
Abstract
Introduction:
Gaps between work-as-imagined (WAI) and work-as-done (WAD) have not been studied in biomedical laboratories. WAI takes the form of standard operating procedures (SOPs), and WAD is the way in which work is really done. The workers are often unable to follow the written procedures exactly. They will realise that they have degrees of freedom to perform tasks, and as they get more experienced, they will have more choices based on practice and know-how.
Methods:
Fifteen workers were interviewed to explore gaps between WAI and WAD. Participants were also asked how they assessed if the deviations they made were able to ensure safety and productivity and the best way to learn safe work in the laboratory.
Results:
Participants did not always follow the SOPs exactly, which resulted in gaps between WAI and WAD. All participants did a “on the spot” mental risk assessment and deviated from SOP based on that. They were able to discern the high-risk steps that they strictly followed. The most common reason for the gaps were work pressure and time constraint, especially in time-sensitive procedures with precious samples and reagents.
Conclusion:
Concepts like WAI and WAD and the inevitable gaps between them are new in the biomedical laboratories. Such gaps need to be identified, assessed, and addressed to ensure safe work. Organizations need to make safety SOPs relevant and ensure that the workers are consulted when developing SOPs. Some local variability is inevitable, and these skills can be strengthened by open communication and interactive safety training methods.
Introduction
The way humans work has been described in four varieties, namely work-as-imagined (WAI), work-as-prescribed, work-as-done, and work-as-disclosed.1–4 WAI is what is imagined and written by policymakers, senior management, middle management, and others. These take the form of standard operating procedures (SOPs) and work instructions. Work-as-prescribed comprises formal laws, regulations, and rules, by which the correctness of work done is judged. Work-as-done (WAD) is the way in which work is really done, and work-as-disclosed is what workers are willing to describe about the way work was done. WAD is characterized by the trade-offs and compromises that the workers make all the time, depending on the work conditions, taking into account both safety and productivity. 5 WAI and WAD have been described and studied in a variety of industries including healthcare,1,6–8 aviation, 9 and other industries.10,11 WAD is highly dependent on the local situation, if nothing goes wrong, the gaps between WAI and WAD are not even visible, and productivity is rewarded. When something goes wrong, however, these become glaringly visible, and investigations often blame the fact that written rules are not followed exactly. As a result, additional rules are often imposed. This in and of itself can create conditions that are new threats to safe work. 12
Safety in biomedical laboratories is managed through a Biorisk Management System (BMS)13,14 that addresses biosafety and biosecurity. There is an ISO standard (ISO 35001:2019) 15 devoted to biorisk management and guidance documents that are widely used in all regions of the world. These include World Health Organization Laboratory Biosafety Manual 16 and Biosafety in Microbiological and Biomedical Laboratories 6th Edition published by the Centers for Disease Control and Prevention. 17 These standards and guidance documents emphasize the need for risk assessment and the identification and implementation of suitable and sustainable risk mitigation measures as a core part of the BMS. Most biomedical laboratories develop their BMS based on these guidelines and standards alongside whatever national legislation and regulations are applicable.
A fundamental purpose of a BMS is to contain the risk posed by biological material in the laboratories through biocontainment. Biocontainment is a combination of primary and secondary barriers, design of facility infrastructure and air handling units, facility practices and procedures, and safety equipment, including personal protective equipment (PPE).18,19 SOPs and work instructions are a key part of ensuring safety and productivity as part of the containment principles to ensure that workers and the environment are protected.
Workers are often unable to always follow the written procedures exactly, based on the local work situations that they encounter. As they get more experienced, they will have more choices in performing them based on practice and know-how. Vijayan and Smoker
5
used the Rasmussen model to study how work is done in a biomedical laboratory and reported that the workers are aware of the risks and manage the tensions and trade-offs by using the following methods in various combinations to remain safe and productive:
Performing dynamic mental risk assessment to omit certain steps from the SOPs Working in teams, planning and coordinating the work processes in advance Using their experience and familiarity with the work processes Making trade-offs and sacrificial decisions
Dynamic mental risk assessment is an on-the-job continuous process of assessing risk as they occur at the workplace so that workers can address the risk and proceed to work safely20,21 This type of mental risk assessment is termed “Dynamic Mental Risk Assessment” and has been used in industries with complex and dynamic work conditions.
These trade-offs and adjustments lead to gaps between WAI and WAD, which has been studied in many industries. One study in petrochemical industries 22 suggests a classification of the gaps into “safety-critical, routine, and efficiency,” with the safety critical ones being reinforced to ensure that there is no noncompliance. In some situations, it may be necessary to make changes to the SOP, in others is may be a question of how much variability should be allowed and how it should be communicated to the workers.23,24 In the field of biorisk management, these local gaps (variability) between WAI and WAD have not been studied. This study aims at understanding the gaps between WAI and WAD in biomedical laboratories, the rationale of why the workers made the deviation and how the deviation is handled.
Materials and Methods
Study Setting
This study was undertaken among workers in biomedical laboratories with 13 participants from Southeast Asia, one from South Asia and one from Europe. The participants were from research or diagnostic laboratories involving human or animal pathogens. The participants were laboratory heads, laboratory workers (lab technician and research assistant), and post-doctoral fellows who work with infectious agents in biosafety level 2 laboratories.
Data Collection
Fifteen participants from the authors’ network were recruited via convenience sampling. The participant pool comprised nine individuals from public university research laboratories, five from public diagnostic laboratories, and one from a private research and development facility. Participants were recruited via email or WhatsApp and provided with information regarding the study’s aims and interview questions. Verbal consent was obtained prior to the one-time virtual interview, which lasted 45–60 min. Interviews were audio-recorded with participants’ consent, and all recordings were subsequently transcribed, anonymized, and stored in encrypted electronic format.
This study used the one-on-one semi-structured interview method using key questions and topics (Table 1) to understand and explore the participants’ opinions and experiences. The semi-structured method gave the interviewer an opportunity to follow-up on the participants’ experiences and knowledge to pursue related topics. It also allowed the discovery of information, which may be important to the participant, but was not known to the interviewer prior to the interview thus allowing the interviewer to explore other dimensions of the research question.25,26 Each response from the participant was used as an opportunity by the interviewer to probe further and to get in-depth information about the participant’s views. Participants were asked to draw from their entire biomedical work experience, regardless of country or institution, and not limit their answers to the current laboratory.
Interview questions
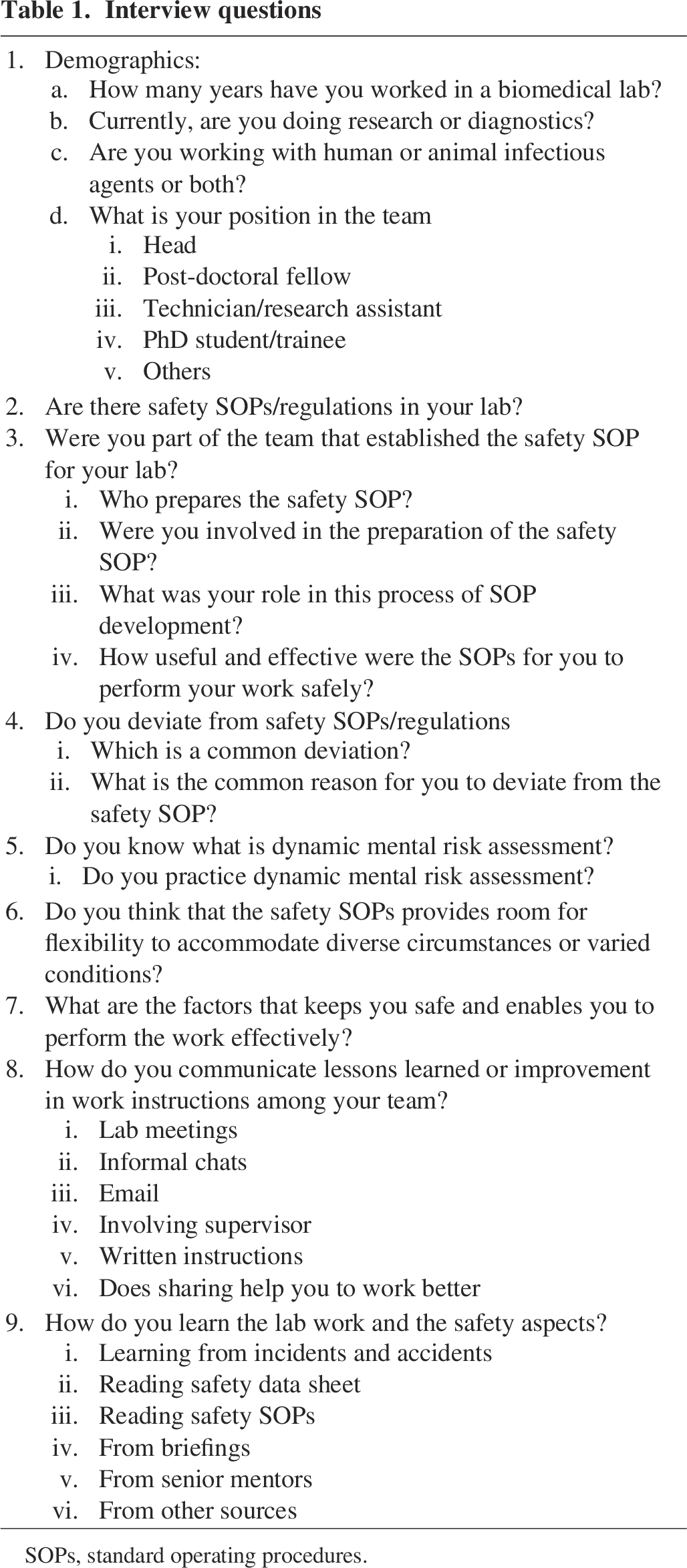
SOPs, standard operating procedures.
Thematic analysis was performed by exploring all the responses and identifying common themes and subthemes described in results section.27–29 All the participants were not asked the exact same questions; therefore, some responses do not total to 100%. On the other hand, some questions, e.g., “Do you read safety SOPs” yielded responses from all the participants and the response totalled to 100%. As the aim of this study is to understand the relationship between WAI and WAD in a biomedical laboratory; identified themes and subthemes were mapped onto the research question. This was done by reviewing the data several times and then coding them such that patterns become discernible. The coded data were used to identify and characterize the factors that described the relationship and gaps between WAI and WAD.
Results
Demographics of the Participants
The participants included seven laboratory heads, five laboratory workers, and three post-doctoral fellows. Their years of experience in biomedical laboratory was 14–30 (average 22), 4–30 (average 11), and 8–18 years (average 11), respectively. All participants at the time of this study worked with infectious agents, 13 with infectious agents affecting humans, and two with those affecting animals. Ten participants were in research, four diagnosis and one a combination of research and diagnostic work.
Standard Operating Procedures
Biomedical laboratories, both diagnostic and research, have written step-by-step work instructions on how to perform the procedure for diagnosis or research. As opposed to work instructions, safety SOPs are developed by the organization’s Environment, Health and Safety Departments (EH&S), participants’ department or laboratory as part of the BMS. Only six participants had an organizational level EH&S, who prepared the safety SOPs, the rest was prepared locally at the laboratory or departmental level. Fourteen participants said that safety SOPs were not integrated into the work instructions. The one participant in whose laboratory safety SOPs and work instructions were integrated said that the work instructions had references to the safety SOPs so that they would know at each step if any additional safety practices were required. Five participants said that the laboratory workers were consulted when developing the safety SOPs the rest said that it was developed by the safety department or supervisor without consultation with the laboratory workers. The participants each had very different understanding of how to integrate safety SOPs into the experimental/diagnostic work processes. One diagnostic laboratory had only a few written instructions for performing their work and no safety SOPs. Staff in this laboratory relied on word of mouth conveyed through the senior staff, and the instructions were committed to memory.
As this study is aimed at understanding the relationship and gaps between WAI and WAD solely for safety SOPs, the interviews did not focus on the gaps between WAI and WAD for the experimental/analytical work instructions. When participants were asked, whether they read the safety SOPs, eight out of 15 (53%) said that they did not because they did not find it useful. The remaining seven (47%) said they did read them. One participant who did not read the SOPs said, “I am very experienced and there are certain unnecessarily complicated things [in the safety SOPs]”. Of the seven who read the safety SOPs, two read them because there was a written assessment, four because they were involved in preparing them, and one because they wanted to get ISO accreditation. All participants said that safety SOPs should be practical and that input from laboratory workers should be obtained when writing the SOPs. In particular, the following responses are worthy of attention:
“Safety rules are made by people who don’t understand lab work for example the need to wear eye protection when working at Biosafety Cabinet (which already has a glass barrier)”.
“Depending on the reasonableness of what is in the (safety SOP), I will follow”
“Very precise safety SOPs are not good; people have slightly different ways of doing things”
“Hard rules for some (parts) and not hard rules for some (parts) is better”
Gaps between WAI and WAD
All participants deviated from the written safety SOPs (WAI), which resulted in gaps between WAI and WAD. All participants did a mental risk assessment on the spot and made deviations to the SOP based on that mental risk assessment, these were never written down. There was a wide array of practices with one (7%) participant saying that very few rules were followed in their laboratories and three (20%) saying that the workers followed the rules very strictly. The rest (73%) were somewhere in between, where the participants used mental risk assessment to make decisions. It is also worthy to note that the three laboratories where the workers followed the rules strictly had consulted the workers in preparing the SOP.
Work where no gaps between WAI and WAD were seen.
All participants strictly followed the SOP for the following work:
Use of biosafety cabinet (BSC) for all work with infectious material Stock virus handling Biological material inventory maintenance, when it was required Waste management Sharps disposal
Work Where Gaps between WAI and WAD Were Seen
Use of PPE
The minimum PPE in these laboratories consists of laboratory coats, gloves, and covered shoes. All the participants wore the minimum PPE when working in the laboratories with no deviations. In a few laboratories, additional PPE consisting of safety glasses or surgical masks were included in the SOP. They wore a surgical mask and safety glasses based on their individual mental assessment, for example, if they were working with airborne virus some workers wore a surgical mask. The reason for not following the additional PPE requirement was cited as discomfort, and they were not convinced that it was needed. Participants said they worked at the BSC (which has a glass sash), and the additional PPE prevented them for working quickly and comfortably.
Only one laboratory had a requirement to wear N95 mask even in BSL2 laboratories. The participant from this laboratory, who held a supervisory role, said that the workers were fit tested, and the N95 requirements was included by the biosafety committee. This participant explained as follows:
“When they have to adjust the metal band on their nose, they feel that this is uncomfortable, so they use the N 95 but they don’t use it in the correct way. Because they know the pathogen is very low hazard for them, for example E coli or other pathogens in the risk group 2. If they work with in BSL-3 laboratories, they all have higher level of compliance and they follow the SOPs very carefully. Most of the deviation in the SOPs occur in the BSL 2 laboratory”.
Use of centrifuge safety cups
Biomedical laboratories use centrifuges for their work, and the safety SOPs require the workers to use a special safety cup while centrifuging and to open the safety cup within the BSC. Participants used their own mental risk assessment to see if the infection was aerosol borne or vector borne, for the latter they did not use safety cup. All participants who deviated said that they use good-quality centrifuge tubes and surface disinfected them before taking out of the BSC. All the participants deviated because using the safety cup took longer to complete the work. Participants used their own mental risk assessment based on the speed of the centrifuge, viral concentration, and whether the infectious agent was airborne, or vector borne. Two said that the safety cups were not always available due to funding restrictions, but the SOPs mentioned them.
Sample transport
The safety SOPs contain an overall statement that all infectious agent containing material must be transported within or between laboratories in double containment, i.e., a primary container, usually a test tube to hold the biological agent and a leak-proof secondary container to contain the primary container. The SOPs further stated that for transportation outside of the institution, double or triple packaging must be used based on the route of movement and the material being transported. Participants explained that within the laboratory, they would carry infectious material in test tubes, microtiter plates, or culture dishes, which were placed in an ice box which was not leak-proof. However, no one omitted the ice box because they wanted to keep the temperature of the material stable for the success of their work. The explanation given was that it was time consuming and not necessary based on their mental risk assessment. All participants also used the correct triple-packaging if they transported the material externally, there was no deviation in this.
Participants gave the following explanation for this deviation between WAI and WAD:
They used screw cap centrifuge tubes, which they would tighten before they moved the tubes anywhere They used a Styrofoam box filled with ice as the secondary container, which they would tape if they were moving to another laboratory or in the lift Their laboratory was small, and distance between the BSC and freezer or incubator was just a few steps away. One participant said it would depend on the virus whether it was aerosol-borne or vector-borne transmission Two participants said that they did not have a secondary container due to funding shortage However, most participants said they would use a leak-proof secondary container if they transported infectious material in lifts or across buildings
Use of fume hood for working with volatile chemicals
Participants had access to a fume hood (device with exhaust ventilation that is designed for working volatile chemicals), which was usually placed in a central location for all laboratories to access. All participants did a mental risk assessment to evaluate the need to use the fume hood, based on the chemical, the quantity and the distance they needed to travel with the chemical bottle. If they felt that they could open the chemical on the laboratory bench because the quantity was small and the chemical was not high risk, they would do that. One participant said that they used the fume hood because co-workers would be displeased if there was any odor. To prevent this, they would walk all the way to the fume hood, even if they felt it was not commensurate with the risk.
Incident reporting
The definition of incidents was adopted from the U.S. Department of Labor Occupational Safety and Health Administration (OSHA). OSHA uses the term “incident” for all events where a worker was hurt, as well as close calls (sometimes called “near misses”). 30 Incident and near-miss reporting had a wide range of practice. In three laboratories where workers were consulted in preparing the safety SOPs, worker feedback as well as incident reporting was also encouraged, and workers did report incidents. Two participants from these laboratories, who held supervisory positions, said they had a system that at least 10 incidents should be reported every month, and each one was addressed with a strictly no-blame culture. The remaining 12 participants said that they would report only serious incidents. Seven of them said that reporting resulted in blame, and they would not report. The one laboratory with no written SOPs also did not have any system to report incidents.
Reasons for gaps between WAI and WAD
The most common reason for deviating from the SOPs is work pressure and time constraint (Figure 1). Participants had to ensure that the experiment was not jeopardized, especially in time-sensitive experiments with precious samples and reagents. In addition, participants chose convenience and the path of least effort, and if this worked and nothing untoward happened, they were likely to do it again. As they gained more experience, they would also omit steps that they thought were unnecessary and were not commensurate with the risk. This indicates that they relied a lot on their own mental risk assessment. None of the participants were familiar with the term Dynamic Mental Risk Assessment;20,21 however, based on the responses obtained, they were all using it to make an assessment and decision to deviate from the written SOP.
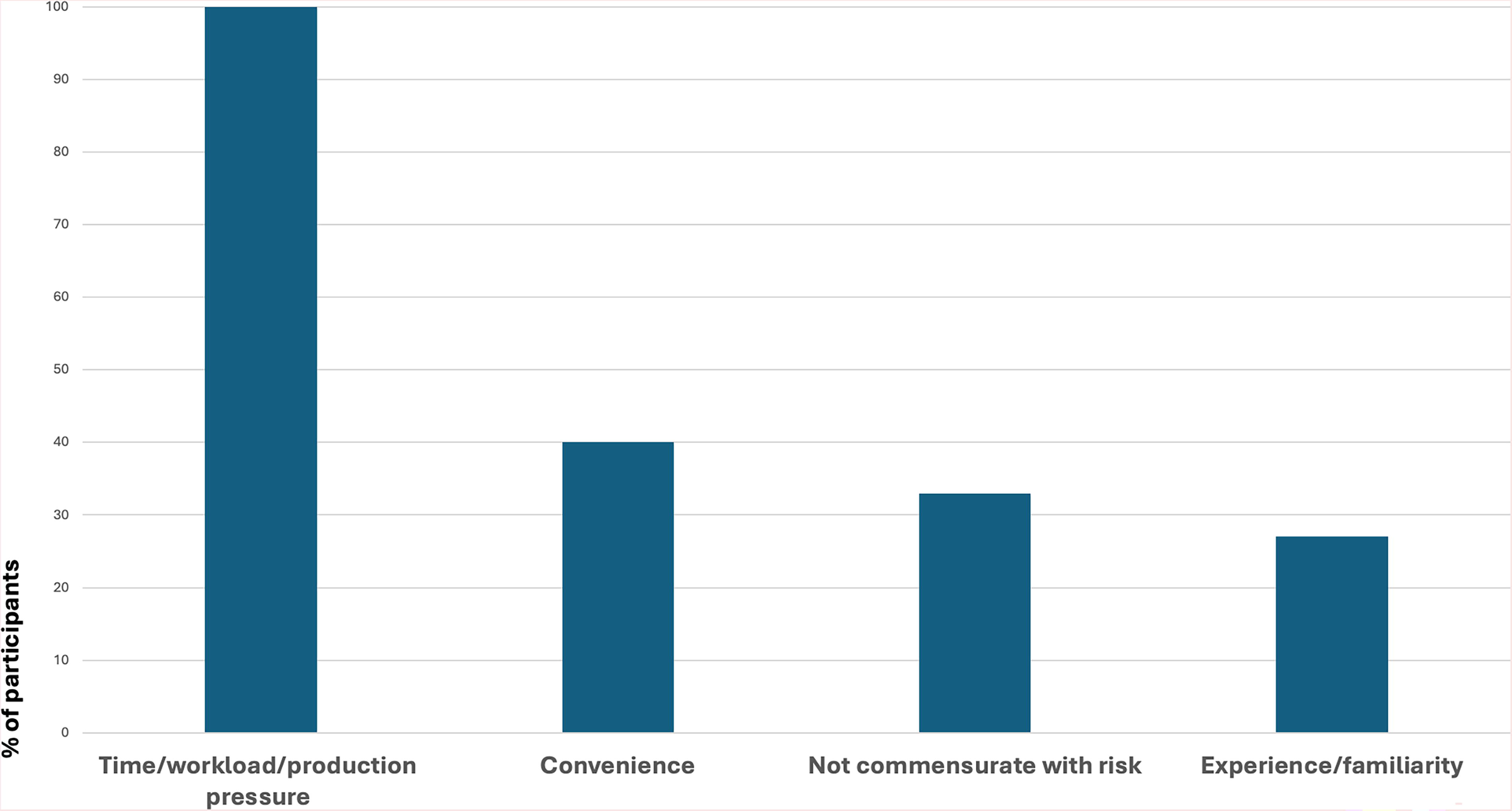
Reasons for gaps between WAI and WAD. WAD, work-as-done; WAI, work-as-imagined.
One participant who was a laboratory head said that the step the workers always deviated was contact time for disinfectants. When questioned further, the participant said that the contact time mentioned in the SOP was one hour, even though based on the product specifications it is only 10 min. The workers in the laboratory brought this up to the supervisor (study participant) who took it to the biosafety committee, but it was not changed to the lower contact time. The participant accepted that this was a step that was often not followed, and this remained a gap between WAI and WAD.
Addressing gaps between WAI and WAD
All participants felt that the safety SOPs at the organization level should be generic, with the laboratories having safety SOPs that are specific to their work. The generic SOPs they said should not be repetitive, be in simple point form, and consist of all the mandatory steps that need to be followed. The participants said that mandatory requirements need to be clear and that there should be a consequence for not following them. All participants felt that safety precautions should be written as part of the experimental procedure so that at each step they would be reminded of how to perform it safely. This would make the safety SOPs relevant to the laboratory worker. Only one of the laboratories had the safety SOPs integrated into the work SOPs; all others had them separate. All participants felt that variability will exist and need not be written down but discussed informally when needed. One participant felt that the only significant variability they would encounter is in the work/experimental procedure and not in safety procedure. Participants also felt that worker consultation in developing the safety SOPs and an open communication channel with no assigning of blame would help learning of best practices.
Methods of learning and skills acquisition
Thirteen participants said that some formal safety training was provided either through their own department or EH&S. However, learning was predominantly achieved through their seniors and by doing the work themselves. Learning from their seniors was the most important method of skills acquisition as shown in Table 2. Only three said they learned from safety SOPs and one from safety training. 47% participants said they learned from information about accidents and incidents that happened to others and 20% said that they learned from others pointing out their mistakes. Regarding mistakes, 83% participants said they learned from their mistakes and 13% said that if they got away with the mistake, they would do it again. When probed further about learning from incidents and accidents, the main reluctance appeared to be the assigning of blame that came with incident reporting and communication about incidents. One participant who is a supervisor said:
Methods of learning and skills acquisition
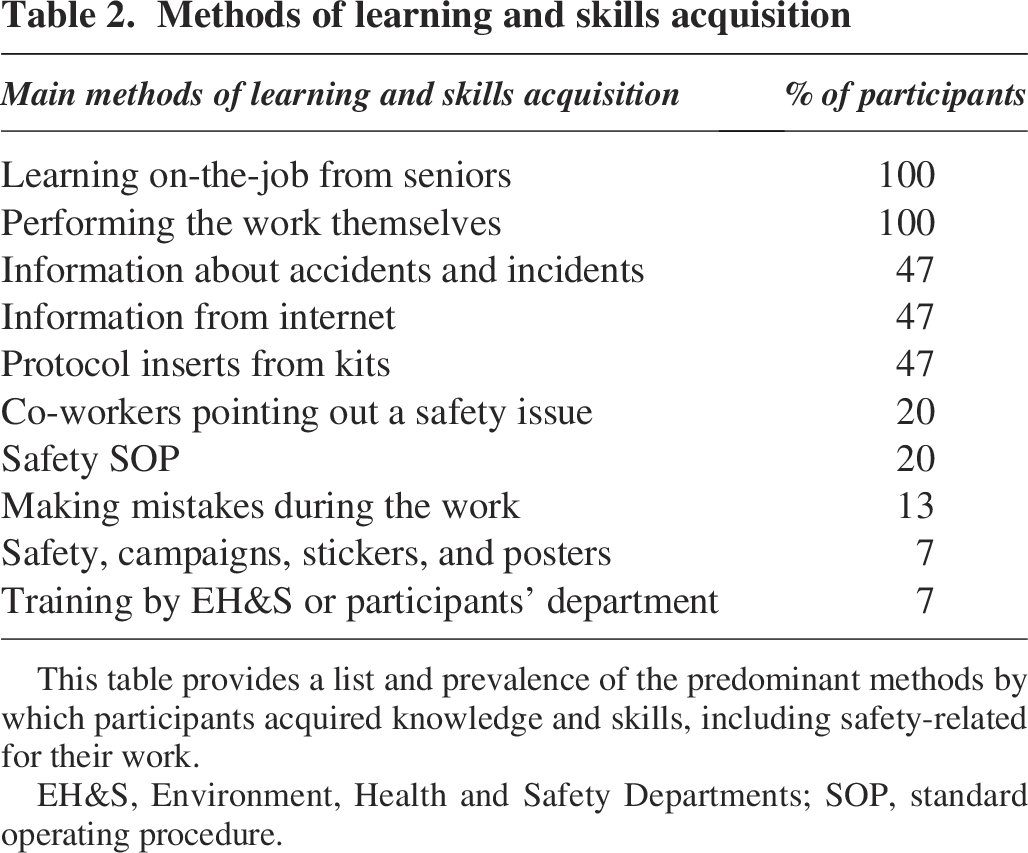
This table provides a list and prevalence of the predominant methods by which participants acquired knowledge and skills, including safety-related for their work.
EH&S, Environment, Health and Safety Departments; SOP, standard operating procedure.
“When I was a junior the system in our institution was a blame system. I grew up in that kind of system where they blame you instead of correcting you or mitigating the problem so that’s why in the course of my career here, I advocate the blame-free system and we encourage incident reporting not to blame them but to mitigate the situation and to learn”
All participants felt that information sharing was the best way to learn skills and to do their job better. When asked if sharing helps to be safe, 83% said yes and the remaining did not have any opinion. Among those who felt that sharing helps, 95% felt it should be done informally and only one said that it should be written.
Discussion
This study shows that the laboratory workers do not always read the safety SOPs because they do not find it useful. They said that the SOPs are repetitive and contain information that is not relevant to them. Based on published literature, this is not unique to biomedical laboratories.24,31 Perhaps the SOPs are too prescriptive, for example, the use of a leak-proof secondary container to move infective samples a short distance within the laboratory and additional PPE that is not the normal practice in many BSL2 laboratories. All the participants used mental risk assessment to assess the need for a leak-proof secondary container during transport of infectious material. They took into consideration the type of virus, the route, and distance of the movement. This type of mental risk assessment is termed “Dynamic Risk Assessment” and has been used in industries with complex and dynamic work conditions.20,21,32
All participants understood the need to use a BSC, which is the single most important primary containment equipment in biomedical laboratories. One participant said that if they were working with an infectious agent that was not aerosol transmitted but perhaps transmitted by a vector like mosquito, they would still use the BSC, but the reason would be to protect their samples from cross contamination rather than themselves. Such arguments and explanations of their work process show clearly that participants do understand the risks and use their on-the-spot mental risk assessment to decide whether to deviate from the written safety SOPs. Abbott and De Lange 33 studied this gap between WAI and WAD in aviation and found that such gaps can never be eliminated. The authors interviewed 16 cockpit crew to understand under what circumstances a gap between WAI and WAD arose. Based on the data, they suggest a “rule management framework,” which was built upon an earlier paper on rail transportation safety. 34 Such a framework can be combined with ideas from Ashraf et al. 22 who studied gaps in WAI and WAD in petrochemical industries. The authors suggest classifying the gaps into categories based on their potential to produce negative outcome so that they can be addressed appropriately. Figure 2 is an adaptation of this framework that organizations can use to better understand the gaps between WAD and WAI in laboratories and turn them into learning experiences.

Suggested framework for addressing the gaps between WAI and WAD. WAD, work-as-done; WAI, work-as-imagined.
While local variability is welcomed in a resilient organization, it does not include human error and safety critical protocol drift because these have the potential to lead to negative outcomes. 22 One such practice termed normalization of deviance was coined by Dr Diane Vaughan 35 a sociologist, who identified this phenomenon during the Challenger disaster in 1986. She writes that over time, deviations become the norm, and everyone just follows the deviation leading to catastrophic accidents. This is especially important in the biomedical research laboratory as the workers learn from their seniors who may themselves be deviating from SOPs. It is therefore essential to question whether laboratory workers are sacrificing safety for faster and more efficient work processes. Rules are essential, but local variability will always exist and needs to be managed. 36
Traditionally, the role of EH&S departments has been to develop safety systems and ensure compliance. In this study, only five participants said they were consulted in developing the safety SOPs in fact, consulting laboratory workers in developing SOPs is not the prevalent practice in many regions (personal observation). While it is the role of safety staff to ensure compliance to written SOPs, they could take a more collaborative approach in trying to understand why workers deviate from SOPs and to work as a team to resolve them. Bautista-Bernal et al. have studied safety culture and performance in different industries. They conclude that some flexibility and collaborative identification of new solutions that do not compromise safety and productivity need to be encouraged and can produce best results. 37
Majority of the participants in this study said that they would not report or talk about any incidents or mistakes because they are associated with blame. Here, it can be useful to consider the idea of “just culture” where incident reporting and learning from incidents do not include assigning blame, unless the act was intentional with a malicious intent.38–41 The aviation industry has incorporated just culture into its management of compliance. These are the lessons to be learned by those working with biological hazards as explained by Snyder et al. 42 These authors promote a “just culture” that combines top-down and bottom-up approach. In the current study, laboratories where workers were consulted in developing the SOPs were also the ones where incident reporting without blame was encouraged. It requires a holistic approach to the way safety is managed throughout the organization.
From this preliminary study, it is clear that learning from seniors is the most prevalent knowledge transfer and skills acquisition method. Literature search did not yield any papers specifically on mentoring in biomedical laboratories, but one paper by Hill et al. 43 has looked at healthcare in general. The authors explained that qualities of the mentor–mentee relationship are crucial in ensuring competency and that it is an ongoing process that does not end with the initial training. In laboratories, there is reliance on initial safety training and on-the-job mentoring, but the mentors are not given any training or guidance on being a good mentor. Programs where the senior staff are given training on being a good mentor has provided positive results in rail transportation and healthcare settings.43,44 More research is needed to design robust and sustainable mentor training and mentorships programs in managing laboratory biorisks.
This study is a follow-on to another study conducted by the current author where the Rasmussen model of boundaries was applied to a biomedical research laboratory. The authors observe that resilient performance cannot be achieved by simply adding more rules to deal with every situation but by providing the right tools and knowledge to deal with everyday situations. 5 This study and the previous study show that the laboratory workers are capable of using mental risk assessment and their experience and expertise in addressing a variety of work situations. Tresfon et al. 4 used the Functional Analysis Resonance Method to understand WAI and WAD in a hospital ward. The authors report that the use of this methodology gave the workers opportunities to reflect on the deviations and work-arounds collectively as part of the study. One notable finding in this study was that the gaps between WAI and WAD were used to rewrite the SOPs, reduce the number of pages in the SOPs, and change the narrative to a more friendly and helpful tone instead of a prescriptive tone of voice. Weenink et al. 45 examined the gaps between WAI and WAD in hospitals and explain that the reasons for these gaps should first be examined. In their study, the scepticism of the staff in accepting the process as necessary and time constraints were some of the causes, very similar to results of this study. The current exploratory study shows that there is local variability in laboratory work processes and supervisors need to discuss and explain the rationale behind regulations and allow the workers to give their opinion before it is written into SOP. More research is needed to understand WAI and WAD gap in biomedical laboratories and to adopt newer concepts of safety to ensure that the gaps are addressed and minimised so that these deviations do not become normalized.
Conclusions
Organizations need to make safety SOPs relevant and practical to laboratory workers and ensure that the workers’ input is integrated into the development of such SOPs. Safety SOPs should be part of the work process so that productivity is not compromised, thus ensuring that workers will follow most of the SOPs. Some local variability is inevitable and such skills can be strengthened by open communication and interactive safety training methods. These concepts are very new in biorisk management, but it is time to include them to manage risk in a practical and effective manner.
Limitations
The cohort studied is very small, and more research is needed to better understand and address the gaps for safer and productive workplace. However, it is a first step to identify that there are gaps between WAI and WAD that need to be studied and addressed.
Ethical Approval
The Parkway Independent Ethics Committee has approved this study (reference number PIEC/2024/52).
Authors’ Contributions
Conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing—original draft, and writing—review and editing by V.V.
Footnotes
Author Disclosure Statement
No competing financial interests or other conflicts of interest exist.
Funding Information
No funding was required for this study.