
Abstract
Informal care receipt is associated with better HIV treatment outcomes among patients vulnerable to treatment failure. Yet, informal caregiving can be highly stressful, leading to distress and cessation of caregiving. Research on factors contributing to informal caregivers' psychological distress may advance our understanding of how to improve caregivers' well-being and sustained HIV caregiving for a vulnerable population. We examined relationships among caregiver stigma, disclosure, and depressive symptoms in a cross-sectional sample of 207 informal caregivers of people living with HIV/AIDS (PLWHAs) in Baltimore, Maryland. Caregivers were primarily African American, low-income, urban adults participating in the Action, Resources, and Knowledge (ARK) study (2003–2005), which recruited urban PLWHAs and their main supporters. Results indicated that among caregivers, HIV caregiving-related stigma was associated with more depressive symptoms, while disclosure of caregiving status was associated with fewer symptoms. We also explored the buffering effect of disclosure in the relationship between stigma and depressive symptoms. Results indicated that among those who reported greater stigma, there was a significant decrease in depressive symptoms as the number of disclosures increased. In contrast, participants who indicated lower stigma had consistently fewer depressive symptoms regardless of number of disclosures. These results suggest the need for interventions to address high levels of depressive symptoms among informal HIV caregivers, particularly those who report greater caregiving stigma and less disclosure of their caregiver status. In addition, future research should examine these relationships further using longitudinal data from informal caregivers and their care recipients.
Introduction
R
Informal caregiving has been found to be highly stressful, and many caregivers report high levels of psychological distress, which can jeopardize their continuity of caregiving. 6 However, few studies have examined factors associated with psychological well-being among informal HIV caregivers who may face the potential stigma of PLWHA care recipients' HIV seropositive status. While understudied, research suggests that disclosure of caregiving or other personal challenges can have a protective effect on psychological well-being by allowing opportunities for affirmation and social support. 7 –9 The present study examined the role that caregiving-related stigma and caregiving disclosure play in contributing to or buffering informal HIV caregivers psychological well-being.
Informal caregivers are often defined as unpaid individuals who help friends or family members who cannot fully care for themselves. 10 Often, caregiving is associated with a multitude of stressors and psychological distress, referred to as caregiver burden. 11 In most studies, caregiving tasks per se are not found to be as stressful as the circumstance of caregiving, including problem behaviors among care recipients, such as engaging in disruptive or unpredictable behavior, and illicit drug use. 12 Perhaps most importantly, caregiving may interfere with the performance of other valued social roles. For example, in low-resource contexts, informal caregiving can be financially draining, especially in caring for illicit drug users, and can pose substantial economic strains resulting from lost wages from caregiving interfering with wage earning and from ill care recipients' disability or stigma restricting their job opportunities. 7,8,13 –15 Caregivers may also experience risks to social, physical, and mental health, with demands that often escalate over the course of the illness. 6,16
Stigma
Another potential source of stress for caregivers is stigma, which arises from an individual feeling ashamed or discredited by a visible or a hidden condition. 17 Courtesy (or associative) stigma, refers to feeling discredited through affiliation with a person who has a stigmatizing illness. 17,18 HIV is a potentially stigmatizing illness for both PLWHA 19 –21 and for their caregivers. 11,18,19 Among African American PLWHAs, stigma has been associated with depression, while in other studies, African American PLWHAs have indicated significantly lower levels of psychological distress compared to PLWHAs of other races and ethnicities. 22,23 In addition, caregivers may fear or experience rejection or loss of friends or family ties due to stigma, or may feel they have to hide from others their association with a PLWHA. 13,19,24,25 Living in relative secrecy because of perceptions of HIV-related stigma can elevate stress levels that can in turn increase the risk for depression, especially among family members of PLWHA. 11,26
Disclosure
It has been postulated that when individuals hide a stigmatizing condition, as is the case with some caregivers of PLWHA, they are faced with decisions/dilemmas regarding when and to whom to disclose their caregiver status, and concerns about potential social consequences of disclosure. 17 Disclosure among caregivers of PLWHA has been associated with both negative and positive social responses. For example, researchers have found that some people who disclosed their HIV caregiver status experienced rejection and harassment, while others gained social support. 9 Studies of African American women in the United States have shown that disclosure of one's HIV caregiver status has beneficial effects on caregivers' mental health. For example, talking about caregiving stresses with family members or friends has been associated with reduced anxiety. 21 Studies have reported great anxiety prior to public disclosure of one's own HIV status, but that the realized benefits of disclosure, including increased emotional support, outweighed the risks. 7,8 Researchers have also noted the societal benefits of HIV caregiving disclosure, in terms of reducing AIDS-related stigma and promoting tolerance of PLWHA. 7,8
Stigma, disclosure, and depression
Several prior studies have examined relationships between stigma, disclosure, and depression among PLWHA and their caregivers. 27 –29 Clark and colleagues 30 found that among PWLHAs with greater levels of perceived stigma, those with greater levels of disclosure also reported poorer psychological functioning. Extant literature suggests that among PLWHA, racial and ethnic differences exist in terms of psychological distress, which may in turn be associated with varying levels of stigma. 31 However, few studies have focused on caregivers of PLWHAs, especially on factors that are associated with depressive symptoms among their informal caregivers. 32 Studies of family caregivers of PLWHA found significant positive associations between stigma and depressive symptoms among caregivers, 11,26 while another study found that greater levels of disclosure was associated with fewer depressive symptoms. 7
In the current study, we hypothesized that among informal caregivers of PLWHA, perceived stigma would be associated with more depressive symptoms, while greater disclosure would be associated with fewer symptoms. We also explored the buffering effect of disclosure in the relationship between stigma and depressive symptoms. Results from these hypotheses could aid in identifying those caregivers at highest risk for depression, as well as inform interventions to reduce depressive symptoms among caregivers of PLWHA. In this analysis, other covariates such as age, gender, education, income, having HIV/AIDS, impaired physical functioning, drug use, caregiver burden, and role relationship between caregivers and PLWHA were added to the model since they have also been associated with depressive symptoms in previous studies with PLWHA and their caregivers. 11,32 –38
Methods
Participants
The Action, Resources, and Knowledge (ARK) study (2002–2005) recruited dyads of HIV-positive individuals (index participants) and their informal primary caregivers (supporters) from a community sample of Baltimore adults for a study examining social support, stigma, disclosure, HIV medication adherence, depressive symptoms, and other indicators of physical health. 1 ARK study eligibility included HIV seropositive status, over age 18, and Baltimore residency. Participants were recruited by street outreach; advertisement at health and social service agencies (e.g., homeless shelters, drug treatment clinics, needle exchange); and by referral of control condition participants of the Intervention for Seropositive Injectors—Research and Evaluation (INSPIRE) study, upon study completion. Twenty percent of the ARK sample had participated in the INSPIRE study. The current analyses focused on 207 informal caregivers, who were nominated by PLWHA as their primary supporter, were predominantly African American, and were sex partners, family members, or friends of the PLWHA.
Procedures
Surveys were administered face-to-face by trained interviewers using a computer-assisted personal interviewing (CAPI) approach and took approximately 1 hour and 15 minutes. All index and caregiver participants were interviewed separately in private research staff offices, signed informed consent forms, and were financially compensated $20 for their time. Approval was obtained from the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
Measures
Depressive symptoms
The outcome measure, caregivers' self-reported depressive symptoms, was assessed using the 20-item Community Epidemiology Study—Depression (CES-D). 39 The CES-D, which has been used in similar populations of caregivers of PLWHA, is a continuous measure of depressive symptoms. 26 Response options range from 0 = “rarely or none of the time (<1 day per week)” to 3 = “most or all of the time (5–7 days per week).” The range of scores for the current sample of caregivers was 0–55 with a positively skewed distribution and a Cronbach α of 0.91. To remedy the positive skew, we tested several different transformations using Stata 940 and concluded that the optimal choice was to transform the CES-D score using a natural logarithm +1 calculation.
Stigma
The stigma scale, which was adapted from items used by Wight and colleagues, 25 included six items with yes/no responses with items referring to perceived stigma from family and friends. For example, items included, “Some friends would avoid me if someone in my family had AIDS,” “Even though I know better, sometimes I still would feel embarrassed if my friend or relative had HIV,” and “Even though they might not say it, my family would not approve of my helping someone with HIV.” The six items were subsequently summed to form a single measure in the model. The scale had a Cronbach α of 0.84.
Disclosure
The disclosure scale, which was adapted from items used by Pearlin and colleagues, 6 comprised four items that included for example, “How many of your friends know that you are helping out [the care recipient]?” The remaining three items used a similar question format, but inquired about disclosure to family members, coworkers, and neighbors. Answer choices from these items included “none,” “some,” “most,” and “all.” Responses were summed to calculate a single score reflecting level of disclosure of caregiver status, with scale scores ranging from 0 to 12. The Cronbach α for this scale was 0.79.
Physical functioning
We used a 6-item self-report measure of caregivers' physical functioning adapted from the instrumental activities of daily living scale. 41 Examples of scale items included, “How much does your health affect your ability to eat, dress, bath, use the toilet,” “ … to bend, lift or squat,” and “ … to walk uphill or climb a few flights of stairs.” Each item was measured on a three-point scale with 0 = “not at all,” 1 = “a bit,” and 2 = “a lot.” The scale items were summed, with scale scores ranging from 0 to 12, with higher scores indicating greater impairment. The Cronbach α for the scale was 0.81.
Caregiver burden
Twelve items were used to assess burden, such as, the “extent that helping out others has caused you financial problems in the past year” and “ … caused you to lose work or to miss work in the past year.” 6,10 Answer choices included, “not at all,” “a little,” “some,” and “a great deal.” Scores ranged from 12 to 40 and the Cronbach α was 0.86.
Demographic characteristics
Caregivers responded to questions on age, gender, education, monthly income, HIV/AIDS status, drug use, and client-caregiver relationship status. Age was dichotomized using a median split at age 45 and education was dichotomized into less than high school vs. high school diploma or some college. Caregivers were asked if they had injected speedball, cocaine, or heroin; sniffed cocaine or heroin; smoked crack; or ingested street methadone or hallucinogens in the past 6 months. Respondents who answered “yes” to any of these drug use questions were coded 1 = yes, while those who answered “no” to all of the items were coded 0 = no. Relationship status was coded as 0 for non-kin (e.g., friend or main partner) versus 1 for kin (e.g., parent, uncle or aunt, sibling).
Data analysis
As part of our preliminary analyses, we generated univariate statistics to describe the sample characteristics. Next, we used factor analyses with maximum likelihood estimation to determine the dimensionality of the scales describing depressive symptoms, stigma, disclosure, caregiver burden, and physical functioning. In addition, we calculated Cronbach α reliability estimates for each of the scales.
Subsequently, we generated bivariate correlations between all of the study variables in preparation for conducting the two-step hierarchical multiple linear regression model. In the first step, we examined the main effects of stigma and disclosure on depressive symptoms, while controlling for age, gender, education, income, HIV/AIDS status, impaired physical functioning, drug use, caregiver burden, and kinship status. In the second step, we added the interaction effect of stigma with disclosure on depressive symptoms. Since the interaction was significant, we created a graph that was centered on caregiver burden and used the lowest order terms on each of the covariates with two curves representing respondents with the lowest and highest scores on the stigma scale.
Results
After generating frequencies on the model covariates in SPSS 15.042 (Table 1), we conducted factor analyses in MPlus 5.143 using a weighted least squares maximum likelihood estimator to account for the binary and ordinal-level scale items. The factor analyses indicated that all five of the scales were unidimensional with acceptable model fit (Comparative Fit Indices [CFIs] ranged from 0.96 to 1.00). 44 The factor analyses for all five scales produced eigenvalues that explained 40.9% to 81.0% of the variance in scale items and the Cronbach α for the scales ranged from 0.79 to 0.91 (Table 2).
SD, standard deviation.
Next, we ran bivariate correlations between all study variables in SPSS 15.0 (SPSS Inc., Chicago, IL; Table 3). We found significant correlations in the expected directions between stigma, disclosure, and depressive symptoms such that greater stigma was associated with greater depressive symptoms and disclosure was associated with fewer symptoms. We also found a strong significant negative correlation between relationship status and being HIV seropositive, such that informal caregivers who were not family members of the PLWHA were more likely to be HIV seropositive or have AIDS (r = −0.50, p < 0.05).
Note: Estimates in bold are significant at p < 0.05.
Before fitting the regression models, we tested the regression assumptions. We investigated and found support for the assumptions of linearity, normality, and homogeneity of variance using the log-transformed dependent variable. The bivariate correlations indicated that the independent variables did not have multicollinearity problems in the multiple linear regression model. However, we found that one participant was an outlier with a standardized regression residual greater than 3.3. Subsequently, we excluded this participant from the final regression analyses.
In the hierarchical multiple regression model analyses, we examined the main effects in step 1 (Table 4). We found that greater reported stigma was associated with greater levels of depressive symptoms (β = 0.13, t = 2.15, p < 0.05) and greater disclosure was associated with having fewer depressive symptoms (β = −0.13, t = −2.26, p < 0.05). We also found that greater depressive symptoms were associated with being younger (β = −0.16, t = −2.54, p < 0.05) and female (β = 0.14, t = 2.10, p < 0.05), in addition to reporting lower educational attainment (β = −0.13, t = −2.12, p < 0.05), greater impairment in physical functioning (β = 0.35, t = 5.21, p < 0.001), drug use in the past 6 months (β = 0.18, t = 3.00, p < 0.01), and greater caregiver burden (β = 0.25, t = 4.06, p < 0.001).
45 or younger = 0, older than 45 = 1.
Male = 0, female = 1.
Less than high school = 0, high school or some college = 1.
Does not have HIV/AIDS = 0, Has HIV/AIDS = 1.
No use within past six months = 0, some use in past six months = 1.
Non-kin = 0, kin or family member = 1.
p < 0.05.
p < 0.001.
p < 0.01.
Step 2 of the model, which included the interaction term between disclosure and stigma, indicated that the interaction was significant (β = −0.20, t = −1.99, p < 0.05). Subsequently, we plotted the interaction of stigma (either 0, the lowest, or 7, the highest) and disclosure (0 to 12) on the level of depressive symptoms, using CES-D scores that were translated back into the original scale units, while centering on caregiver burden and selecting the lowest order of each of the other covariates (Fig. 1). We found that while disclosure had little effect on depressive symptoms among those with the lowest stigma scores, participants who reported the highest stigma scores had significant reductions in depressive symptoms associated with greater disclosure of their caregiving status.
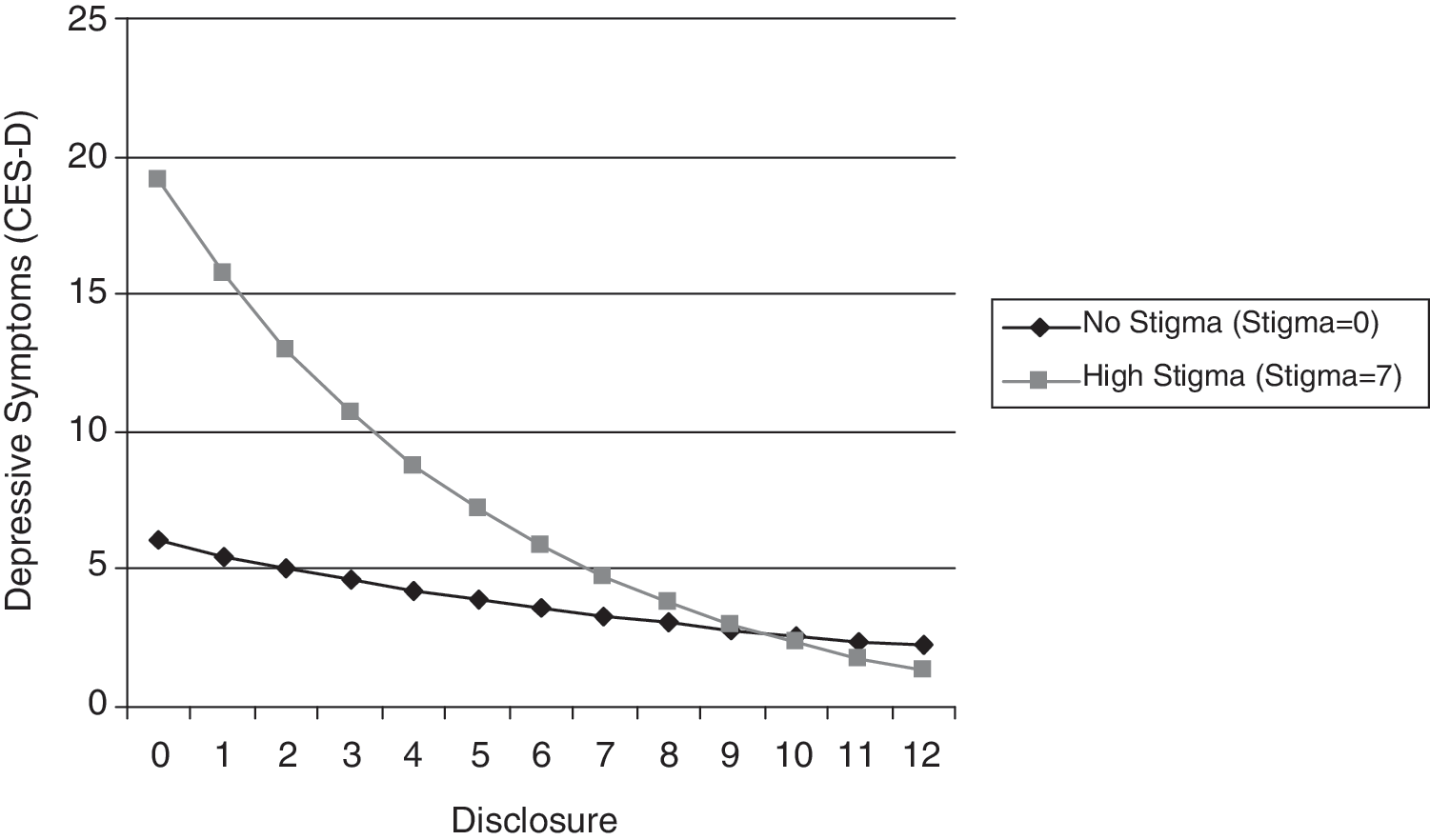
The interaction between stigma and disclosure on depressive symptoms.
Discussion
As hypothesized, we found that stigma was associated with higher levels of depressive symptoms among informal HIV caregivers and that greater disclosure of caregiving status was associated with fewer depressive symptoms. Both of these study results support extant literature on the main effects of stigma and disclosure on depressive symptoms. 7,11,26
The study results also indicated that disclosure moderated the relationship between stigma and depressive symptoms such that those individuals with greater stigma who had also disclosed their caregiver status to others experienced fewer depressive symptoms. These results suggest that future interventions should facilitate caregiving disclosure where appropriate, particularly for caregivers who report greater stigma but have not disclosed their caregiver status to others. In addition, anecdotal evidence from the study indicated that some participants expressed interest in disclosing their caregiver status and requested guidance in how or when to disclose.
Formation of support groups for family and friends of PLWHAs may be one way to facilitate disclosure. For example, one study of caregivers of PLWHA reported decreased feelings of social isolation as a result of a support group intervention. 45 Support groups may enable caregivers to discuss their stresses openly with people who may empathize with them. However, individuals in this high-risk, high-needs population may need more structured interventions than basic support groups to help them decide when to disclose, the possible risks and benefits of disclosure, and optimal ways of disclosing. 7,9 Also, learning how to minimize the stresses of negotiating HIV caregiving responsibilities, especially from nondepressed caregivers, could be a valuable component of interventions designed to reduce depressive symptoms among HIV caregivers.
Research suggests that informal caregiving is highly normative among low-income African American communities, and that caregiving support programs often do not adequately reach them. Low-income African Americans provide disproportionately higher levels and more intensive forms of informal HIV care compared to other income or racial groups. 16 Moreover, they tend to underreport caregiving burden, and to be underrepresented in caregiving organizations and in caregiving support groups that are currently often hospital-based. Future research is needed to explore ways to mobilize caregiving groups in this disadvantaged caregiving population at high risk for caregiving-related depression. Community-based recruitment and venues for HIV caregiving support groups may help to improve their engagement in caregiving support programs, which may have implications for their own well-being as well as for continuity of care receipt and HIV treatment outcomes.
In addition, further research is needed to determine the degree to which care recipients' illicit drug abuse contributes to caregivers' perceived affiliative stigma. Future studies that examine detailed data on PLWHA care recipients' drug use history may help to ascertain this relationship. Such information may help to inform appropriate approaches to intervention to reduce caregivers' affiliative stigma in this community.
Several limitations should be noted with regards to the current study. Because we used cross-sectional data, longitudinal study may further our results by enabling researchers to explain the interaction of stigma and disclosure on depressive symptoms over time. In particular, future research should address the direction of causality between the study variables since it is possible that more depressed people are less likely to interact with others, which may subsequently lead to fewer disclosures of caregiver status. It is also possible that alternative specifications of the disclosure variable could alter the strength of its relationship with depression. In addition, more depressed people may perceive greater stigma due to the association between depression and negative thoughts. Therefore, longitudinal studies that can address the causal direction of these variables are warranted.
Also, these data may be potentially limited by recall bias. Participants may not accurately remember the number of individuals to whom they disclosed their caregiver status, especially if they had been caring for an HIV-seropositive individual for a number of years. In addition, sample members may not accurately represent all of the caregivers of HIV-positive individuals. Healthier caregivers who perhaps felt less stigmatized and freer to discuss their caregiver status may have been more likely to consent to the interview. However, including data from these caregivers would likely strengthen the interaction effect. Finally, the generalizability of the findings may be limited to urban African Americans who live in areas with high HIV/AIDS and drug use prevalence.
Despite these limitations, the current study adds to the body of relatively few studies that address depressive symptoms among caregivers of people living with HIV or AIDS. 32 While relationships between stigma, disclosure, and well-being have been explored among people with chronic illnesses, little research has examined these relationships among caregivers of people living with HIV or AIDS. 6 Psychosocial research among caregivers of PLWHAs is vital to improving the well-being of these caregivers as well as their care recipients, who have major disparities in HIV health outcomes. Therefore, research that aids in the support of informal caregivers is vital to maintaining or improving psychological functioning among caregivers as well as the people who depend on them, including PLWHAs and their family and friends.
Footnotes
Author Disclosure Statement
No competing financial interests exist.