visit
Of the 54 study participants, 41 (75.9%) were of African origin, 4 (7.4%) were of East Indian origin, 9 (16.7%) were of mixed race, and 52 (96.2%) self-identified as heterosexual. In terms of level of education achieved, 13 (24.1%) attained a primary school level education and 32 (59.2%) attended secondary school (Table 2). There were 44 (81.5%) study participants who did not complete secondary school as only one (1.8%) person successfully completed a full secondary school certificate and 9 (16.7%) study participants attended tertiary/vocational education. Thirty (55.6%) participants were employed/self-employed [and of these 14 (46.7%) were intermittently self-employed by doing occasional odd jobs], 17 (31.4%) were unemployed, 4 (7.4%) were students, and 3 (5.6%) were receiving Public Assistance Grants from the government. As a result of parents who died from AIDS, 18 (33.3%) of the study participants were housed/institutionalized at the Cyril Ross Home up till the age of 18 years, while the other 36 (66.7%) study participants lived with caregivers/relatives and attended the HIV outpatient pediatric clinics (Table 2). At initial visit to MRFTT, 12 (22.2%) participants were on single-tablet regimens (STRs) and 42 (77.8%) were on multiple-tablet regimens (MTR). Overall, at initial visit to the adult HIV clinic, 28 (51.9%) of the study participants were virally suppressed and 12 (66.7%) of 18 patients institutionalized at the Cyril Ross Home were virally suppressed as compared to 16 (44.4%) of 36 patients who lived with relatives (p = 0.387).
The initial ART regimens in persons with perinatally acquired HIV were lopinavir/ritonavir/zidovudine/lamivudine or nevirapine/zidovudine/lamivudine which were available in pediatric formulations. For those participants intolerant of zidovudine, abacavir was used. In total, 13 different ART regimen combinations using a total of 12 different antiretroviral agents were utilized by participants in this study. Two STRs which are used once daily were available in T&T, efavirenz/tenofovir/emtricitabine, and tenofovir/lamivudine/dolutegravir (TLD) and at their last visit, 29 (53.7%) study participants were on STRs as compared to 25 (46.3%) who were on more complex ART regimens involving MTRs daily (Table 3). Due to drug patency issues, TLD is no longer available in T&T. Of the 29 participants on a STR, 25 (86.2%) were virally suppressed, 1 (3.5%) patient was virally unsuppressed, and 3 (10.3%) were lost to follow-up. Of the 25 patients on MTR, 6 (24.0%) were virally suppressed, 3 (12.0%) were virally unsuppressed, 10 (40.0%) patients were lost to follow-up, and there were 6 (24.0%) deaths compared to zero deaths among patients on STR.
Statistical Analysis of Clinical Outcomes of Adult Patients with Perinatally Acquired HIV by Exposure Variable at Their Last Clinic Visit
Production of a test statistic, effect size and confidence interval are dependent on the variable being binary in nature.
Rank-biserial correlation coefficient.
Indicates significance (p < 0.05).
OR, odds ratio.
In Figure 1, among the 54 study participants at their last visit, 31 (57.4%) of these were virally suppressed, 4 (7.4%) were virally unsuppressed, 13 (24.1%) defaulted from care and were lost to follow-up, and there were 6 (11.1%) deaths (4 males and 2 females), all died with AIDS-defining illnesses. No participants were reported as migrated or transferred from care.
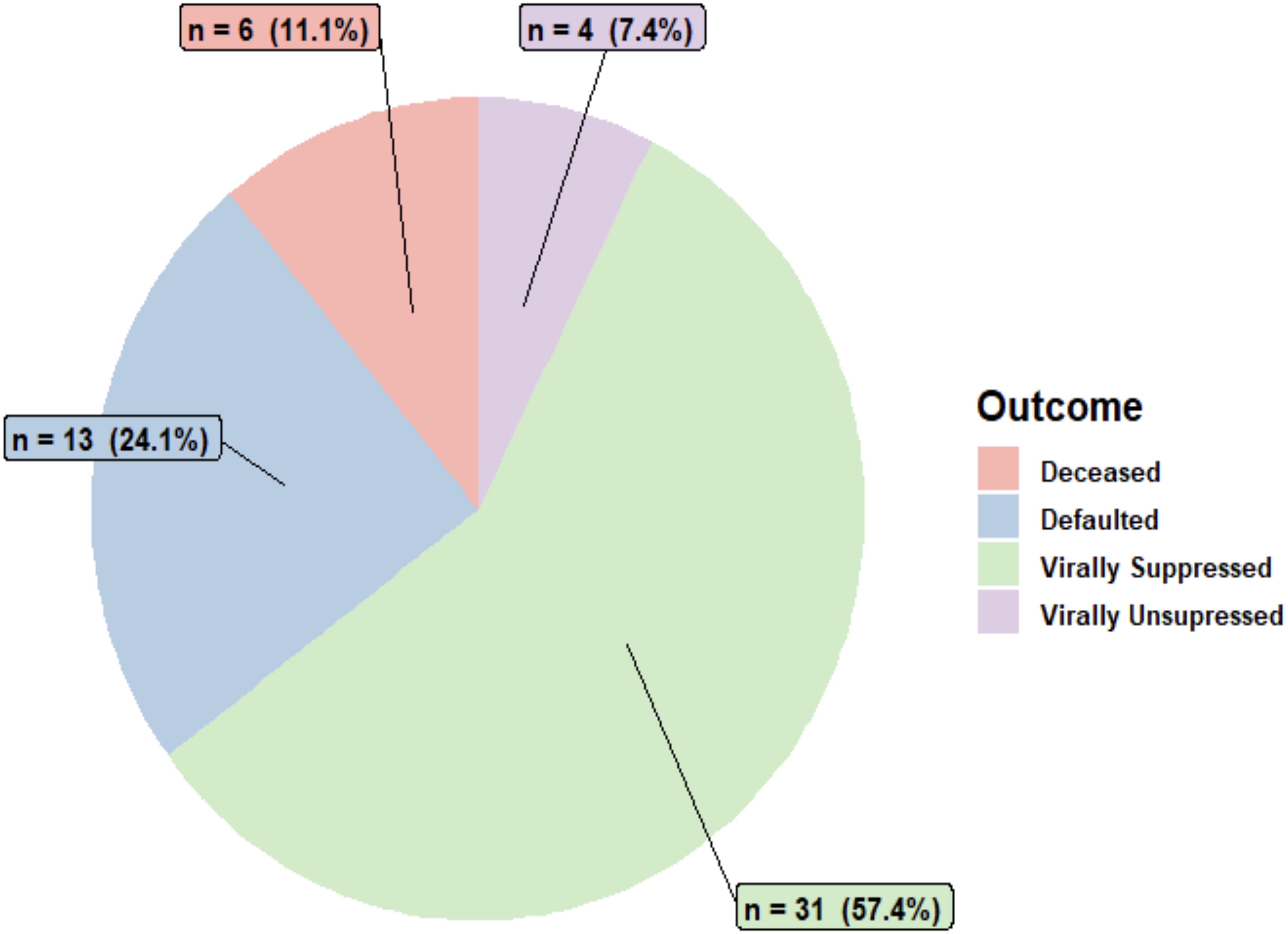
Clinical outcomes of adult patient with perinatally acquired HIV.
Statistical analysis was performed using the previously mentioned exposure variables on the binary outcome categories: Virally suppressed with the combined nonvirally suppressed group (virally unsuppressed, deceased, and defaulted), as seen in Table 3. Test statistics and effect sizes were produced for the analysis of numerical variables and the relationship of the categorical variables was in the form of a 2 × 2 contingency table. Persons who were employed/self-employed were more likely to be virally suppressed than those who were unemployed (p = 0.029). The median participant age in the virally suppressed group was 25.0 years (range 20–29 years) compared to 23.0 years (range 18–29 years) in the nonvirally suppressed group. The participant’s age was noted to be significantly associated with their clinical outcome (U = 288.5, p = 0.01988) with a moderate effect size (r = −0.370).
Of the 29 study patients on STRs, 25 (86.2%) achieved viral suppression compared to 6 (24%) of 25 who were on multiple-tablet/dosage regimes (p < 0.001). Of the 18 patients who were institutionalized at the Cyril Ross Home, 14 (77.8%) were virally suppressed as compared to 11 (30.6%) of 36 patients who lived with caregivers/relatives (p = 0.043) (Table 3). Additionally, all six deaths occurred among patients who lived with caregivers/relatives.
Discussion
Our retrospective study involving 54 adult patients with perinatally acquired HIV from a single center (MRFTT) revealed that at their last visit, 31 (57.4%) achieved viral suppression, 4 (7.4%) were not virally suppressed, 13 (24.1%) were lost to follow-up, and there were 6 (11.1%) deaths. In the Caribbean, eight countries (Anguilla, Antigua and Barbuda, Bermuda, Cayman Islands, Dominica, Montserrat, and Saint Kitts and Nevis) achieved the WHO certification of elimination of mother-to-child transmission (MTCT) of HIV and syphilis. 21 Trinidad and Tobago are working toward eliminating MTCT of HIV, according to the Global AIDS update, ART uptake for pregnant women living with HIV in T&T has increased from 66% at the end of 2010 to 95% by the end of 2021. 22 The Cyril Ross Home currently has only two residents, both under the age of 10 years.
Most of the study participants residing at the Cyril Ross Home maintained viral suppression during their stay at the institution, due largely to the dedication of the caregivers, who ensured that the residents consistently received their daily ART regimes. 23 Unfortunately, the viral suppression for participants who lived with relatives/caregivers and attended the pediatric outpatient clinics was not as good, and a few developed HIV drug resistance and had to switch ART regimens as the children had to depend on parents/relatives/caregivers to give them their daily ART medication, and some of the parents/relatives were poorly adherent with their own ART regimens, and some may not have fully comprehended the importance of adherence to achieve viral suppression.
There was no formal protocol for transition from pediatric care to the adult HIV clinic; however, the youths were informed beforehand that on attaining the age of 18 years, they would have a counseling session with the physician, a call would be made to the MRFTT (the adult HIV clinic) to set up an appointment date with a specific health care provider and a referral letter would be given to the study participant along with a 3-month supply of ART. The youths from the Cyril Ross Home were sent to a Half-Way House for 6–12 months, after which they had to find their own housing. During the transition to the adult HIV care, this was a turbulent period in the lives of these youths as they transferred from the safe space of the pediatric HIV clinic and had to become more autonomous, attend clinic on their own, and assume their own responsibility for adherence to ART. Some of the anticipated barriers in the transition from pediatric to adult care among study participants included anxieties about HIV-related stigma and meeting new health care providers, 24 there may be a feeling of loss of the bond of the pediatric health care provider–patient relationship and there may be apprehension to navigate the health care system on their own. 24 One of the authors (R.J.E.) who was the physician at the Cyril Ross Home also worked at the MRFTT and this may have reduced some of the barriers in the transition to adult care.
After leaving pediatric care, some youths were disengaged from care for periods of 6–12 months before they made the transition to adult care at the MRFTT Clinic due to HIV-related stigma, unstable housing, and alcohol/drug abuse putting them at increased risk for HIV disease progression and transmission of HIV to sexual partners. Overall, at the initial visit to the MRFTT Clinic, 28 (51.9%) of the study participants were virally suppressed, and 12 (66.7%) of the 18 study participants who were institutionalized at the Cyril Ross Home were virally suppressed as compared to 16 (44.4%) of 38 participants who attended pediatric outpatient clinics and lived with caregivers/relatives (p = 0.387). As the youths transitioned from the sheltered environment of pediatric care to the adult HIV clinic, they experienced HIV-related stigma including self-stigma whereby a person may internalize the negative stereotypes and ideas about PLHIV and apply these to themselves resulting in a negative self-image. 25 HIV-related stigma may be exceedingly detrimental to PLHIV as this negatively affects many facets of their quality of life including their social (social support, disclosure), psychological (anxiety, self-esteem, depression), and behavioral components 25 and may result in poor retention in care, nonadherence to ART, and poor viral suppression. Thus, some participants developed HIV drug resistance as demonstrated in the study, where participants were on 13 different ART regimens using a combination of 12 different antiretroviral agents. Strategies to reduce HIV-related stigma include enhanced social and peer support, empowerment and resiliency techniques, the engagement of caregivers/relatives and health workers, psychoeducation, and cognitive behavioral therapy. 25
For those on STRs, 25 (86.2%) of participants achieved viral suppression at their last visit compared to 6 (24.0%) who were on multiple-tablet/dosage regimes (p < 0.001). Our findings were consistent with previous work from Sutton et al. 26 wherein MTRs were associated with lower rates of viral suppression and higher rates of defaulting from care and increased mortality. 26,27 The first-line ART regimen for adult patients attending the MRFTT HIV clinic is the nonnucleoside reverse transcriptase (NNRTI)-based STR of efavirenz/tenofovir/emtricitabine. However, due to the adverse effects in central nervous system, this regimen is no longer considered a preferred regimen. A limited supply of TLD was donated to T&T; however, T&T is considered a high-income country due to its gross domestic product and hence is no longer able to access generic dolutegravir-based regimens due to patency issues. 28 A study of HIV pretreatment drug resistance (PDR) conducted at the MRFTT using samples collected from patients newly diagnosed with HIV infection over the period 2018–2019 found a PDR of 31.3% to any drug and 29.3% to a NNRTI 29 and it was concluded that dolutegravir-based regimens should be the preferred first-line ART therapy in T&T. 29 Another component of the disparate rates of viral suppression relates to the limited availability of drug resistance testing in T&T due to inadequate resources. As a result, when participants are failing therapy, an attempt to achieve viral suppression is made through the provision of complex MTRs that are known to have a higher barrier to genetic resistance; however, these increase the pill burden and have a less favorable side effect profile.
At their last clinic visit, patients who were institutionalized at the Cyril Ross Home were more likely to be virally suppressed (77.8%) than those who lived with caregivers/relatives (30.6%) (p = 0.043). In a study by Meyer et al., 30 29.8% of individuals were virally suppressed on entry to prison and 70% achieved viral suppression during incarceration indicating that HIV treatment may be optimized in a highly structured environment. 30 Baillargeon et al. 31 conducted an analysis of the records of ART fill prescriptions among 2,115 persons released from Texas state prisons over the period 2004–2007 and found that 55% of individuals were virally suppressed at release; however, only 30% of ex-inmates had filled their ART prescription on return to their communities. 31 In contrast, DiPrete et al. 32 randomized individuals awaiting release from prison to an intervention designed to promote postrelease ART adherence and viral suppression versus standard of care in two southern U.S. states. It was found that over 6 months, ART adherence in both study arms averaged about 80%, which was higher than that seen with most chronic noncommunicable disease. 32 Persons institutionalized at the Cyril Ross Home were regimented to take their medications daily (given to them by caregivers), and this discipline to take ART may have become entrenched resulting in greater viral suppression than among those persons who lived with caregivers/relatives. Additionally, all six deaths occurred among patients who lived with caregivers/relatives and those who were on multiple-tablet/dosage regimes.
The study found that there were 30 (55.6%) patients who were employed/self-employed and these persons were more likely to be virally suppressed than those who were unemployed (p = 0.029). Unemployed participants had a comparatively high rate of either defaulting from care, being virally unsuppressed or deceased (combined 70.6%). Those three persons who were unemployed but receiving finances through Public Assistance, conversely had a 100% rate of viral suppression. The Public Assistance Grant in Trinidad and Tobago is provided to meet the needs of persons who are deemed to have inadequate household income 33 and requires the submission of a medical report by a physician yearly for the financial aid to continue and is therefore an incentive for participants to be actively followed up in clinic. This is supported by the findings of a meta-analysis by Petry et al. 34 wherein they concluded that interventions in the form of financial incentives led to improved adherence to medication. 34
There was a statistically significant negative correlation with participant age and viral suppression, as the median age in the virally suppressed group was 25.0 years (range 20–29 years) compared to a median age of 23.0 years (range 18–29 years) in the nonvirally suppressed group (p = 0.02), suggesting that younger individuals are less likely to achieve viral suppression. These results are similar to a study by Weijsenfeld et al. 35 conducted in the Netherlands to determine the virologic treatment outcomes in young persons with perinatally acquired and nonperinatally acquired HIV. In this study, it was found that the adjusted risk for virologic failure was significantly greater among those aged 18–24 years as compared to those 25–29 years of age in both groups of patients, 35 and it was suggested that young adulthood is a period of vulnerability and turmoil that may result in suboptimal adherence and reduced HIV viral suppression. These findings contrast with the study conducted by Xia et al. 9 among persons with perinatally acquired HIV living in New York City, which found that patients aged 22 and 23 years were less likely to be virally suppressed than those who were 20 years of age (in New York City the transition to adult HIV care takes place at 21 years of age). However, similar to our study, this study was cross-sectional, so it was difficult to draw conclusions from the findings, thus further longitudinal studies are important to evaluate virologic treatment outcomes, age-specific interventions, and psychosocial support mechanisms for youths transitioning to adult care.
There were a number of limitations of the study, the small sample size affected data analysis and the study was conducted in a single HIV clinic which would decrease the generalizability of the results The retrospective nature of this study can also lead to challenges in ascertaining the causative relationships between variables.
Comprehensive programs that include STRs, the engagement of caregivers/relatives and health workers, life skills, and enhanced psychosocial interventions for youths living with perinatally acquired HIV are important to support the transition to adult care and reduce the complex challenges of living with a stigmatizing disease.
Footnotes
Acknowledgments
The authors thank the staff of the Medical Research Foundation of Trinidad and Tobago for their support during the study.
Authors’ Contributions
J.E.: Involved in conceptualization, methodology, formal analysis, writing—original draft, and writing—reviewing and editing. G.B.: Involved in conceptualization, methodology, data extraction, and writing—reviewing and editing. N.L.: Involved in methodology and writing—reviewing and editing. S.T.: Involved in conceptualization, methodology, and writing—reviewing and editing. W.S.F.: Involved in methodology, data extraction, and writing—reviewing and editing. E.R.: Involved in methodology and writing—reviewing and editing. R.J.E.: Involved in conceptualization, methodology, data extraction, writing—reviewing and editing, and supervision.
Availability of Data and Materials
The data that support the findings of this study are available from the Medical Research Foundation of Trinidad and Tobago, but restrictions apply to the availability of these data; thus, they are not publicly available. Permission can be requested by contacting the Medical Research Foundation of Trinidad and Tobago.
Ethical Approval
The study protocol and procedures, data collecting instruments, and informed consent form were submitted and approved by the Campus Research Ethics Committee of the University of the West Indies, St. Augustine, Trinidad, approval number CREC-SA.2305/08/23.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.