
Abstract
Introduction:
The National Public Health Reference Laboratory at the National Center for Disease Control (NCDC), Tripoli was the single site for SARS-CoV-2 diagnostic testing in Libya. During the pandemic, large quantities of waste were generated each day. In response, the laboratory biosafety team conducted an assessment and implemented a plan to strengthen biosafety and biosecurity measures to mitigate high-risk biological waste.
Objectives:
To assess the potential biosafety and biosecurity hazards during surges in diagnostic response and create training programs and accompanying effective standard operating procedures (SOPs) that align with medical practices, ethical standards, available resources, and local regulations.
Methods:
A biosafety team was created to assess existing practices, identify gaps, and provide recommendations. SOPs were developed for biological waste collection, segregation, offsite transportation, treatment, and disposal.
Results:
From May 2020 to May 2022 approximately 22.8 kilograms of COVID-19 testing related laboratory waste was created and managed on daily basis. In response, NCDC’s biosafety team achieved a number of key goals: All laboratory and contract employees were trained on waste management best practices; four waste management SOPs were developed and deployed to provide standard guidance; training sessions were conducted to enhance safety measures; biomedical waste were professionally managed, ensuring compliance with health and environmental standards; and the biosafety team conducted regular monitoring and inspections for accountability and adherence to protocols.
Conclusion:
Examining the complete lifespan of biological waste from creation to disposal can inform more comprehensive policy development and improve overall laboratory biosafety during pandemic response.
Introduction
Libya has faced continuous challenges in governance and stability since the 2011 revolution. Rival factions competing for power and governance have created and sustained humanitarian crises and degraded national and subnational health systems. Just as the 2020 ceasefire ended the six-year civil war, the COVID-19 pandemic hit, making the country and its weakened health system exceptionally vulnerable. Libya’s first case of COVID-19 was officially reported in Tripoli on March 20, 2020, in a 73-year-old man who had returned to the country on 5 March from a trip to Saudi Arabia. 1 By early 2022, Libya had recorded approximately 398,000 cases and 5,900 deaths from COVID-19. 2
Public health laboratories play a critical role in disease surveillance, diagnosis, prevention, effective treatment, health promotion and outbreak response. Timely and efficient diagnostic testing was key to confirming suspected COVID-19 cases, allowing for patients and their close contacts to take precautions to prevent further exposure and transmission. In Libya, the National Public Health Laboratory at the National Center for Disease Control (NCDC), Tripoli, served as the site for all SARS-CoV-2 testing in the country. Samples were received and testing was conducted in Biosafety Level 2 laboratories. The sample receipt, processing and COVID-19 testing cycle generated considerable amounts of medical waste on a daily basis, including discarded samples, reagents, consumables, and personal protective equipment (PPE) which drastically altered the healthcare waste, biomedical waste (BMW) compositions.3–6 While protocols for managing BMW differ across nations in Libya, the standard treatment methods involve autoclaving, shredding, and deep burial. In addition, BMW management is allocated to the private sector due to a lack of government resources and capacities. Currently, there are four private contractors engaged in waste treatment and disposal operating in the Northern region (Tripolitania) of Libya. However, these companies are operating on outdated legal frameworks and institutional inefficiencies with a complex interplay between public laboratories and private companies. The COVID-19 surge response created a tremendous increase in BMW at NCDC. Consequently, biosafety and biosecurity measures related to the handling and disposal of BMW had to be enhanced within the facility, prioritizing laboratory and public safety to mitigate adverse effects on health and the environment, and in accordance with interim guidance provided by the World Health Organization in 2020 (WHO). 7 However, the WHO guidance failed to address the requirements or suggested procedure for transferring decontaminated waste from the laboratory, a key challenge for NCDC. Inadequate management of healthcare waste has the potential to heighten the spread of COVID-19, especially in economically developing countries where regulations governing waste disposal are not as robust as in developed nations.8–11
Generally, developing countries are characterized by poor healthcare waste management and often employ improper waste disposal techniques. 12 While there may be potential safety risks associated with the disposal of waste from SARS-CoV-2 testing laboratory, there is a scarcity of studies that have examined these concerns. This study was designed to reassess the potential biosafety and biosecurity hazards and improve BMWs segregation, collection, storage, transportation, and final disposal to ensure the delivery of safe, efficient, and reliable waste management services as well as improve social acceptability and to create a sustainable clean environment in Tripoli.
Methods
Evaluation of Knowledge and Implementation of Practices
The majority of NCDC laboratory personnel were involved in a continual training in biorisk management program, which was organized in collaboration with Sandia National Laboratories, the World Health Organization, the Elizbeth R. Griffin Program (ERGP), the Civilian Research and Development Foundation (CRDF Global) and Global Health Development (GHD) and the Eastern Mediterranean Public Health Network (EMPHNET). NCDC prioritized general biosafety trainings including topics such as biorisk management, waste segregation and management (solid and liquid), and applied biosafety for all members working in diagnostic and research laboratories. Additionally, three technologists furthered their expertise by taking advanced courses earning their certification as biosafety officers. NCDC established a biosafety team, led by an IFBA-certified biosafety officer, and two additional technically trained PhD laboratory scientists who received basic and advanced-biosafety training through various international programs including those operated by Sandia and GHD/EMPHNET. In addition, all three team members participated in some form of biosafety officer mentoring or twinning program to gain hands-on skills including developing biosafety protocols, validating laboratory assessment tools, designing and facilitating training curriculum and evaluation. They also collaborated with colleagues at ERGP and GHD/EMPHNET for subject matter expert review, consultation, and greater international collaboration. This biosafety team was formed as an initial NCDC intervention team to assess existing knowledge, attitudes, and practices on waste management practices, to identify threats and weaknesses in operation and oversight, to provide recommendations for improvement, and to oversee the compliance of laboratory staff members. The biosafety team designed an evaluation process that includes two checklists to inspect laboratory biological waste management systems. The first checklist, Occupational Health and Safety, includes a set of questions to determine if each laboratory is implementing the recommended preparedness and planning activities for COVID-19. The second checklist, Biological and Hazardous Waste Management, provides a series of screening questions to ensure proper segregation, management, storage, transport and disposal from the NCDC public health laboratories. The complete checklists and guide are provided as supplemental material (see Supplementary Data S1). The NCDC laboratory and individual technicians were assessed on specific waste management handling best practices including: proper selection and use of PPE for various laboratory tasks, waste segregation and labeling (color coding), duration of waste storage, waste treatment methods, infection prevention control, post-exposure prophylaxis, and adherence to local regulations regarding final disposal. Furthermore, laboratory teams were evaluated on their knowledge of emergency response protocols for incidents involving biological waste, and notable progress on the development of contingency plans to address potential disruptions in waste collection or failures in waste treatment and disposal processes.
Training and SOP Development
The biosafety team reviewed outcomes from the checklist evaluations to develop a just-in-time refresher training for all NCDC laboratory personnel handling and processing samples to ensure biological wastes were handled safely and securely. While knowledge on selection and use of PPE was strong key BMW training topics that required refresher training included waste segregation, packaging and labeling, collection, storage, treatment, and transportation.
SOPs were developed in collaboration with the Infection Control Department at NCDC and in coordination with GHD/EMPHNET and ERGP to provide technical guidance, harmonize laboratory practices, enhance overall laboratory safety, and promote a culture of responsible waste management. 13 Three SOPs were developed using a universal SOP template (available as Supplementary Data S2) which are as follows: Collection and Segregation of Medical Waste; Medical Waste Offsite Transportation; and Medical Waste Treatment and Disposal. These SOPs outline the required PPE, materials, and steps for each activity and are freely available in English and Arabic. 13 Our intent in developing the SOPs was not only to respond to gaps in the assessment but also to develop a template SOP that could be systematically applied to the larger NCDC laboratory network in Tripoli, Benghazi, and Sebha.
Measuring Laboratory Waste Production
A private professional company was assigned by the director of the NCDC to offsite transportation, treatment and final disposal of BMWs for the period from May 2020 to May 2022. The company, already under contract with NCDC, employed an autoclaving system accompanied with a shredder (size 1000 kg/h and 500 kg/h plus 2 shredders) to decontaminate the BMW and reduce the size as required by the Ministry of Health (MoH). This company was assessed by the NCDC biosafety team to evaluate capacity and skills for BMW and was found to be the only company able to process waste safely and effectively. The company was certified by the MoH, Ministry of Trade and Ministry of Local Affairs (MoLA) and aligned with the Libyan Environment General Authorization (EGA) regulations and contributing to the sustainability of the environment criteria set by the as per Supreme Scientific Committee and the NCDC. 14 Laboratories, both public and private, that conducted COVID-19 diagnostic testing during the pandemic contracted with waste management companies for offsite sterilization and processing, as recommended by the national government. Any risk associated with handling the waste off-site (transportation, treatment, and final disposal) was the sole responsibility of the authorized professional contractor. The scheduled timeline for BMW collection and transportation was conducted by company’s members of staff was twice weekly, and the amount of generated waste was measured at the company’s site using weighing scale for each patch collected from the laboratory before treatment. Subsequently the records were submitted to the directory of the laboratory on regular basis. The EGA oversaw and regulated requirements for the construction of the landfill in accordance with territorial planning and considerations of its physical location and BMW contents. Waste is inspected by EGA and local governance officers on site before being approval for disposal.
Results
Increased BMW Generated During the Pandemic
There was a sharp increase in BMWs generated because of increased referred samples for COVID-19 diagnosis using polymerase chain reaction (PCR) method and utilized PPE, consumables, and sample containers during the pandemic. During the study period (May 2020–May 2022), a total of 17,130 kg of waste was referred for decontamination at an offsite facility using autoclave and shredder methods, Figure 1. This waste was generated from the investigation of a total of 650,445 samples sent from the laboratory. Notably, the largest amount of waste production peaked in August 2021, totaling 1,677.5 kg. On average, the reference laboratory generated 22.8 kg of solid infectious biological waste on a daily basis. Each batch of 96 samples processed with the Techstar nucleic acid extraction kit resulted in 2.8 kg of waste, whereas the Nuactor method produced 2.41 kg. These were the only kits used during this study period. Accordingly, the weight per sample ran between 0.025 and 0.029 kg (average 0.02745 kg) inclusive sample, plate, master mix together with PPE.
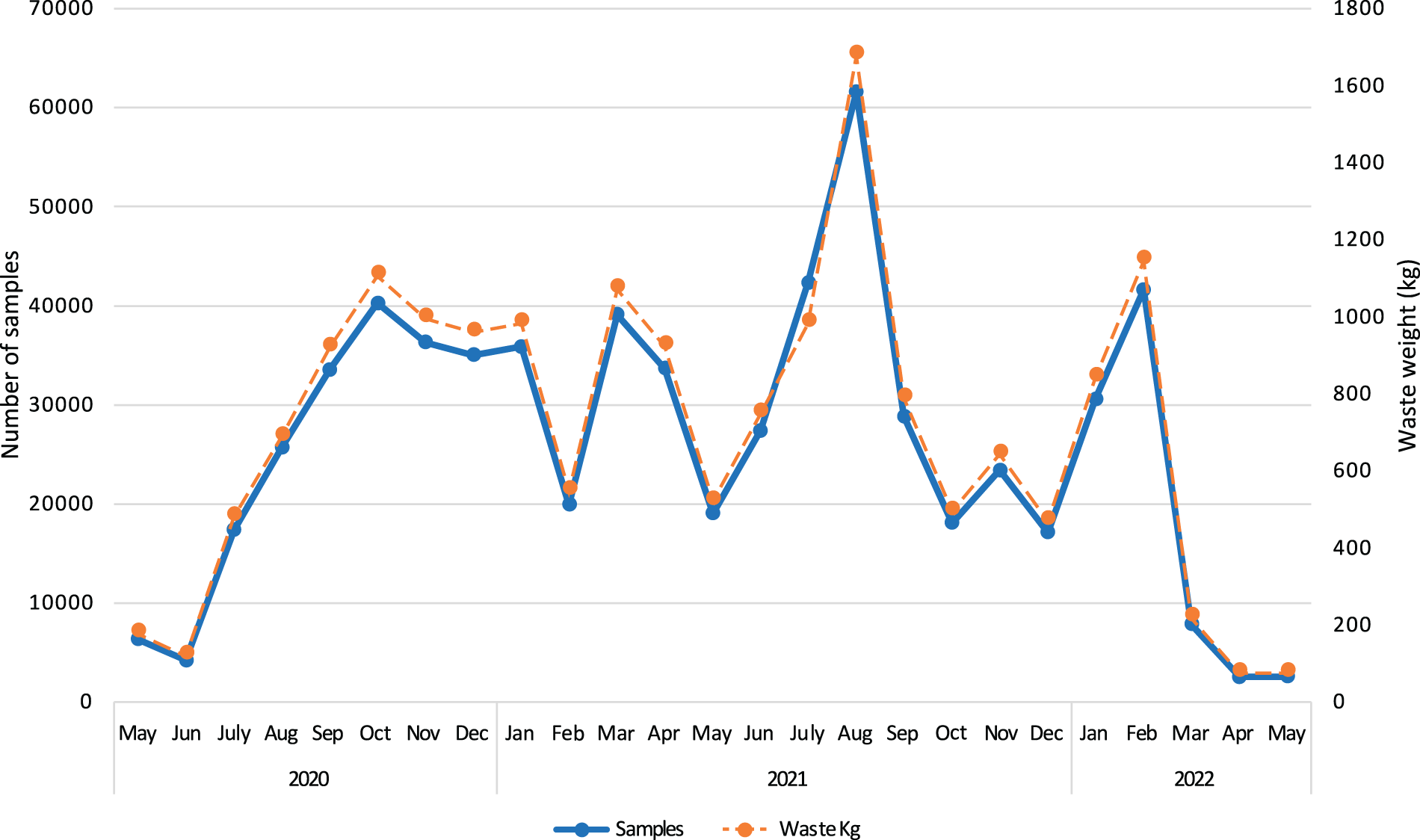
Distribution of processed samples and biomedical waste (BMW) generated/month during the pandemic. During the study period (May 2020–May 2022), a total of 17,130 kg of waste was referred for decontamination at an offsite facility using autoclave and shredder methods. This waste was generated from the investigation of a total of 650,445 samples sent from the laboratory. This graph demonstrates the correlation between COVID-19 processed samples (bold line) and generated BMWs in kilogram (dash line).
Capacities Assessment
All laboratory technologists assessed demonstrated a comprehensive understanding of an efficient waste collection scheme for daily operations including the segregation, collection, and storage of BMW in biohazardous autoclavable bags and subsequent storage in leakproof, puncture-proof containers at 4°C for 72 h prior to final transportation. However, due to lack of available space within the laboratory BMW was not autoclaved onsite. Instead, the waste was temporarily stored in solid leakproof container in a secure place before transportation to off-site treatment. Moreover, the Shams Alkhalij Company, the waste management company assigned to collection, transportation, treatment, and final disposal for the study period has an autoclaving system accompanied by a shredder to decontaminate the BMW and reduce the size as required by the MoH. This approach aligns with the Libyan Environment General Authorization regulations, is intended to reduce waste by 70% volume, followed by compression, and contributes to the sustainability of the environment criteria set by the Supreme Scientific committee and the NCDC. 14 As part of the program, contract personnel from the waste management company were trained on best practices for waste collection, handling, and transportation as well as decontamination and final disposal of BMW in compliance with regulations of MoH and the adherence to protocols of the MoLA. NCDC staff were monitored monthly for compliance with all available SOPs, while the waste management company was audited on a quarterly basis. Corrective actions were implemented immediately within the NCDC network with direct intervention and refresher training (where necessary) by the biosafety team whereas formal reports for noncompliance were submitted following the quarterly assessments of the waste management company.
Establishment and Implementation of Integrated Waste Management SOPs
Three integrated SOPs and accompanying training initiatives were developed and validated for BMW collection, segregation, offsite transportation, safety treatment, and final disposal, aimed at reducing the risk of infection and compliance with safety and accountability. SOPs and training for NCDC laboratory personnel covered the collection, segregation of medical waste, and temporary on-site storage, while SOPs for the Shams Alkhalij Company focused on the off-site transportation, waste treatment, and disposal. In addition, PPE was sufficiently supplied, accessible, and properly used during the handling of BMW. In contrast to PPE shortages experienced across several healthcare facilities, hospitals, and clinics, the NCDC public health laboratory did not run into supply shortages. Refresher training was provided to all laboratory staff to reiterate the limitations of PPE (for infection prevention) and to ensure the sequence of donning/doffing was performed correctly in combination with proper disinfection and good hand hygiene practices to minimize the probability laboratory acquired exposure/infection. The biosafety team conducted regular laboratory observations to monitor personnel SOP compliance, while the waste management company was audited on a quarterly basis to ensure adherence to terms, conditions, and scheduling as outlined in the SOP specifications of the offsite transportation. The adherence and compliance with SOPs were monitored by the NCDC director and by the designated officials (outlined in responsibilities and accountability section for each SOP). Laboratory personnel were audited through interviews, document review, and process observation to evaluate adherence. The contractor workforce was audited to identify errors, gaps, risks and opportunity for improvement. The waste management company was evaluated on the use of biological indicators, implementation of weekly and monthly safety checklists, availability of additional vehicles for surges, and logbook accounts of waste collected and processed. BMWs were transported in closed and sealed solid containers that display the biohazard label, using specially equipped cooled vehicles exclusively used for potentially infectious healthcare waste transportation set forth by local authorities, which are systemically cleaned and disinfected. Validation of autoclave process for the PROMED P400 was assessed using both chemical and biological indicators which reduces the likelihood of contamination, the autoclaved waste was then shredded, rendered unidentifiable and no longer considered hazardous. In addition, biosecurity risk assessments were conducted every six months to ensure safe transportation and company compliance with local regulations and guidelines. Consequently, there were no BMW-related incidents or injuries documented during the study period.
Occasionally, the waste management company did not meet the collection schedule, primarily due to armed conflict risks that hindered safe transportation of the treated BMW to the final disposal site. Other challenges included the high demand and substantial volume of medical waste generated from other healthcare facilities (isolation centers, laboratories, and private healthcare settings) that caused interruption of the waste collection. In such instances, NCDC notified the company of delays and alternate pickups were scheduled. In the interim sufficient space was allocated onsite until the alternate pickup. The government landfill site designated for the final waste disposal was inspected bimonthly by government authorities to assess the process and to ensure safety to the public and environment from potential contamination and hazards. In addition, to recognize the significant implications of improper waste disposal on community well-being and ecosystem integrity.
Discussion
In low-resource and conflict-prone settings like Libya, inadequate infrastructure for laboratory biological waste treatment and disposal poses a significant problem. During the pandemic, it has been reported globally that 97% of BMW produced from diagnostic tests for coronavirus were incinerated, this traditional method is harmful to the environment and contributes to the air pollution and greenhouse gas emission. 17 There is a pressing need for robust, practical and environmentally sound approaches to managing BMW generated during routine and surge operations. The COVID-19 experience can serve as an example of the type and quantity of waste than may be generated during surge response across laboratory networks. With proper data collection and analysis this information can serve as a standard in strategic planning for laboratory and medical facility waste management during outbreaks and pandemic preparedness.
Estimating the BMWs generation rate is essential for laboratories to design and implement a better waste management system for both routine and surge operations. During the peak of the pandemic, the average daily infectious waste at the NCDC laboratory was 22.8 kg, with estimated the weight per sample ran was between 25 and 29 g inclusive sample, plate, master mix together with PPE. Studies have demonstrated that the COVID-19 pandemic has profoundly impacted the quantity and composition of medical waste, resulting in a rise in the overall waste produced and an escalation of infectious waste in landfills.14,15 A literature survey from 2021 reported that for every 1000 coronavirus tests, PCR procedures produced about 22 kg of plastic waste, estimating a mass of over 15,000 tons of plastics generated from COVID-19 PCR testing worldwide.16,17
Training programs (initial and refresher) and facility-wide validated SOPs are essential components of an effective BMW management. As part of the post-training survey NCDC laboratory personnel regarded consistent and targeted training in BMW management as an essential component for ensuring safety, consistency in risk management, continuous improvement, and environmental protection, viewing it not merely as a regulatory requirement, particularly in the context of the COVID-19 pandemic. While the NCDC laboratory assessments, SOP development, and training were developed in response to the evolving issue of BMW generated during COVID-19, preventing environmental contamination of untreated waste, the process and subsequent capacity building established an institutional systemic approach to BMW management that strengthens laboratory biosafety, safeguards Libya’s ecosystem, and minimizes biological threats.
This study had some limitations due to the operating environment in Libya and the focus on solid waste. The concurrence of the COVID-19 pandemic and ongoing conflict and violent events in Libya undoubtedly exacerbated public health challenges in the capital city, where the final disposal of treated BMW was occasionally disrupted during insecurity and fighting. Our study did not address the management practices related to liquid BMW due to minimal liquid waste generated in the laboratory. It should also be noted that neither NCDC nor any other facility dealing with infectious pathogens in Libya has the capacity to treat liquid waste. However other studies, including El-Ramady et al, reviewed the challenges related to waste management including liquid decontamination during COVID-19 pandemic. 18 While available and operational, we did not employ the onsite autoclave and instead relied on the waste management contractor to sterilize and shred waste following removal from the laboratory. The main reason was due to lack of space within the facility, this decision introduced a level of occupational exposure risk of contract workers during collection and transportation. We partially corrected this risk by training the contract workers and transporting the package in a sealed containers to prevent subsequent exposure of direct waste bags/containers prior to terminal treatment. As noted above, we had no incidences reported during our study period.
Conclusion
Proper BMW treatment and disposal is a key component of laboratory biosafety and biosecurity as well as providing a safe environment to the larger community. We found that conducting regular biosafety assessments, providing refresher training and validated SOPs, and adequate and accessible PPE for medical waste management processes created an environment for the NCDC reference laboratory to manage the surge in samples and waste from SARS-CoV-2 diagnostic testing. We were successful in approaching processes both in the laboratory and across to the private sector to ensure adaptation and compliance with BMW management best practices. This integration very likely mitigated potential biosafety hazards and protected the internal and external environment. Our goal is to promote the BMW guidelines and SOPs developed under this project as a universal standard for diagnostic laboratories across NCDC laboratory network with hopeful adoption across sectors.
Authors’ Contributions
All the authors contributed equally to this work. Each author participated in the planning, execution, and analysis of the research, as well as in the writing, revision, and editing of the article.
Footnotes
Acknowledgments
The authors would like to thank their incredible colleagues at the National Center for Disease Control, Libya, for their courageous efforts during the pandemic. The authors appreciate the Elizabeth R Griffin Program (ERGP) and GHD/EMPHNET teams for their invaluable support and contribution.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Availability of the Data
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.
Ethical Statement
This study was conducted in accordance with the ethical standards set forth by National Center for Disease Control Committee. The study procedures were approved by director of the Public Health laboratory. The research was conducted in compliance with the Declaration of Helsinki and all relevant national and international guidelines and regulations.
Authors’ Disclosure Statement
No competing financial interests exist.