
Abstract
Evidence suggests that persons living with HIV (PLWH) are at increased risk for anal cancer. Early detection of anal cancer is an important prevention measure, but screening rates have been low. This report describes the experience of a quality improvement initiative to increase anal cancer screening at an HIV-specialty clinic. Chart reviews were conducted for three time periods: baseline year, prior to program discussion; transition year, during planning; and implementation year, during program availability. Odds ratios using Fisher's exact test showed that the odds of receiving anal cancer screening increased significantly in the transition year, odds ratio (OR) = 2.859, 95% confidence interval (CI): [1.798; 4.546], Fisher's z = 4.40, p < 0.0001, and in the implementation year, OR = 7.446, 95% CI: [4.783; 11.588], Fisher's z > 8.2, p < 0.0001. Patients and clinicians reported high levels of satisfaction with the program. Referring clinicians were also more likely to discuss anal cancer screening.
Introduction
W
Chemotherapy and radiation remain the preferred treatments for SCCA. Data suggest that treatment outcomes for SCCA in PLWH are similar to those in persons without HIV. 9,10 Therefore, some experts have advocated for early identification of anal cancer as a way of improving survival and outcomes for persons diagnosed with SCCA. 8,11 –14
The development of SCCA has been linked to the precursor lesion of anal intraepithelial neoplasia (AIN). 15 This is similar to cervical intraepithelial neoplasia (CIN), the precursor for cervical cancer. Given the similarities between AIN and CIN, the methodology used for detecting CIN have been adopted for the anal canal, namely the use of anal cytology (anal Papanicolaou or anal Pap). 15 –18 The sensitivity and specificity of anal cytology is varied, with sensitivity ranging from 40% to 90% and specificity ranging from 8% to more than 60%. 19 It is clear that anal cytology may not be the ideal screening test, however, it remains one of the only currently available methods to detect anal dysplasia. The paucity of data regarding the natural history of anal HPV infection, along with the variability of diagnostic specificity has contributed to the limited adoption of anal cytology for routine screening, and in some centers this practice is still considered controversial. 17,19
Some experts believe that universal implementation of anal cytology screening is further hindered by the lack of infrastructure in many institutions to address abnormal results. 15,16 One of the dilemmas that arises for primary care HIV clinicians is the limited availability of experts who can adequately care for patients found to have abnormal cytology. 9 If a patient is discovered to have abnormal cytology and no follow-up is available, this can lead to undue anxiety for patients and pose a dilemma for clinicians. Therefore, many providers elect not to perform anal cytology.
In centers that are able to provide comprehensive anal dysplasia screening, patients with abnormal cytology are referred for high-resolution anoscopy (HRA), the equivalent of cervical colposcopy. 9 HRA uses a magnification process to examine tissue for dysplastic changes. Currently, few clinicians are trained to perform HRA in the United States. However, given the increased interest in anal cancer and anal dysplasia, more and more HIV treatment centers are now training clinicians to perform HRA through formal courses offered by the American Society for Colposcopy and Cervical Pathology (ASCCP).
Screening recommendations
Even though there are no consensus guidelines regarding the universal use of anal cytology, the U.S. Department of Health and Human Services (DHHS), American Cancer Society, American Society of Colorectal Surgeons, and HIV Medicine Association of the Infectious Diseases Society of America all endorse early detection of anal cancer in PLWH. These authorities suggest that anal cancer screening with digital rectal exam (DRE) be considered a part of routine screening for PLWH. 12,15,20,21 The U.S. DHHS published guidelines in 2009 that addresses the importance of annual DRE to detect any masses, plus anal cytology as an option for those with appropriate resources and expertise in interpreting and managing abnormal screening results. 21 The New York State Department of Health AIDS Institute recommends that clinicians perform an annual DRE on all HIV-infected persons, with additional anal cytology screening in the following HIV-infected populations: (1) men who have sex with men (MSM), (2) any patient with a history of anal condyloma, and (3) women with abnormal cervical or vulvar histology. 22 HIVQUAL-US, an organizational entity comprising expert HIV clinicians, and supported in part by the U.S. DHHS, produces a list of quality indicators for the treatment of PLWH. DRE was recently added as part of the newest set of HIV quality indicators with anal cytology also listed as an optional indicator. 23
Given the complications of advanced cancer and the fact that early identification and treatment may result in improved health outcomes, it is imperative that PLWH be screened regularly for anal cancer. A recent report by Rosa-Cunha and colleagues 24 found that patients were rarely asked about anal health during routine office visits. Another report that examined compliance with HIV-related quality indicators in federally funded HIV treatment centers in the United States found that routine screening for anal cancer was low. 25 The median percent of HIV-infected MSM who received an annual DRE in 2007 was estimated to be 17.4%, and the median percent of HIV-infected MSM who received anal cytology was 12.5%. 25
A project to increase anal cancer screening
As part of an ongoing quality improvement initiative at the University of Colorado's Infectious Disease Group Practice, clinic providers were surveyed regarding their adherence to routine prevention measures, including immunizations and screenings for colon cancer, cervical cancer, and anal cancer. Clinicians identified low compliance with the recommendation for annual DRE, with more than 80% of clinicians reporting not screening or rarely screening patients for anal cancer on a routine basis. A baseline chart review estimated the clinic's compliance with anal cancer screening to be 10% in 2007.
In 2008, a working group consisting of key opinion leaders and stakeholders within the Infectious Disease Group Practice was formed to address this opportunity for practice improvement. The working group developed a quality improvement strategy to increase compliance with anal cancer screening recommendations. Discussions with providers in the clinic identified the key barriers to screening as a lack of time to screen during routine office visits and a lack of appropriate referral resources for patients with abnormal cytology results.
The working group suggested the development of a comprehensive anal health program to address these barriers. Similar programs exist at other HIV treatment centers across the United States, most notably in San Francisco, New York, Seattle, Boston, San Diego, and Philadelphia. 26 The anal health program was developed with the intent of offering patients a screening DRE, anal cytology, HRA for patients with abnormal cytology results, and treatment for patients with confirmed high-grade dysplasia. The working group met with representatives from surgery, oncology, and pathology. The working group wanted to ensure that a comprehensive treatment plan would be feasible in the event that a patient needed additional services that were beyond the scope of the anal health program such as radiation or surgical management of identified cancers. The team also met with a local HRA and anal dysplasia expert to obtain recommendations on implementing a comprehensive treatment program.
The anal health program was launched in early 2009. For patients with biopsy proven high grade AIN (HG-AIN), topical treatment with infrared coagulation (IRC) was also provided. IRC is a heat-based treatment that has been shown to effectively treat HG-AIN. 27 Overall setup costs, including education and training, were estimated to be approximately $12,000 (U.S.). The program was evaluated in terms of its effect on clinic providers' compliance with the recommendation that all PWLH receive regular anal cancer screening; patient and provider satisfaction with the program were also assessed.
Methods
Procedure
After receiving approval from the Colorado Multiple Institutional Review Board, chart reviews were conducted for three 12-month time periods: (1) the baseline year (2007) prior to any discussion of a dedicated anal health program, (2) the transition year (2008) during which preliminary plans were developed and a working group was formed, and (3) the implementation year (2009) when the anal health program offered services to patients. An online sample size calculator (
A list containing the medical record numbers of all patients seen in the Infectious Disease Group Practice during each 12-month time period was obtained by searching the billing and scheduling system. Only patients with an ICD-9 code of VO8 (asymptomatic HIV) or 042 (HIV disease) were included in the master list for each year. The list was screened for duplicates until a final list of unduplicated patients was obtained. A random number generator was used to determine which charts to include for analysis. Due to issues with confidentiality, only the primary outcome measure (presence of DRE or anal cytology) was recorded, therefore intraindividual correlation between each time period could not be calculated. Patient satisfaction was assessed via a voluntary self-administered questionnaire that was provided to patients at the conclusion of their visit. Provider satisfaction was assessed through an anonymous online survey.
Measures
Charts were reviewed by the first author for documentation of a DRE and/or anal cytology. Results were recorded without patient identifiers in a Microsoft Excel spreadsheet (Microsoft, Redmond, WA).
Patient satisfaction was measured using a self-administered 18-item questionnaire adapted from a validated patient satisfaction measure for colon cancer screening. 28 The wording of the questions remained structurally the same, but the terms used were modified to reflect procedures performed in the anal health program. Items were scored on a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree. Several items were reversed coded in order to keep the scoring system consistent and to assist with analysis. Based on an exploratory factor analysis, three subscales were identified for this revised measure: satisfaction with the clinic, satisfaction with the experience, and patient distress. Three items did not show communality with other items (wait time, clinic location, and schedule availability), so those results were analyzed separately. Cronbach α showed high internal consistency for the “satisfaction with clinical program subscale” (Cronbach α = 0.866) and the “satisfaction with exam experience subscale” (Cronbach α = 0.873). The patient distress scale only had two items, leading to a low Cronbach α (Cronbach α = 0.550).
Finally, providers' behavior and satisfaction were assessed by an anonymous survey administered after the end of the first year of implementation. This survey was developed by the first author. Psychometric analysis could not be performed because of the limited number of possible respondents among clinic staff. Providers were asked about the likelihood that they would discuss anal cancer screening with patients, perform screening examinations on their own patients, and refer patients to the anal health program for screening. Clinicians were also asked about their satisfaction with the services received by patients they had referred to the anal health program.
Analysis plan
Fisher's exact test was used to determine the significance of change in the percent of patients receiving anal cancer screening in the baseline year compared to each of the subsequent years. Additional comparison between the transition year and the implementation year was also assessed. Odds ratios with 95% confidence intervals were computed using the VassarStats online statistical calculation website (
Factor analysis was performed on the patient satisfaction questionnaire, and a three-factor solution was the most interpretable; therefore, descriptive statistics were used to summarize patients' responses on each of the three identified patient satisfaction subscales. Descriptive statistics were also used to summarize responses on the provider questionnaire. Descriptive analyses were performed using IBM SPSS version 18.0 (SPSS, Inc., Chicago, IL).
Results
The anal health clinic had a total of 128 visits in its first 12 months of operation (the implementation year). The majority of visits were for general screening (53%), which included DRE and anal cytology. Thirty percent of visits were for follow-up and/or consultation for abnormal anal cytology results or abnormal findings on DRE. One case of SCCA was identified in the anal health program. The percentage of patients in the entire practice who received a DRE or anal cytology screen improved significantly over the course of the 3-year period (Fig. 1). Compared to the baseline year, screening rates increased significantly between the baseline, transition, and implementation years (Table 1).
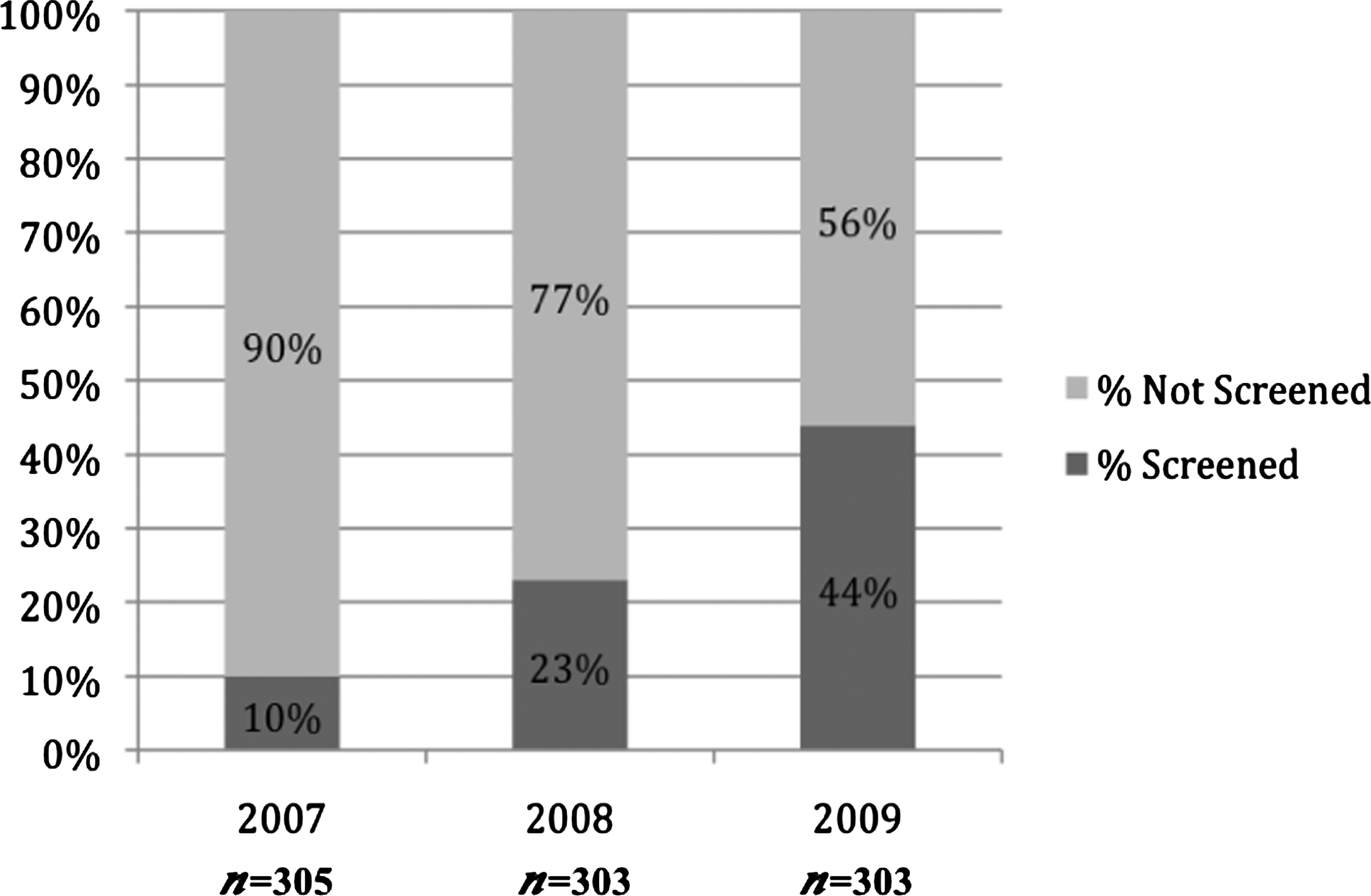
Chart review data: percentage of patients receiving anal cancer screening either by digital rectal exam (DRE) and/or cytology.
Note: The first year listed in each comparison is the reference year.
OR, odds ratio; CI, confidence interval.
Patients' overall satisfaction with the anal health program was high. A total of 62 patient satisfaction surveys were collected between October 1, 2009 and February 28, 2010, representing an 86% response rate among patients seen in the anal health program during that time period. Results showed high satisfaction with the clinic and with the screening experience. Low levels of patient distress were also found (Table 2).
Mean Score: 1 = strongly disagree to 5 = strongly agree.
Reverse coded items.
Provider survey results were positive. There was an 89% satisfaction survey response rate among clinicians in the Infectious Disease Group Practice. Respondents reported that, with the availability of the anal health program, they were more likely to discuss anal cancer screening; 87.5% said they were likely to refer their patients to the program for screening. In addition, 62% of respondents reported doing more of their own anal cancer screening examinations after the anal health program started. Most respondents (87%) reported making at least one referral to the anal health program in the previous 12 months and 100% of those who referred a patient reported being satisfied or very satisfied with the services their patients received. Clinicians who had not made a referral reported screening and managing their own patients.
Limitations
One of the limitations of this analysis relates to the potential for external factors that may have prompted additional screening, such as the release of several studies in 2009 highlighting the growing burden of anal cancer in PLWH. 4,5 Additionally, this report looked only at the number of patients who actually received a screening exam. Due to inconsistencies with documentation among clinicians, patients who were offered a screening examination but refused were not captured. Furthermore, some individuals may have received examinations that were not documented in the medical records.
In an effort to preserve patient confidentiality and the way in which the evaluation plan was designed, chart review data only captured evidence of an anal health examination, other patient characteristics were not recorded. Therefore multiple regression analysis to assess for other confounding factors that may have influenced screening was not performed. However, the patient population remained relatively stable over the course of the 3 years, so the potential for a demographic shift that may explain the observed results is low.
Further limitations of the patient satisfaction survey were the need for additional instrument validation and the potential for positive response bias. To our knowledge, there were no validated patient satisfaction survey instruments for use in this particular setting or with these types of procedures. A prior survey instrument focused on flexible sigmoidoscopy was adapted for use in our study and, although factor analysis identified three potential subscales, additional validation in other populations is needed. Furthermore, although the questionnaire was voluntary and anonymous, some individuals may have felt compelled to give higher scores because only one clinician provided HRA services during the evaluation period and some patients might have felt their care would be compromised by a low rating. However, this potential source of bias most likely did not have a strong influence on the patient satisfaction results, as care was taken to minimize this impression for patients by emphasizing the importance of honest answers. In addition, patients completed the questionnaire only after all treatment was completed.
With regard to the provider satisfaction survey, although it was anonymous the potential for biased responses existed because respondents were colleagues of the primary author and may have felt a need to rate the services provided more favorably. Additionally, some of the respondents were involved in the overall conception and design of the anal health program, so there was also a potential for investigator allegiance.
Conclusion
This quality improvement project demonstrates the ability of a dedicated anal health program to improve compliance with one of the newest HIV primary care quality indicators. Clearly, the anal health program did not conduct all of the exams in the clinic. However, the dedicated program addressed one of the perceived barriers to screening, which was an infrastructure for treating patients found to have abnormal cytology or physical exam findings. By addressing a major clinician-perceived organizational barrier, the anal health program provided more opportunities for clinicians to discuss anal cancer screening, perform their own exams, and/or refer patients for a focused examination. This combination of factors resulted in an overall increase in the number of patients screened in the clinic.
Findings from this quality improvement program echoed findings of a previous study reported by the University of California, San Diego in 2001. 14 Matthews and colleagues 14 found that the percentage of patients receiving anal cancer screening via anal cytology was 73% by the end of the 5-year study period. As the University of Colorado's anal health program continues to expand, it is anticipated that the anal cancer screening rate will approach that in other HIV treatment centers with regular access to anal dysplasia specialists.
The challenges of implementing an anal dysplasia program have been described by others. 26,29 HIV treatment centers considering an anal health program should have a clear plan that addresses the scope of services offered, the equipment and training needs of the providers, and appropriate protocols for follow-up care. From a quality improvement standpoint, this report demonstrates that a dedicated anal health program is feasible, and can be implemented to improve the rate of anal cancer screening for PLWH. Although not a part of this current program, a dedicated anal health program could also integrate other services such as screening for asymptomatic sexually transmitted infections as has been advocated by other public health experts. 30 As further research and data become available on the burden of SCCA in PLWH, centers that provide primary HIV care services must find methods to improve SCCA identification in order to address this growing comorbidity in the current era of HIV.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the Anal Health Working Group, the staff of the Infectious Disease Group Practice, and the patients who participated in this project.
Author Disclosure Statement
Jeffrey Kwong—Speakers Bureau, Gilead Sciences, Inc. Paul Cook and Lucy Bradley-Springer have no disclosures.