
Abstract
There are no published reports on ways in which caregivers use the Internet to support people living with HIV/AIDS (PLWHA). Five hundred caregivers were recruited in a 5-week period to complete an online survey of demographic characteristics, Internet use, online health-seeking self-efficacy, and ways they used the Internet to support PLWHA. Caregivers were on average 39 years old, white, heterosexual, highly educated, and Internet-savvy. Most provided informal care only (e.g., as a friend; 78%), with the remainder divided among those who provided care exclusively as part of their job (11%) or in both informally and professionally (11%). Most (72%) respondents visited a general medical website for HIV information, and 44% shared information from the Internet with PLWHA. Compared to informal caregivers, caregivers whose roles were both informal and professional had greater odds of recently sharing information from the Internet with PLWHA (odds ratio [OR] = 2.03) and ever printing off information from a website to give to PLWHA (odds ratio [OR] = 3.87). Professional caregivers had higher odds of ever printing off information from a website to give to PLWHA (OR = 1.87), but lower odds of sending an e-mail with a website link (OR = 0.32) than informal caregivers. These findings suggest that websites providing HIV-related resources should consider the various ways in which caregivers use their content, and how utilization differs by role. More research is needed to understand how people providing care for PLWHA share information and support each other and the impact that doing so has on caregiver burden and treatment outcomes for PLWHA.
Introduction
L
The Internet has revolutionized how individuals access and share health information and resources. Studies show that health care providers are increasingly using electronic means to distribute educational materials to their patients. 4 Eighty percent of Americans have reported seeking medical information online. 5 In a typical day, this amounts to 8 million U.S. adults using the Internet to find information on various health topics. 6 Online health information has become an important resource for HIV information and support. A 2005 study of Internet-using HIV-positive men and women showed that health-related online searches were common, with Internet health-related searching associated with greater adherence and active coping. 7 More recently, the Internet was the fourth most used source of information on antiretroviral treatments (following physicians, HIV-related magazines, and drug ads) among a U.S. sample of primarily African American and Latino men living with HIV. 8
Given the widespread availability of HIV information found online, 9 the Internet may be an important resource for caregivers. A report on persons who said that the Internet was crucial or important during a loved one's health crisis (who were called “e-caregivers”) found that many credited the Internet with helping them find information (25%), support from other people (36%), and professional or expert services (34%). 10
While online health information and resource seeking continues to grow, 11 there have been no published studies of the ways in which caregivers of PLWHA use the Internet. The goals of this study were to: (1) describe the personal and demographic characteristics of a sample of HIV caregivers recruited online; (2) examine how they use the Internet for general and HIV-specific health information and resources; and (3) determine the degree to which caregiver role (informal, professional, or both informal and professional) is associated with the use of the Internet to provide HIV-specific support.
Method
Eligibility and recruitment
This study was conducted as part of a multimethod program of research 12 designed to understand how the Internet can be used to address the needs of PLWHA. Caregivers were recruited during a 5-week period (July to August 2008) using e-Rewards© (Dallas, TX), a nationally recognized market research company with online access to more than 2.6 million persons who agree to participate as survey “panelists” and fit a range of demographic profiles. Recruitment was stratified by ethnicity and race in an attempt to approximate the ethnic and racial distribution of persons living with HIV/AIDS. 13 Respondents were recruited by targeting two subgroups of e-Rewards © panelists. First, we sent an e-mail invitation to a sample of existing e-Rewards © panelists whose profile stated they live with or provide care for someone living with HIV (but were not HIV-positive themselves). Second, to maximize the number of non-white caregivers in the study, an e-mail was sent to racial and ethnic minority HIV-positive e-Rewards © panelists asking them to forward the invitation to someone close to them who may be interested in participating in the study (to whom we refer to as “nonpanelists”). Inclusion criteria for all respondents were: (1) 18 years of age or older; (2) English proficiency; (3) providing care and support for someone who is HIV-positive, defined as: “ … emotional, social, or financial in nature; giving advice or guidance; or helping out with chores or tasks. This can either be part of your job or just something you do as a family member or friend”; (4) self-reported HIV-negative; and (5) living in the United States or one of its territories. We considered allowing caregivers who were HIV-positive to participate in the study, but ultimately decided against it since this group may have different motivations for going online to seek general health and HIV-specific information and resources that would have been difficult to disentangle from those of caregivers not living with HIV/AIDS. Panelists completing the survey questionnaire were reimbursed $21 in e-Rewards © currency (redeemable for goods from a prespecified list of vendors), while nonpanelist respondents were mailed a check for $21 in cash by e-Rewards © .
Procedures
To ensure that each participant completing the online survey was a valid and unique respondent, 14,15 interested persons clicking on the invitation e-mail link were guided through a two-stage, online screening process. First, they were shown a list of characteristics (e.g., “I live with or support someone living with HIV”), and asked to check those characteristics that describe themselves or their situation (“prescreener” in Figure 1). Because e-Rewards © maintained a database of panelist sociodemographics, their responses could be authenticated against existing information. Non-panelists' responses could not be verified; nonetheless, they were required to indicate that they lived with or provided support to someone living with HIV in the pre-screener. Those eligible after pre-screening were passed into second-level screening for the remaining eligibility criteria (“study screener,” Figure 1). Those ineligible after either screening stage were thanked and redirected to the e-Rewards © website. Eligible respondents proceeded to a series of “chunked” (i.e., presenting key information on separate webpages to increase readability and understandability) informed consent pages, following best practices for Internet-based research. 16 All procedures were approved by the University of Minnesota and the Centers for Disease Control and Prevention Human Subjects Review Boards.
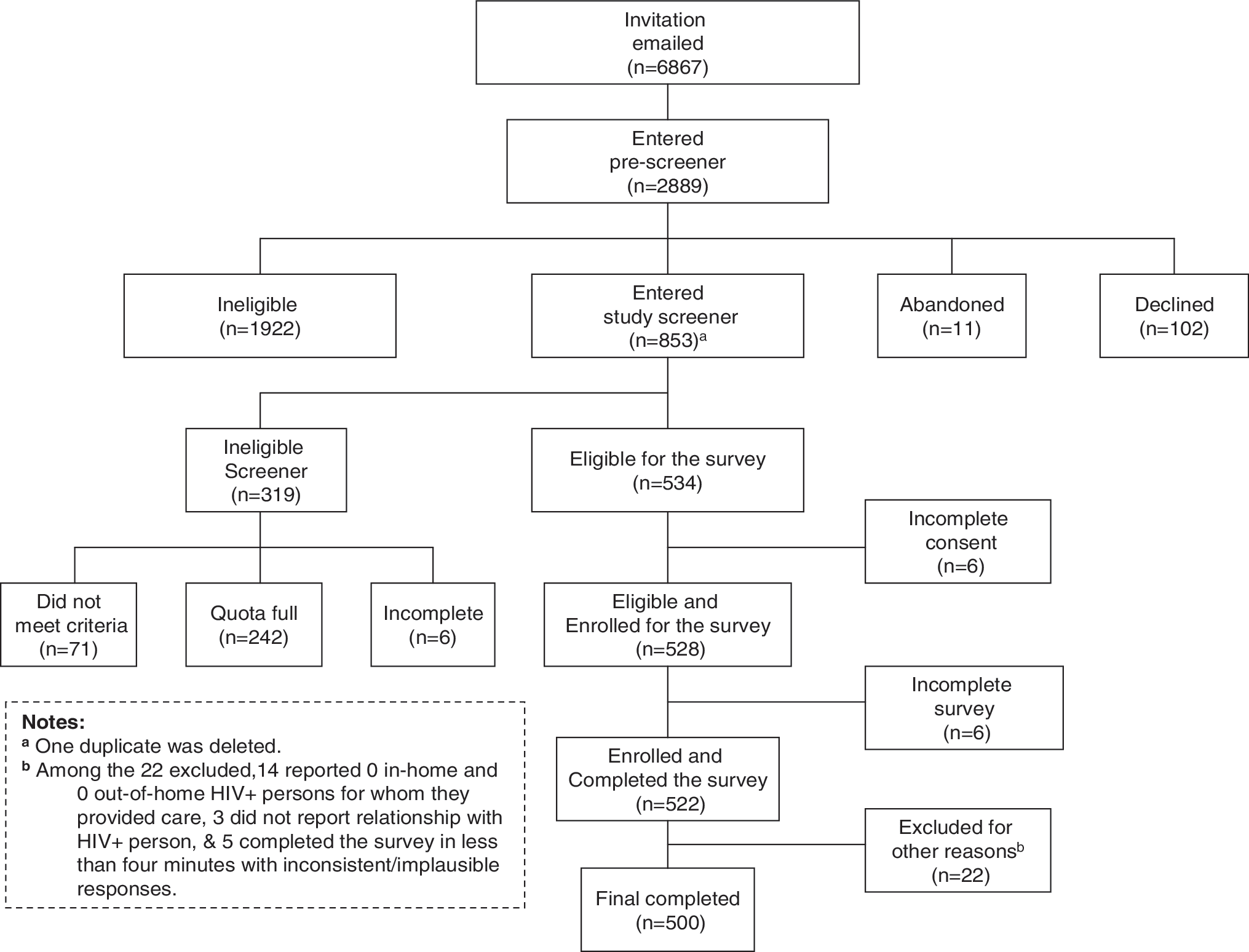
Flowchart of eligibity and recruitment.
Measures
Demographic characteristics recorded in the screener included age, gender, ethnicity, and race, education level, and sexual orientation. The online survey consisted of a total of 42 items. Internet experience was assessed by asking respondents how long ago they first used the Internet (less than 6 months, 6 months to less than 1 year, 1–3 years, 4–6 years, 7 or more years ago), which Internet connection speed they used to complete the survey (high speed, dial-up, or other), where they most often accessed the Internet (home, work, or somewhere else), and how many hours per week they used the Internet for personal reasons and work-related tasks.
Survey respondents were asked to report the number of PLWHA living in their household in the past year and, of those, how many were a spouse or domestic partner, child, friend, someone they supported as part of their job, or another type of relationship. A similar set of questions was asked about the number of PLWHA not living in their household to whom they provided care in the past year. Current use of the Internet for general health information and for HIV-specific purposes was assessed by asking respondents how many times in the past month they had engaged in the items presented in Table 1. In addition, respondents were asked the degree to which they agreed or disagreed with the statement, “The information I get on the Internet is very helpful for taking care of and providing support for HIV-positive people in my life” (1 = strongly disagree to 5 = strongly agree). To understand more specifically how caregivers used the Internet to provide support to PLWHA, they were asked whether they have never, once, or two or more times sent an HIV-positive person an e-mail with a website link or document found online, printed off information from a website and gave it to an HIV-positive person, or had a discussion with an HIV-positive person about something they found on the Internet (Table 2).
Percentage who reported engaging in activity at least once in the past 30 days.
Mean.
Median.
One missing case.
χ2 test.
Two missing cases.
Fisher's exact test.
Internet health seeking self-efficacy was measured using four items from the 10-item eHealth Literacy Scale (eHEALS), 17 that assesses “consumers' combined knowledge, comfort, and perceived skills at finding, evaluating, and applying electronic health information to health problems,” (article e27) and has shown good psychometric properties in a sample of youth. 17 To limit the length of the online survey, we chose the following four items: “I know how to find helpful resources on the Internet,” “I know how to use the Internet to answer my questions about health,” “I can tell high-quality health resources from low-quality health resources on the Internet,” and “I feel confident in using information from the Internet to make health decisions.” Response options were on a Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”).
Analyses
Data were analyzed using the statistical package STATA, version 9.2 (StataCorp, College Station, TX). Summary statistics included frequencies, percentages, means, and medians. Respondents were categorized into three mutually exclusive categories for the purposes of analyses: (1) those who exclusively provided care to PLWHA as a function of their personal relationship and not as part of their job (“informal” caregivers); (2) those who exclusively provided care to PLWHA as part of their job (“professional” caregivers); and (3) those who provided care both informally and as part of their job (“both” caregivers). Because few respondents identified as American Native/Native Alaskan (n = 6), this group was combined with Asian/Pacific Islander (n = 42) for the purpose of analyses. Chi-square, Fisher's exact, and Kruskal-Wallis tests were used to explore demographic, Internet use, and caregiving group differences.
The four items selected from the eHEALS scale showed good reliability (Cronbach α = 0.80) among this sample of caregivers. For each participant, the self-efficacy items were summed and divided by four to obtain a global index of self-efficacy for Internet health seeking. Next, because self-efficacy scores were not normally distributed (median = 4 on the 1–5 scale), a median split was used to divide scores into either high (scores ≥4) or low (scores <4) self-efficacy.
To examine the degree to which caregiver role was associated with using the Internet to provide support for HIV-positive persons (after adjusting for sociodemographic factors and self-efficacy), significant bivariate factors were entered into four logistic regression analyses of the main outcome variables of interest (see Table 3). Since outcome variables were ordinal-level (never, 1 time, or 2 or more times), we used either an ordinal logistic regression or an unconstrained partial proportional odds model 18 using the gologit2 command (when the parallel odds assumption was violated). 19
All outcome factors were categorized as never, once, or twice.
Odds ratio.
Not included in model since statistically insignificant in bivariate analysis.
Proportional odds assumption violated for “More than 1 race/ethnicity” in “Had a discussion” model with OR reported for odds of being in higher outcome group.
CI, confidence interval; OR, Odds ratio.
Results
Response and enrollment rates
Invitation e-mails were sent to 6867 individuals, of whom 2889 (42% initial response rate) entered the prescreener (Fig. 1). Among these respondents, 853 (29.5%) passed the caregiver prescreener; 63% (534/853) of eligible caregivers met the additional study criteria, and 528 completed the consent and enrollment process. Ninety-nine percent (522/528) of enrolled respondents completed the survey, of whom 22 were later withdrawn for a variety of reasons (e.g., reported 0 in-home and 0 out-of-home HIV-positive persons for whom they provided care, see Figure 1 for a list of reasons for withdrawal). The results discussed below describe the final sample of 500 caregivers. Among this group, the median survey completion time from the second screener to the final question was 10 minutes.
Demographics
Table 4 shows the personal and demographic characteristics for the sample and by caregiver role (informal, professional, and both informal and professional). Overall, caregivers were white, heterosexual, and highly educated, with a mean age of 39 years (standard deviation [SD] = 11.67). Fewer African Americans and Asian/Pacific Islanders and American Indian/Native Alaskans provided care informally compared to the other ethnic and racial groups (Fisher's exact, p = 0.013). A greater percentage of homosexual respondents provided informal care to PLWHA than those who identified as heterosexual or bisexual respondents (Fisher's exact, p = 0.000), while no bisexual respondents identified as informal and professional caregivers.
Informal, provides personal caregiving (e.g., as a friend) only; professional, provides job-related caregiving only; both, provides personal and job-related caregiving.
Two missing cases.
A/PI, Asian/Pacific Islander (n = 42).
AI/NA, American Indian/Native Alaskan (n = 6).
Ten missing cases.
Eighty-seven percent of the sample reported using the Internet for the first time 7 or more years ago. At the time they took the survey, 96% had a high-speed Internet connection and 72% reported accessing the Internet most often at home (i.e., as opposed to work or somewhere else). The median number of hours per week caregivers used the Internet for personal reasons and work-related tasks was 10 and 9, respectively.
Sixty percent of respondents reported providing care to PLWHA as a friend, 19% as a spouse, 17% as an “other family member,” 12% as a volunteer, 3% as a parent, and 3% as a child (not shown in tables). Exclusively providing informal care constituted 78% (391/500) of the sample. Overall, 22% reported providing support to PLWHA as part of their job, and roughly equal numbers reported caregiving in a professional capacity exclusively (n = 52) and caregiving informally and professionally (n = 57).
Use of the Internet for general Internet/health activities and HIV-specific activities
Table 1 shows the overall mean and median and group means of the number of times respondents used the Internet for general Internet and health information activities, as well as HIV-specific information and resources in the past 30 days. Nearly all respondents (98.6%) reported using the Internet for at least one of these activities in the past 30 days. The most common use of the Internet for general health included searching the Internet for a health topic (94%) and sharing the information found online with other people (80%). Specific to HIV, 72% of respondents visited a general medical website for HIV information, 44% shared information from the Internet with PLWHA, and 24% sought support groups for people who are caregivers of PLWHA. The right-hand column shows that, with the exceptions of searching the Internet for health topics and using e-mail to communicate with health care providers, those who provided care both informally and professionally used the Internet for general and HIV-specific purposes more than those who identified exclusively as informal or professional caregivers. The median self-efficacy index score was 4 (range 1– 5, M = 4.01). Professional (M = 4.27, SD = 0.72) and both informal and professional (M = 4.19, SD = 0.69) caregivers had higher self-efficacy index scores compared to informal caregivers (M = 3.94, SD = 0.72; F(2, 496) = 7.01, p = 0.001). Sixty-three percent of respondents (n = 314) were categorized as having high self-efficacy (scores ≥4).
Using the Internet to provide care for HIV-positive persons
Most (61.5%) respondents somewhat or strongly believed that the information they got online was very helpful for taking care of and providing support to PLWHA. Table 2 shows that respondents in this study used the Internet in a variety of ways to provide care and support to PLWHA. A greater percentage of the “both” group sent an HIV-positive person an e-mail with a website link, χ 2 (4, N = 499) = 21.57, p < 0.001, and printed off information from a website for an HIV-positive person, χ 2 (4, N = 498) = 29.38, p < 0.001, than members of the other groups. More professional caregivers had never sent an HIV-positive person an e-mail with a website link (58%) than informal caregivers (35%) or caregivers who functioned in both roles (23%), while more informal caregivers reported never printing off information for an HIV-positive person (40%) than members of the other groups (12%–17%).
Factors predicting the use of the Internet to provide support to PLWHA, adjusted for key sociodemographic variables, are shown in Table 3. Compared to informal caregivers, caregivers whose roles were both informal and professional had greater odds of recently sharing information from the Internet with PLWHA (OR = 2.03; 95%CI = 1.15–3.56) and ever printing off information from a website to give to PLWHA (OR = 3.87; 95% CI = 2.09–7.17). Compared to informal caregivers, exclusively professional caregivers had higher odds of ever printing off information from a website to give to PLWHA (OR = 1.87; 95% CI = 1.09–3.23), but lower odds of sending an e-mail with a website link (OR = 0.32; 95% CI = 0.18–0.60).
Discussion
The results of this study must be considered in the context of its limitations. First, the use of eRewards© to recruit respondents into this study limits the degree to which the results are generalizable to all HIV caregivers. Consistent with other online samples recruited in HIV-related studies, 20 this sample of caregivers appeared skewed toward those who were highly educated and Internet-savvy. However, the degree to which caregivers recruited from online marketing panels differ from other Internet-savvy caregivers or the general population awaits further study. Second, the cross-sectional design precluded causal inference of the impact of independent variables on outcomes. Third, in our decision to keep the online survey as brief as possible, other potentially important factors associated with providing care for HIV-positive persons may not have been assessed. For example, it is not known whether caregivers approve of or are willing to interact with online or electronic medical records on the behalf of HIV-positive individuals. Finally, although precautions were taken to detect and eliminate invalid responses (e.g., using a double screening strategy), the study relied on self-reported data that may be prone to error.
Although the Internet is only one of many sources for caregiver information and support, the results of this study begin to fill a gap in understanding of ways in which the Internet is used by persons to provide informal and professional care for PLWHA. Overall, this sample of caregivers used the Internet for a variety of health information purposes, social and supportive functions, and other health care functions. In addition, many caregivers used the Internet to provide support to PLWHA, with use differing by caregiver type (informal, professional, or both informal and professional). Each of these areas is discussed in turn below.
Caregivers in this study went online seeking general health and HIV-specific information. Consistent with prior reports 5,21 and unsurprising given the venue from which respondents were drawn, most caregivers in this study had searched the Internet for a health topic in the past month. The Internet was used also as a resource for HIV-specific information, with many visiting a general medical or HIV-specific website for HIV information or seeking information online about clinical trials for new HIV treatments. It may be that caregivers are more likely to use general medical websites for HIV information than HIV-specific websites because such sites offer “one-stop shopping” where information about their own personal health needs and the needs of PLWHA are provided. In addition, general medical websites may be more widely publicized and, therefore, more well-known in the general population, increasing the likelihood of their use. HIV-specific website administrators may consider partnering with general medical websites to increase their visibility and ultimately boost their readership. It is unknown the degree to which HIV-specific websites provide increased utility in terms of resources and services for consumers beyond those of general medical websites and warrants further study. Moreover, whether general medical or HIV-specific, the accuracy and credibility of HIV-related websites may be problematic. Nineteen percent of persons with chronic illnesses or disability report being confused by the types of information they found online, 22 and 9% report that the information they found online for a medical problem or condition was harmful. 6 A recent review of HIV-related webpages found that only 25% of webpages explicitly stated their contents were reviewed by an expert in the field. 23 Although not a focus of this study, the credibility of HIV-related websites remains a concern.
Among this sample of Internet-using caregivers, the Internet appears to serve as an important outlet to share general and HIV-specific health information with others. Online information sharing may provide an important approach for caregivers to obtain answers to complex HIV-related questions that are difficult to locate by conventional means (e.g., articles written in magazines or books). Similar to issues of credibility about HIV-related webpages discussed above, what is unknown is the accuracy of information shared between nonexperts about complex health issues such as HIV/AIDS. In addition, some caregivers went online for social and support purposes, including chatting or instant messaging with other people about health topics, using the Internet for support groups, and seeking support groups for people who are caregivers of PLWHA. Future studies should explore whether caregivers who socialize and seek support online have improved physical, mental, and emotional health outcomes compared to those who do not.
Using the Internet for health information may intersect with conventional medical care among caregivers and PLWHA in a variety of ways. One prior report noted that 69% of Internet-using persons with chronic conditions reported that the information they found online led them to ask a doctor new questions or seek a second opinion. 22 The results of this study showed that many caregivers used the Internet to inform health decisions for themselves and PLWHA. For example, nearly half of caregivers used e-mail to communicate with their health care provider and one third brought information that they found online to their physician. Specific to HIV, 16% of respondents reported sending an e-mail to a medical expert about HIV. The use of online resources to inform medical decisions and communicate with providers raises a number of complicated issues, including how doing so may affect the quality of the patient–provider relationship (e.g., does electronic communication increase the perceived trustworthiness or caring of the provider?) and the degree to which it improves or impedes treatment decisions.
An aim of this study was to examine how caregivers used online resources to support PLWHA, and the degree to which this differed by caregiver role. Just under half of all caregivers in this study shared information from the Internet with PLWHA. Caregiver role was associated with differences in general and specific online activities engaged in to support PLWHA. Generally, those who provided both professional and informal care shared information from the Internet with PLWHA more than caregivers who were exclusively in one of those roles. With respect to specific online activities, informal caregiving may have been more highly associated with sending an e-mail link to an HIV-positive person than professional caregiving because of the convenience of electronic communication and possibly because of concerns that professional caregivers may have about security and confidentiality of e-mail communication. Conversely, professional caregivers might prefer to print off HIV-related information during face-to-face appointments with patients. We anticipate that questions related to patient confidentiality, as well as the patient–provider relationship and treatment decision practices noted above, will continue to proliferate as technology is increasingly used to inform and manage medical illness. This study of caregivers was unique because of its recruitment strategy (i.e., the use of an Internet-based market research company rather than conventional online sources) and because caregivers represented diverse ethnic and racial backgrounds. The broad sample of caregivers obtained in this study may have decreased potential geographic and racial/ethnic biases in our findings related to Internet use practices. This sample of Internet-recruited caregivers was comparable in several respects to a recent study of clinic-recruited informal caregivers living in the northeast United States. 24 Slightly over half were female in both studies and most identified as Caucasian (53% of this sample versus 41% in the Engler et al. 24 study). However, at least one important difference was evident; most of the respondents in the current study (60% versus 19%) provided care to PLWHA as a friend, while only 19% (versus 47%) were the spouse or partners of a PLWHA. These differences likely reflect differences in recruitment sources and sampling strategies.
Implications
The results of this study contribute to our understanding of how caregivers utilize online resources to seek support for themselves and provide support to PLWHA. In light of these findings, websites that provide HIV-related resources may wish to consider the various ways in which caregivers use their content, and how utilization differs by role. While some HIV-related websites have created distinct online venues for caregivers that provide informal and professional support (e.g., The Body:
With respect to future research, more information is needed to understand how people providing care for PLWHA share information and support each other and the impact that doing so has on caregiver burden, as well as treatment outcomes for PLWHA. The Internet is used increasingly as a form of social networking, the advantages of which have been largely unstudied for HIV caregivers. In addition, we recommend further studies to understand why caregivers may not share information or resources found online with PLWHA and to examine how online HIV information seeking intersects with traditional medical management of HIV disease.
Footnotes
Acknowledgments
This study was funded by the Centers for Disease Control and Prevention Cooperative Agreement #5UR6PS000341. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.