
Abstract
A peer-driven intervention (PDI) was developed to support uptake and adherence to highly active antiretroviral therapy (HAART) among women sex workers who use illicit substances in Vancouver, because uptake and adherence continues to be suboptimal. Trends of adherence were examined among women in this program by (1) exposure to the intervention and (2) risk behaviors including drug use and unstable housing. Between January 2007 and January 2008, 20 HIV-positive women were enrolled into the PDI on a rolling basis. PDI participation included weekly peer support meetings, a health advocate (buddy) system, peer outreach service, and onsite nursing care. Adherence was measured directly with pharmacy records (PR) and indirectly with self-report and viral load (VL) outcomes. Participants attended an average of 50 (21–70) PDI meetings. Overall self-reported adherence was high (92%) and most women (11) reported increased adherence from the first to the last 13 PDI meetings attended (average increase = 18%). The number of viral load tests ≤50 copies/mL increased by 40% from the pre-PDI period (1 year before enrollment), to the PDI period (duration enrolled). PR adherence and improvements in VL outcomes were higher among participants with greater housing instability and frequency of injecting/smoking drugs. Despite a very difficult environment to provide HIV care, there is evidence to suggest that the PDI may have had a positive impact on adherence outcomes. Although this would not predict long-term treatment success, the PDI approach to HIV treatment support is a promising program for women who might otherwise be excluded from treatment altogether.
Introduction
T
Although there is no gold standard for the definition of optimal adherence, 2 evidence suggests that a moderate level of adherence to newer HAART therapies is important for consistent viral load suppression, although disease progression is reduced and mortality is improved with increased adherence. 3 –5
Unfortunately, even in many developed country settings where HAART is readily available, adherence to antiretroviral medication among vulnerable populations such as injection drug users (IDUs) continues to be suboptimal. IDUs face greater challenges adhering to HAART than other populations, 6 –8 and have been shown to have a poorer uptake of and virologic response to HAART as well as greater mortality from AIDS. 6,9
A wide range of interventions have been suggested to improve adherence to HAART among vulnerable populations, ranging from social support, directly observed therapy, counseling, financial incentives, and technological devices. 2,10
Social support exists in an informal structure in many populations, and can include the provision of services (clinical or other) or monetary compensation (including food or travel), or outreach (by outreach workers, peers, friends, or family). 2 Social or peer support adherence interventions programs are intended to harness positive aspects of social relationships that can increase adherence 2,11 ; these programs have been shown to help patients manage chronic infectious diseases such as HIV in IDUs. 2,11 –16 Broadhead et al. 11 developed a peer-driven intervention (PDI) program for IDUs with HIV in which each of the 14 participants was assigned a health advocate, a peer of the same gender. Peers and health advocates met weekly with one another for counseling and support. The PDI influenced participants to keep up their medical care, and improved their medication adherence.
In British Columbia, Canada, the provincial drug treatment program provides antiretrovirals free of charge to all people living with HIV. 17 However, despite wide availability of HAART, evidence suggests that IDUs in Vancouver's Downtown Eastside (DTES) continue to experience lower levels of access and adherence to HAART, including lower response rates of CD4 cell counts. 7 Among the population of interest in this study, HIV-positive women in the DTES who engage in survival sex work and use illicit substances, less than half reported currently being on HAART, and 26% who were previously on HAART had discontinued. 18 Barriers to accessing HAART included a fear of side effects, lack of knowledge about the treatment, inability to adhere to daily medication regimes and make regular medical appointments, and a fear that others would suspect their HIV status. 18 Other factors that may indirectly impact adherence, such as poor access to health and support resources, poverty, lifetime history of trauma, and high levels of drug use are also characteristic of this population. 18,19
In response to the suboptimal uptake and adherence to antiretroviral therapy in this community a peer support model, known as a PDI was developed and piloted. The objectives of this study are to examine trends describing the association between adherence and: (1) exposure to the intervention and (2) risk factors for lower retention (e.g., drug use patterns). Results from this analysis are intended to help with the continued development of treatment and care options that meet the needs of this population, and have important implications for designing and scaling up effective interventions in similar populations.
Methods
Study design
A pilot PDI was implemented within a larger community-based HIV research project partnership (the Maka Project), between the British Columbia Centre for Excellence in HIV/AIDS and the WISH Drop-In Centre Society. 18,19 Participants were recruited into the PDI through referral by an HIV specialist, family care physician, or other health provider, friend, or by self-referral. Recruitment happened on a rolling basis beginning in January through August 2007. Prior to the first PDI visit, women completed a health intake questionnaire. Eligibility criteria included being an HIV-positive woman (or transgender woman) either currently or formerly involved in sex work and medically eligible for HAART (CD4 < 250), and needing additional support to either initiate or adhere to HAART. Analyses were based on participants with a minimum of 6 months enrollment in PDI.
Pilot PDI model
Based on initial research on the barriers to accessing and adhering to antiretroviral therapy in this population, 7,18,20 the PDI intervention consisted of four key elements: weekly peer support meetings, capacity training for women to become health advocates (“buddies”) to one another, a peer outreach service, and drop-in onsite nursing service. After initial intake, women received extensive training and support on becoming a health advocate to another woman. Standardized training was lead by a local sex work organization. Project staff then allocated the pairing of a health advocate-peer dyad. All women attended a weekly 1-hour peer support group session with their dyad (4–5 dyads per group), led by a community facilitator, in which they received education and facilitated discussion on health and wellness topics (including safe disclosure, managing side effects, depression, nutrition, positive living). Women were divided into three support groups. A nurse was available onsite at all times to provide referral for health and support services (e.g., counseling, crisis support), follow-up with regular care providers and discuss challenges with adherence, and health and HIV care issues. At the end of the weekly support group, women completed a questionnaire with their health advocate/peer dyad.
Women also set goals for the week in terms of peer support needs, such as attending medical or social support appointments. Each pair then discussed their goals with the community facilitator and received honoraria for attendance at the PDI groups and support to their dyad ($10 for attendance in the 1-hour group; $10 for support of the health advocate-peer dyad; $5 support for a peer's adherence of 95% or more based on pharmacy records, paid to the health advocate). Due to regular inconsistencies in pharmacy records (i.e., missing records and significant delays in accessing records), the financial incentive could not be attached to pharmacy records as initially planned and compensation for adherence was tied to self-reported adherence. Because of challenges identified by project staff and participants, the direct financial incentive for adherence was removed in June 2007.
Data collection tools
Three types of questionnaires were administered: a baseline intake questionnaire by the project nurse (included information on sociodemographic and psychosocial characteristics, baseline and past health problems, medication management and regime, other medications used, drug use and resource needs assessments); a weekly questionnaire administered by health advocates (included information on health/HIV care, self-reported adherence to HAART, housing, drug use, violence, police presence and impact); and a 3-monthly health questionnaire (results not included).
Measuring adherence
Adherence was measured using pharmacy records, self-report, and viral load outcomes. Daily records of adherence were collected from participants' pharmacies; if participants were directly observed to take HAART, or if they picked up their medication or had it dropped off, then that day was counted as adherent. The fraction of days adhered to per week was calculated to give an overall score of adherence per PDI-week; supplementary outcomes included the fraction of weeks with 100% (comparable to self-reported adherence) and 80% adherence. Self-reported adherence was assessed by a question, “Did you take all of your antiretrovirals last week?” on the weekly health advocate questionnaires (i.e., fraction of weeks with 100% adherence). Viral load test data was collected through the Provincial Drug Treatment Program. 17 For each participant, the fraction of all viral load tests less than or equal to 50 copies/mL (undetectable) were calculated.
Because of sample size considerations, we did not have the power to conduct standard regression-based statistical analysis. Instead, we calculated adherence trends by PDI exposure and adherence risk factors (see below). Results were presented in graphs, with mean adherence as a summary measure.
Measuring exposure to the PDI
To assess the impact of exposure to the intervention, self-reported adherence for the first 13 versus the last 13 PDI meetings attended was calculated, as well as the change in self-reported adherence using the formula [(fraction of weeks with 100% adherence in the last 13 PDI meetings attended − fraction of weeks with 100% adherence in the first 13 PDI meetings attended)/(fraction of weeks with 100% adherence in the first 13 PDI meetings attended)]. We could not do this for pharmacy adherence data due to the amount of missing information. The fraction of viral load tests less than or equal to the critical value (50 copies/mL, or undetectable) were calculated for two periods: pre-PDI (1 year before PDI enrollment) and PDI (the duration of PDI enrollment until May 2008). The change in the fraction of viral load tests with undetectable viral load from the pre-PDI to the PDI period was also calculated using the formula [(fraction of viral load tests ≤50 copies/mL in PDI period − fraction of viral load tests ≤50 copies/mL in the pre-PDI period)/(fraction of viral load tests ≤50 copies/mL in the pre-PDI period)]. The change in self-reported adherence from the first 13 to the last 13 PDI meetings attended and the change in the fraction of undetectable viral load tests (pre-PDI to PDI period) were examined by the number of PDI meetings attended (in quartiles: ≤40, 41–50, 51–60, and >60 meetings).
Variables of interest
Trends of adherence by several behavior variables previously shown to impact adherence were examined. Housing stability was measured with a binary variable (moved at least once during PDI enrollment: yes/no). Drug use during the PDI was categorized by injection drug use and smoked drug use (injected/smoked on average at least one day per week: yes/no). Because crack cocaine smoking was the most common type of drug use, adherence was examined by frequency of crack smoking (“approximately daily,” defined as 5–7 days per week for at least 50% of all weeks enrolled in the PDI: yes/no). Finally, the relationship between self-reported adherence and pharmacy record adherence was examined, using a common measure (i.e., fraction of weeks with 100% adherence).
Results
Baseline characteristics of the population
Twenty participants were included in this analysis. Participants had a mean age of 41.7 years (range, 21 to 62 years). The mean number of weekly PDI group meetings attended was 49.5 (21 to 70 meetings). Self-reported health problems at baseline were common, including hepatitis C (75% reporting), depression (50%), rash (35%), nausea or vomiting (30%), neuropathy (30%), asthma (30%), abdominal pain (25%), headache (25%), and diarrhea (15%).
The majority of women reported living in a single room occupancy hotel (55%), with 20% reporting living in an apartment or house, 10% reporting having no fixed address, and 15% reporting having another living situation. During PDI enrollment, 80% of participants reported moving at least once. Fifty-five percent of the women reported that their partner/family were their main sources of social support, with 20% reporting their friends, 10% reporting HIV organizations, and 10% reporting a social worker.
At baseline, 40% of participants reported they currently injected drugs, including stimulant drugs (cocaine, crack cocaine, crystal methamphetamine) and/or opiates (heroin, morphine or dilaudid). Eighty-five percent of participants reported that they currently smoked drugs (including cocaine, heroin, or crystal meth); 80% reported that they currently smoked crack cocaine. Twenty-five percent reported they currently injected heroin although none reported injecting daily.
Pharmacy record adherence
The overall mean adherence from pharmacy records was 87.9% per PDI-week (range, 26.2% to 100%). The mean fraction of weeks with 100% and at least 80% adherence was 75.8% (range, 5.3% to 100%) and 83.2% (range, 10.5% to 100%), respectively.
Figure 1 shows how the three measures of pharmacy record adherence varied by different risk behavior characteristics. The mean weekly adherence per PDI-week and the mean fraction of weeks with 80% and 100% adherence was higher in women who injected or smoked drugs an average of at least 1 day per week, who reported smoking crack approximately daily and who reported moving at least once during the time they were enrolled in the PDI (Fig. 1).

Three measures of pharmacy record adherence (mean adherence per peer-drive intervention (PDI)-week, mean fraction of weeks with 80% adherence and mean fraction of weeks with 100% adherence) by risk behavior characteristics.
Self-reported adherence
The overall fraction of weeks in which participants reported taking all of their HAART during PDI enrollment was 91.7% (range, 68.4% to 100%), which was higher than pharmacy adherence.
During the first 13 meetings attended, 87.2% participants reported taking all of their HAART in the past week, with 90.4% of participants reporting this in the last 13 meetings (an average increase of 3.7%). Eleven participants reported an increase in self-reported adherence (an average increase of 17.8%), whereas five reported a decrease in adherence (an average decrease of 19.1%) and four reported stable adherence (all 100%).
Viral load outcomes
There were 43 tests that reported less than or equal to 50 copies/mL in the pre-PDI period and 57 tests less than or equal to 50 copies/mL in the PDI period, for an average of 2.2 tests per participant and 2.9 tests per participant in the pre-PDI and PDI periods, respectively. In total, 43.9% of the tests in the pre-PDI period had viral load less than or equal to 50 copies/mL whereas 61.3% of tests in the PDI period had viral load less than or equal to below 50 copies/mL, representing an increase in the overall fraction of tests less than or equal to 50 copies/mL from the pre- to PDI periods of 39.6%.
Figure 2 shows the mean percent change in the fraction of viral load tests less than or equal to 50 copies/mL from the pre-PDI to the PDI period by the number of PDI meetings attended. The amount by which viral load outcomes improved over the two time periods increased along with the number of PDI meetings attended, from 7% to 59% among women who attended less than or equal to 40 PDI meetings and greater than 60 PDI meetings respectively. Women who attended 51–60 meetings had the highest increase (96%) in suppressed viral load tests over the two time periods (Fig. 2).
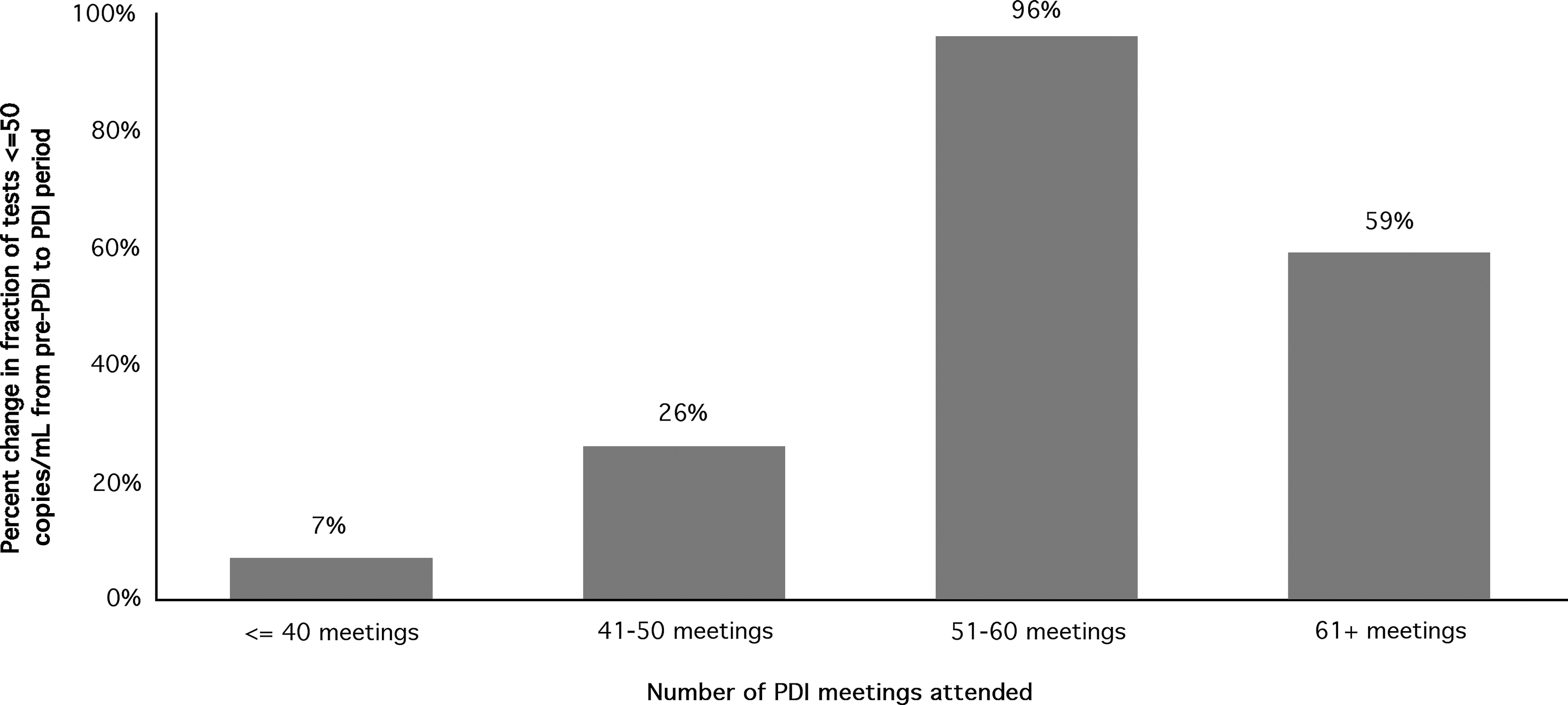
Percent change in viral load tests ≤50 copies/mL by number of peer-driven intervention (PDI) meetings attended.
Figure 3 shows how the average percent change in the fraction of viral load tests less than or equal to 50 copies/mL from the pre-PDI to the PDI period varied by different risk behavior characteristics. The average increase in the fraction of tests meeting the 50 copies/mL criteria over the two time periods was 29.2%. Viral load outcomes showed greater improvement over the two periods for participants who injected drugs more frequently, smoked drugs more frequently and who moved at least once during their enrollment in the PDI (Fig. 3).
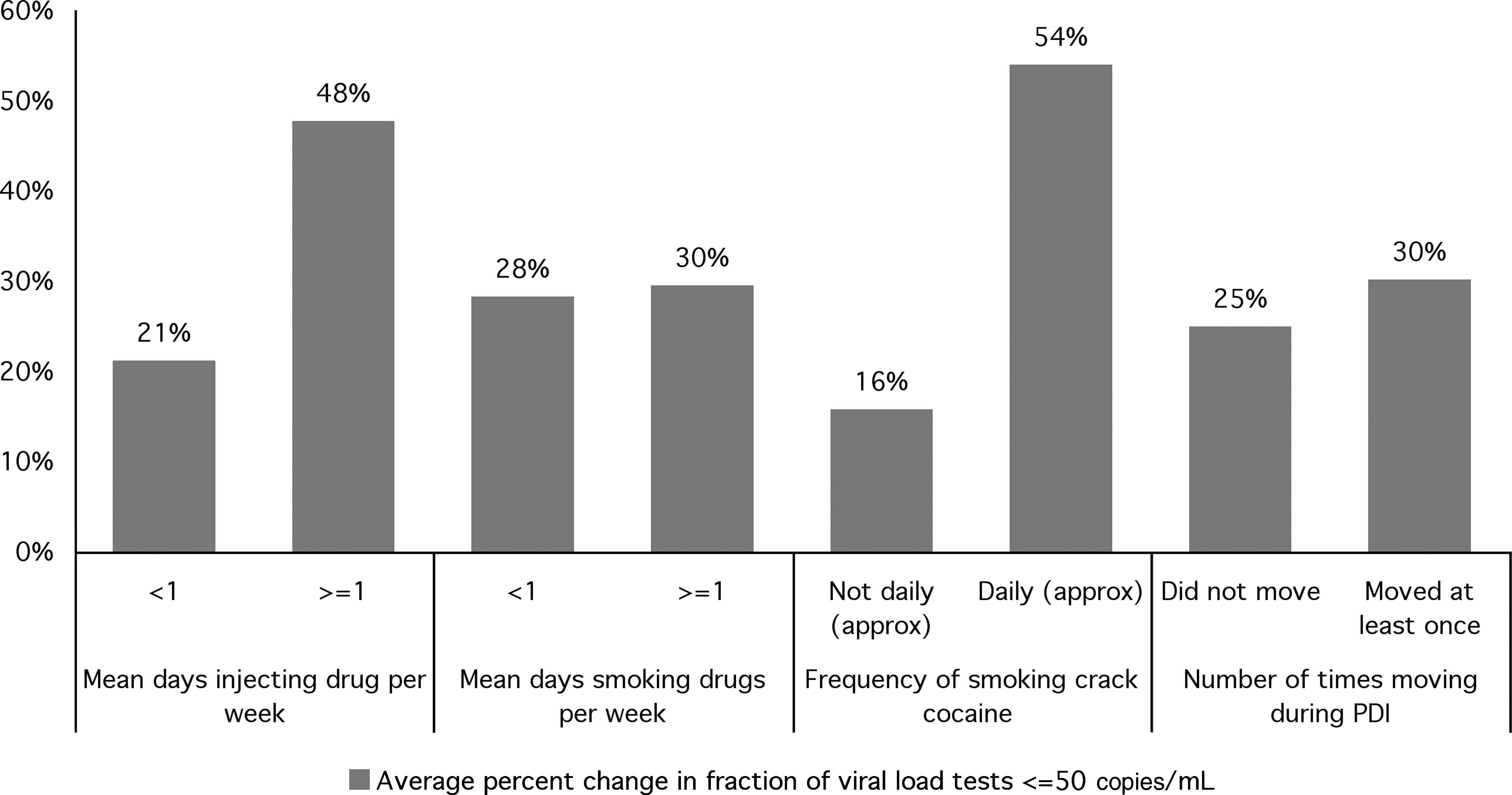
The average percent change in the fraction of viral load tests less than or equal to 50 copies/mL from the pre-peer–drive intervention (PDI) to the PDI period by different risk behavior characteristics.
Discussion
In this study we examined trends describing the association between adherence to antiretroviral medication in a group of women sex workers in Vancouver's downtown eastside area and: (1) exposure to a peer-driven intervention designed to increase uptake and adherence and (2) risk behavior factors previously shown to be associated with reduced adherence, including injection or smoked drug use and housing instability. Results suggest that the PDI may have had a positive impact on adherence outcomes, since self-reported adherence either increased or remained the same over the course of enrollment for 75% of the women, the percent change in the number of times viral load was undetectable increased along with increased attendance to PDI meetings and there was a higher fraction of undetectable viral load tests while women were enrolled in the PDI compared to the year prior to enrollment in the PDI. The PDI may have been more beneficial for higher-risk women, since pharmacy record adherence and improvements in viral load outcomes were higher among participants with higher risk behavior including increased drug use and housing instability.
Self-reported adherence in our study was measured with a high, 100% cutoff point; nevertheless, overall self-reported adherence was higher in our study (92%) than what has been reported in other studies (varied from 30% 21 to 86% 22 in a review 2 ; other studies report 89% and 83% 23 adherence). Self-reported adherence may have been relatively high in this study because early in the intervention, women were partnered with a peer, and a financial incentive was attached to the peer's adherence. Given challenges identified early on by project staff and participants with respect to attaching financial incentives to self-reported adherence both in terms of social desirability bias and trust with researchers and care providers, direct financial support for adherence was removed in June 2007. While this may have helped boost overall adherence, it does not explain why the majority of women either had stable adherence or an increase in self-reported adherence from the first 13 to the last 13 PDI meetings attended. It is also possible that since the PDI required a fair amount of commitment by participants, the program attracted a group of women who already had the ability to adhere well or improve adherence to antiretrovirals. Overall adherence from pharmacy records was lower than adherence from self-report and may reflect a more accurate measure of adherence. However, the amount of missing data from pharmacy records makes it challenging to draw strong conclusions from these data. Despite this, we also found that there was a positive relationship between self-report adherence and pharmacy record adherence, indicating that these two measures may be related.
There were some limitations and challenges to this study, as well as strengths. This study analyzed a small sample size and so the strength of the interpretations of quantitative results is limited; however, small sample size was a benefit to the PDI, because a major part of the PDI was the peer support group meetings. Women in the program felt that a smaller group size was ideal since smaller groups allowed for increased cohesiveness and closer bonds among members. If a group got too large, it would have to split up, inhibiting the continuity and closeness and trust that women developed. We did not have a comparison group for the PDI attendees, although a randomized controlled trial comparing adherence outcomes among women in the PDI model compared to the standard of care would be ideal to validate our study results. However, in the project development stages it was perceived to be unethical to randomly allocate women to a PDI compared to a non-PDI group because all the women were interested in the peer concept from the outset and it was not possible to randomize to standard of care and still keep the women engaged in any form of care.
In the future, self-report adherence would likely be the optimal way to measure adherence in this population rather than from pharmacies, unless the intervention program could directly oversee and allocate HAART prescriptions. Self-report is simple, inexpensive, commonly used and perceived to be a valid measure of medication adherence, though overreporting is sometimes a concern. 24 –26 In a recent meta-analysis review of adherence to antiretrovirals in the general population in North America and sub-Saharan Africa, 77% and 66% of the articles examined used self-report. 25 When not tied to financial incentives, self-reported HIV medication adherence was perceived to be fairly accurate in this study. Women could receive medication from any pharmacy in this study; however, each pharmacy had different quality of data record-keeping and levels of commitment to participating in the PDI which resulted in a fair amount of missing or unconfirmed data even though this method was meant to be the more objective assessment of adherence. Viral load outcomes (and CD4 counts) have been shown to be associated with improved adherence 27,28 and are useful indirect measures of adherence that can supplement self-report data. Although we cannot be sure that we were measuring adherence only, the number of undetectable tests increased among women in the course of the program and this may indicate that the PDI had other positive health-related impacts in addition to improving adherence.
Although a cost-effectiveness analysis is beyond the scope of this article, we were able to estimate the monthly cost of continuing and monitoring the PDI program with the core essential components (peer support meetings, health advocate capacity training) to be approximately $173 per PDI participant. This is less than some programs (e.g., intensive individual-based) 29 but more than others (e.g., pillbox organizers). 30 The incentive provided to PDI participants ($30 per week) is relatively high, and comprises three quarters of the total program cost; it is feasible that this could be reduced without compromising participation.
However, in line with a harm reduction framework and a peer-based approach, there are important benefits of a high incentive. This PDI model is intended to target high-risk individuals who have traditionally been neglected in current models: individuals with drug addictions, who have experience as survival street-based sex workers, who frequently have unstable housing, who identify as women and who are HIV-positive. Programs targeted at higher-risk individuals tend to be most costly. 31 The incentive promoted peer group attendance, cohesion, and a measure of stability, an important benefit to these PDI participants. For many women, the incentive and peer support group involvement also reduced their time engaged in survival sex work. 32 Women reported increased self-esteem and reduced boredom as a result of participation in peer support meetings, leading to less time spent on the streets and drug use. 32 Women developed close relationships with one another and benefited from increased social and moral support. 32
In conclusion, the majority of the women in the program reported either an increase in adherence or stable adherence throughout the program as well as improved viral load outcomes. This program brought attention to the HIV treatment and care needs of a group of women who might otherwise be excluded from treatment altogether. In the future, the project will continue in a modified form. It will be partnered with a local sex work support organization in Vancouver (WISH Drop-In Centre Society) and will be adapted according to recommendations given in an independent review. There will be other opportunities for continued monitoring and assessment of the program in order to best tailor it to the HIV treatment and care needs of this population.
Footnotes
Acknowledgments
K.N.D. drafted the manuscript, and analyzed, interpreted, and entered data; K.S. made substantial contributions to conception and design of the study, and acquisition and interpretation of data; H.S., D.P., and E.G. made substantial contributions to data acquisition and study design; M.W.T. made substantial contributions to conception and design of the study and interpretation of data.
This study was supported through a grant from the Canadian Institutes for Health Research (CIHR). K.D. is supported through Ph.D. trainee scholarships from CIHR and the Michael Smith Foundation for Health Research (MSFHR). M.W.T. is supported through a Senior Scholar Award from the MSFHR. Special thanks to Peter Vann.
Author Disclosure Statement
No competing financial interests exist.