
Abstract
With the rising incidence of HIV/AIDS in China, nurses will increasingly be caring for patients with HIV/AIDS. Thus, it is necessary that they have enough knowledge to reduce the risk of occupationally acquired HIV infection and that they change their attitude to care for HIV/AIDS patients. The objective of this study is to explore the relationship between student nurses' HIV/AIDS knowledge and their attitude using a structural equation model (SEM). A cross-sectional survey was conducted in January 2008 among 528 student nurses at the technical secondary school of the China Medical University. An SEM is proposed to determine the direction and magnitude of the interdependent effects between the latent factors. The SEM was built using LISREL version 8.5. The measurement properties of the latent factors underlying the questionnaire were based on a confirmatory factor analysis (CFA). Our results as following, HIV/AIDS knowledge and attitude may be measured by seven underlying constructs, namely, preventive knowledge, knowledge of transmission routes, specialty knowledge, knowledge of nontransmission routes, positive attitude toward HIV/AIDS, negative attitude toward HIV/AIDS, and occupational attitude. The SEM fits the data well. The interdependent relationships between these constructs identified the factors of preventive knowledge, specialty knowledge, and attitude toward HIV/AIDS as having both direct and indirect effects on occupational attitude. In conclusions, our results represent an initial effort to assess the relationship between student nurses' HIV/AIDS knowledge and their attitude toward the disease. CFA and SEM analysis have demonstrated their usefulness in evaluating multifactor complex constructs.
Introduction
C
Nursing students are important auxiliaries to clinical nurses. They are on the frontline of HIV prevention, care, and advocacy. Therefore, it is necessary that they have enough knowledge to reduce the risk of occupationally acquired HIV infection and that they change their attitude to care for HIV/AIDS patients when they enter clinical practice. Many studies have demonstrated that a large minority of nursing students had tremendous fears about the possibility of contracting HIV/AIDS. 7 –10 Huang et al. 10 found that nearly 1 in 4 students considered themselves to be at moderate to very high risk of contracting HIV among undergraduate students in China. Radecki et al. 11 found that significant decreases in personal fear and misgivings concerning HIV, coupled with a substantial decrease in the perceived need for testing of no-high-risk individuals, as respondents gained additional education and training. Cai et al. 7 observed that only 40.4% of medical professionals were willing to provide health care services for people living with HIV/AIDS in Southeast China. Enhanced education as well as specific programs promoting supportive attitudes and willingness to care is therefore required, especially among those working at lower facility levels in remote areas.
Investigating the relationship between nursing students' HIV/AIDS knowledge and their attitudes is essential to effectively improve HIV/AIDS professional educational programs. The knowledge and attitudes of nursing students regarding HIV/AIDS play an extremely important role in prevention and management. This raises questions about what will change the nursing students' attitudes toward caring for their patients with HIV and how knowledge influences attitude. However, there is no clear relationship between knowledge about HIV/AIDS transmission and prevention and willingness to care for patients with HIV.
In this study, we use structural equation modeling (SEM) to measure latent constructs, a method that is a relatively recent development in the literature. SEM provides researchers with a comprehensive means of assessing and modifying hypothetical models, thereby offering great potential to enhance the theoretical development of the initial structure based on exploratory factor analysis. The objectives are the following: (1) to determine the measurement properties of the latent factors underlying the HIV/AIDS questionnaire construct; (2) to explore and quantitatively analyze the relationship between HIV/AIDS knowledge and attitude; and (3) to provide a basis for future guidelines for a nursing student HIV/AIDS educational program.
Methods
A cross-sectional design was used. A cluster sampling method was used to select the study subjects. All 542 nursing students from three grade 12 classes that were going to begin clinical practice at the technical secondary school of the China Medical University were included in the study. A total of 528 valid questionnaires were collected. We used a self-administered HIV/AIDS questionnaire written in Chinese, the content of which was initially drafted based on the contents formulated by relevant previous studies. 12 –15
The study was based on an anonymous survey, and the results have remained confidential. The questionnaire did not contain any identifying information about the individual subjects. Participation in the study was totally voluntary, and the participants had the option of declining to answer specific questions or of leaving the entire questionnaire blank if they did not wish to participate. The participants were given the questionnaires on infection control and universal precautions during the class, and return them after class. The study protocol was approved by the bioethics advisory commission of the China Medical University, and all participants were provided with a written informed consent form before participating in the study.
HIV/AIDS knowledge was measured with a 18-item set of questions covering the basic characteristics of the disease, routes of viral transmission, and risk of occupational exposure. The knowledge questionnaire was reviewed for content validity by three experienced HIV/AIDS Chinese nurses and three epidemiology professors. The knowledge questions consisted of four basic subscales: preventive knowledge, knowledge of transmission routes, knowledge of nontransmission routes, and specialty knowledge. Respondents were given the option to reply that each statement was true or false or that they were uncertain. The attitude questionnaire was measured with a 15-item scale consisting of three subscales: positive attitude, negative attitude, and occupational attitude. Each item is attached to a four-point Likert-type response scale that ranges from “strongly disagree” to “strongly agree.” Numeric values for the scores ranged from “1” for “strongly disagree” to “6” for “strongly agree.”
A preliminary investigation of 50 randomly sampled nursing students was carried out 1 month before the formal investigation of the whole group. The purpose of the preliminary investigation was to select the most representative items from the questionnaire to ensure structural validity and increase the reliability of the investigation. All 50 students who participated in preliminary investigations were selected to the formal investigation. The results showed no significant difference between the 50 students and the others in formal investigation.
Exploratory factor analysis (EFA) was first applied to summarize the factor structure. The analysis was performed using principal axis factoring with varimax rotation on the correlations of the observed variables. The context and meaning of items were also taken into account during the EFA. Confirmatory factor analysis was used to assess the relationships between the latent constructs obtained from the preliminary EFA; to determine whether there was a construct common to these factors, the confirmatory factor analytic measurement model was fitted to the data. For both CFA and SEM, assessing the model's adequacy may be based on various measures. 16 –18 In the present study, we consider (1) the root mean square error of approximation (RMSEA), which should be below 0.05 for a good fit; (2) the Satorra–Bentler χ 2 ; (3) the standardized root mean square residual (SRMR); (4) the goodness-of-fit index (GFI), an index of the amount of variance and covariance explained by the model; (5) the adjusted goodness-of-fit index (AGFI), adjusted for the degrees of freedom in the model; and (6) the incremental fit index (IFI). Values greater than 0.80 for indices (4) to (6) indicate an adequate fit of the model. 19 –22
A hypothesized recursive structural equation model (SEM) was used to estimate the magnitude and direction of the interdependent effects between the factors that were identified as related. This general covariance structure contains both observed and latent variables. The factor score regressions obtained from the CFA were used to compute composite variable regression coefficients and measurement error variances for the SEM (error variances not accounted for by the latent factors). This process ensures that the estimation of the scale/composite variable is proportionally weighted by the actual contribution made by each observed variable, thereby minimizing the measurement error in the items contributing to each scale. This also has the advantage of increasing the reliability (and validity) of the computed scale scores. The composite scores were computed by multiplying the observed item scores by their proportionally weighted factor score regression coefficients, such that each factor score became a continuous variable ranging from 1 to 4. These composite variables were then used to examine the relationships between the latent variables underlying these composite scales.
The preliminary EFA of the data was performed using SPSS version 13.0 (SPSS Inc., Chicago, IL). The second-order CFA and the SEM were undertaken using LISREL 8.3.
Results
Participant characteristics
In this study, the participants were aged between 16 and 29 years old, with a mean age of 20.6 years (standard deviation [SD] = 1.9).
Reliability and validity analysis
The preliminary investigation with 50 nursing students had a Cronbach α coefficient of 0.74. An EFA was first applied to ensure structural validity. The analysis was performed using principal axis factoring with varimax rotation on the correlations of the observed variables. The Bartlett's test for sphericity was found to be significant (p < 0.01) while the Kaiser-Meyer-Olkin measure of sampling adequacy was 0.70, justifying the application of a factor-analytic procedure. Fifteen factors with eigenvalues greater than 1 were extracted, accounting for 74.3% of the variance. The remaining eight factors explained approximately 14% of the variability and were thus dropped from further analysis. After a substantial review of the literature, these factors were classified into several domains: preventive knowledge, transmission routes, specialty knowledge, nontransmission routes, positive attitude toward HIV/AIDS, negative attitude toward HIV/AIDS, and occupational attitude.
One month later, the formal investigation was carried out, with a Cronbach α coefficient of 0.84. The factor analysis demonstrates that the 7 factors extracted from the 33 items accounted for 87.2% of the variance.
Relationship between HIV/AIDS knowledge and attitudes
To assess the factor structure underlying the 33 items of the survey, a confirmatory factor-analytic measurement model was fitted to the data using the scaled covariance matrix of the polychoric correlations. In the solution, presented in Figure 1, seven correlated factors are labeled: preventive knowledge (η 1), transmission routes (η 2), specialty knowledge (η 3), nontransmission routes (η 4), positive attitude toward HIV/AIDS (η 5), negative attitude toward HIV/AIDS (η 6), and occupational attitude (η 7). To facilitate the interpretation of Figure 1, the seven factors are bounded by ellipses and the item descriptions within each first-order factor are bounded by rectangles. For example, the loading of the items for the “opportunities for growth” factor (η 3) ranged from 0.51 for “obvious symptoms and physical signs” to 0.60 for “dead from cancer and pneumonia.” It is evident that all the factor loadings were high (ranging from 0.37 to 0.78), indicating a strong association between each of the latent factors and their respective items. The factor loadings also made substantive sense, as they were meaningful and statistically significant. The relationships between the categories of preventive knowledge, transmission routes, specialty knowledge, nontransmission routes, attitude toward HIV/AIDS, and occupational attitude must also be significant. The results showed that convergent validity was achieved.
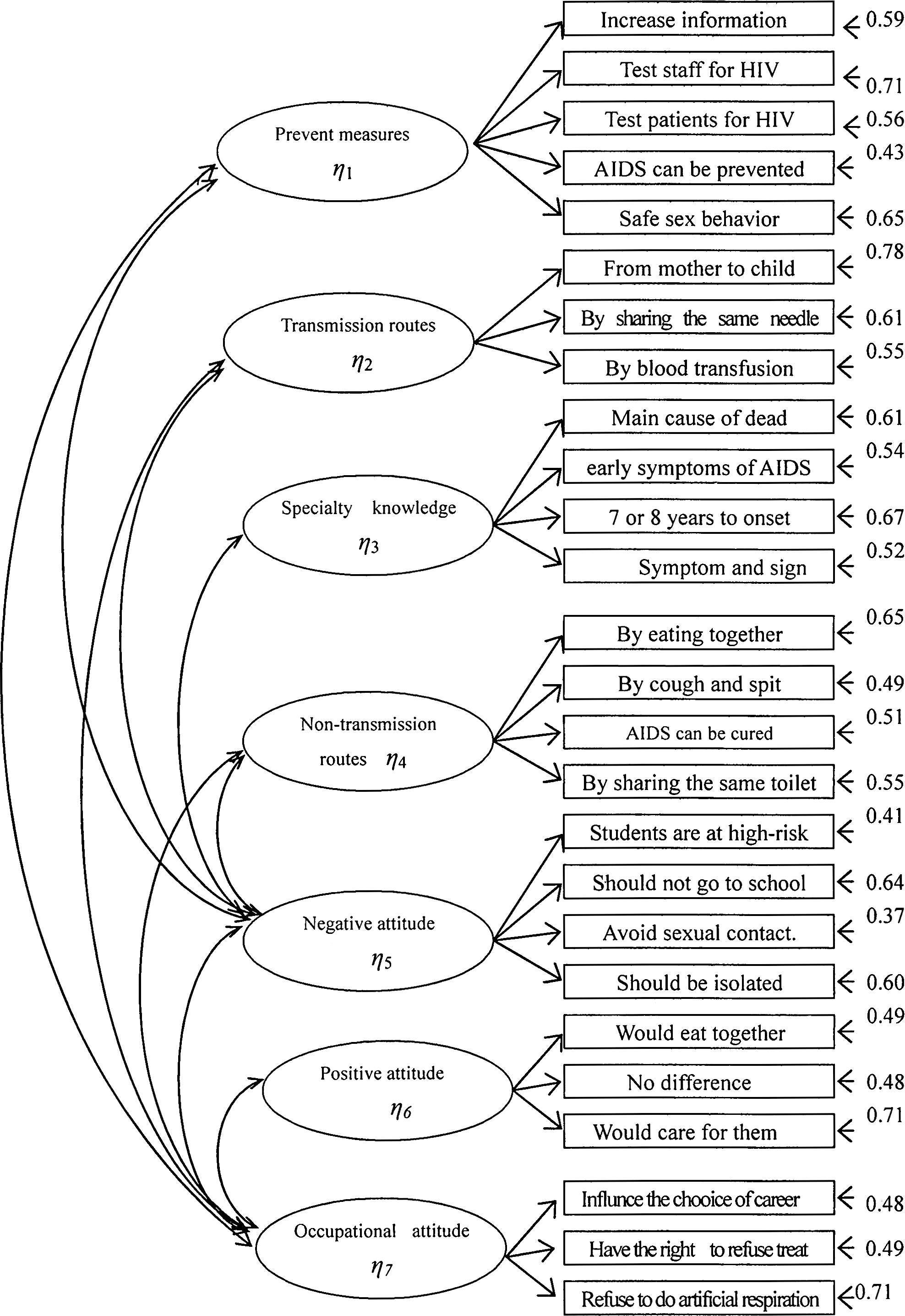
Completely standardized solution to confirmatory factor analysis (CFA) results.
As indicated by the CFA in Figure 1, the model accounted for 95% of the variance and covariance in the observed items. The Satorra-Bentler χ 2 was not significant. The RMSEA and SRMR values were 0.70 (p > 0.05). All other fit indices exceeded 0.80, indicating that there is no lack of fit, except for the GFI, which was 0.68. In the analyses reported here, no further modifications were performed on the model to achieve a better fit.
Relationship between HIV/AIDS knowledge and attitudes
To assess the relationships between the latent constructs and items obtained from the preliminary EFA and to determine whether there was a construct common to these factors, the confirmatory factor analytic measurement model was fitted to the data. A hypothesized recursive SEM was used to estimate the magnitude and direction of the interdependent effects between the factors identified to be related. This general covariance structure includes both observed and latent variables.
To estimate the direction and magnitude of the effects between the seven factors, a recursive SEM was fitted to the composite factor scores using the maximum likelihood estimation method. The best fitting solution is illustrated in Figure 2. The AGFI index indicated that 80% of the relative variance and covariance of the data was accounted for. All other indices and measures were satisfactory. The path coefficients proximal to the unidirectional arrows (from ellipse to ellipse), shown in Figure 2, are the standardized estimates of the direct effects of one factor score on the other. These may be interpreted as standardized regression coefficients. For example, an increase of one standard deviation in specialty knowledge (η 3) can lead to a corresponding increase of 0.31 standard deviation unit in occupational attitude score (η 7). All estimated path coefficients were significant.

Solution to recursive structural equation model (SEM).
Discussion
We assessed the relationship and the interdependent effects between seven latent factors. The findings have methodological implications for further research on the relationship between HIV/AIDS knowledge and attitudes toward the disease. Our measurement model provides preliminary support for the relationship between these two elements. The results provide further information on the interrelationships between the factors affecting nursing students' occupational attitudes.
Our results show that specialty knowledge, negative attitude, knowledge of transmission routes and knowledge of nontransmission routes had significant direct and indirect effects on occupational attitude. The results of Cai et al. 7 showed that knowledge and attitude scores as well as the proportion of those willing to provide care significantly differed by facility level and education might be promoted the willingness in southeast China. 7
Surprisingly, preventive knowledge and positive attitude had little effect on occupational attitude. It is also possible that the relationships between preventive knowledge, positive attitude, and occupational attitude are bidirectional. This result shows that it is important for nursing students to change their occupational attitude by acquiring specialty knowledge and knowledge of transmission and nontransmission routes and by reducing their negative attitudes toward HIV/AIDS. The results of Hu et al. 23 showed that those feeling morally responsible and those being able to treat infected patients safely were more willing to treat infected patients. Chen et al.'s 15 results showed that nurses who have a better understanding of HIV/AIDS prevention are more likely to have negative attitudes toward HIV/AIDS. So if we only disseminate preventive knowledge and promote a positive attitude, the results are likely to be unsatisfactory.
There are three main factors that had significant direct and indirect effects on negative attitude: knowledge of transmission and nontransmission routes, and specialty knowledge. Bird et al. 24 found that experiences with discrimination when receiving treatment have important implications for the health and health care of HIV-positive individuals. So it is important to change the negative attitude. The main factor influencing negative attitudes was knowledge of nontransmission routes such as eating together, coughing or spitting, sharing a toilet, etc. Lack of knowledge of nontransmission routes of HIV/AIDS is the main reason behind HIV/AIDS-related panic. Quach et al. 25 found that there were misconceptions on nontransmission routes and the one third of participants who reported positive attitudes regarding their interaction with HIV/AIDS patients were less likely to support mandatory testing or to exclude HIV/AIDS patients from their practices. Therefore, we can change nursing students' work attitudes indirectly by teaching about HIV/AIDS nontransmission routes. The results also show that specialty knowledge have significant direct and indirect effects on positive attitude toward HIV/AIDS. Suominen et al. 26 found that nurses and students who had previous experience of nursing an HIV/AIDS patient reported more cautious perceptions than those who did not. Health care personnel should have the opportunity in their training to work with HIV/AIDS patients. Therefore, we can improve nursing students' attitude toward HIV/AIDS by teaching specialty knowledge.
Various statistical criteria have been used to guide the selection of items for the CFA. The meaning and context of individual items should be taken into account during the selection process. We further note that alternative models could fit the observed data equally well, resulting in potentially different interpretations. In the present study, we assumed that the relationships between the six factors were recursive. It is possible that some of the relationships are bidirectional, especially the relationships between occupational attitude and other factors. Another limitation of the SEM approach is the requirement of large sample sizes for parameter estimation in the presence of many latent variables and/or a large number of items.
Footnotes
Acknowledgment
This work was supported by the National Natural Science Foundation of China (30700690), and the Foundation for the Educational Department of the Liaoning Province of China (20061020).
Author Disclosure Statement
No competing financial interests exist.