
Abstract
HIV-associated neurocognitive disorders (HAND) remain prevalent, especially in regions like South Africa where HIV prevalence is high but access to antiretroviral treatment (ART) is limited. The incidence of HIV dementia (HAD) has been halved with the use of ART, but the prevalence remains high. Appropriate brief screening tools to screen for HAD are needed in order to facilitate treatment initiation. The validity of the International HIV Dementia Scale has not been established in a region where infection with HIV clade C is predominant. The International HIV Dementia Scale (IHDS) was administered together with a detailed neuropsychological test battery to 96 HIV-positive individuals who had not received ART and who were attending primary care HIV clinics. The validity of the IHDS was established using a receiver operating characteristic (ROC) analysis. HIV-positive individuals displayed greater impairment when compared to HIV-negative controls on the IHDS and a range of neuropsychological tests. Neuropsychological tests discriminated well across HAND categories for HIV-positive individuals. In ROC analysis, the IHDS showed an area under the curve of 0.64, with a sensitivity of 45% and specificity of 79% at a cutoff score of 10. Individuals with HAD, who screened negative on the IHDS, performed poorly on some tests of executive function. These data suggest that the IHDS may have limitations as a tool to screen for HAD in South Africans infected with HIV. Variable performance in neuropsychological testing may account for false negative screens. The inclusion of brief tests of executive function in a screening battery should be considered.
Introduction
H
Formal neuropsychological testing remains the gold standard of diagnosis of HAND. 10,11 While most studies report a typical pattern of neuropsychological impairment, involving executive functions, motor functions, speed of processing, and impaired recall, there is evidence to suggest a wider variability of deficits. 12 Neuropsychological deficits in HAND are thought to track the brain regions primarily involved affected by HIV, namely the subcortex and striatum. 11 Accordingly, impairments of executive dysfunction, motor slowing, impaired speed of processing, and impaired memory recall are regarded as characteristic of HAND. 1 Neuropsychological test batteries need to sample across a number of domains in order to detect impairment. Furthermore, the application of neuropsychological testing is well known to be dependent on a range of factors including age, culture, language, level of education, and the presence of comorbid neurologic problems, such as substance abuse. 2 –4,13
A number of brief screening tools have been proposed for use in primary health care and resource-limited settings. These include the HIV Dementia Assessment, HIV Dementia Scale (HDS), and the International HIV Dementia Scale (IHDS). 14 –16 The IHDS has been validated in both the United States, Spanish-speakers, and Uganda. 15,17 Both the HDS and IHDS were found to be useful tools in a smaller study in Canada. 18 The development of an appropriate screening tool for HAND first requires detailed neuropsychological characterization of impairments that may be affected by regional differences, such as culture, language, or clade differences. 2,19 Differences in the neurotoxic effects of the different HIV clades have been proposed, although early clinical studies suggest that clade C, common in South Africa, may produce high rates of HAND. 19 The validity of a brief screening tool would then need to be validated across different settings.
A number of potential issues need to be considered when making use of screening tools. These include the need to be brief, easy for nonspecialists to administer, and adaptable for use in cross-cultural settings. Also, a screening tool should be both as sensitive and specific to HAND, taking into account neuropsychological functions commonly thought to be affected by HIV. The IHDS includes three subtests: a nondominant finger-tapping test, a nondominant Luria hand sequence, and a four-word recall test. The IHDS was validated in an American and Ugandan sample, and was found to have a sensitivity and specificity in the Uganda sample of 80% and 55%, respectively. 15 More recently, the IHDS was compared to a brief neuropsychological battery in Canada, where a receiver operating characteristic (ROC) analysis generated an area under the curve of 0.74. 18 The authors reported that the HDS and IHDS were relatively efficient in diagnosing HAND, with the IHDS displaying a sensitivity and specificity of 76.9% and 65%, respectively. 19 Further studies in regions of high HIV prevalence and unique clade sequencing are needed.
In the present study we aimed to describe the performance of the IHDS against categories of HAND defined by the updated American Academy of Neurology criteria. We examined scores from a detailed neuropsychological battery in a sample of clade C HIV-positive individuals, compared to a group of HIV negative controls.
Methods
Subjects
This study formed part of a larger investigation of HIV-associated neurocognitive disorders in Cape Town, South Africa. In summary, 283 HIV-infected individuals at three primary health care centers were invited to participate from February 2008 through August 2009. Of these, 163 attended two full-study visits during which detailed sociodemographic, neuromedical, neuropsychological, and laboratory measures were administered. The evaluations took between 2 and 3 h, and were conducted by trained technicians in the participants' first language. Details of this characterization have been previously published. 7 Of the 163 individuals characterized, 96 received the IHDS in addition to the above assessments and were included in this analysis. The IHDS was administered by the medical doctor as part of the neuromedical assessment. Included individuals ranged from 18 through 40 years of age, and were assessed prior to commencing treatment with ART. In order to exclude neuropsychiatric confounders to neuropsychological test performance, potential participants were administered a number of instruments including the Alcohol Use Disorders Identification Test (AUDIT), the Centers for Epidemiologic Screening-Depression tool (CES-D), and the MINI Neuropsychiatric Interview (MINI). All have been validated and used in South Africa. 20 Participants were excluded if they had a severe psychiatric disorder (such as schizophrenia or bipolar disorder), recent history of substance abuse or significant neurologic disorder (such as epilepsy or significant head injury with loss of consciousness more than 30 min). Also, while hepatitis C coinfection is known to contribute to neuropsychological impairment, rates of infection in South African clinic settings are relatively low. 21
All participants who met study criteria and agreed to participate provided written informed consent. Approval to conduct the study was obtained from the Research Ethics Committee of the Faculty of Health Sciences, University of Cape Town, and from the relevant clinic authorities.
Neuropsychological test battery
A neuropsychological test battery was administered to all participants to assess specific domains of neurocognitive function. The battery comprised tests of attention (the Mental Alternation Test [MAT] and the Mental Control Test [MCT]), learning and memory (the Hopkins Verbal Learning Test [HVLT] and the Brief Visuospatial Memory Test [BVMT]), motor (Finger Tapping [FT] and the Grooved Pegboard Test [GPT]), psychomotor speed (Trail Making Test part A [TMTA], Color Trails Test 1 [CT1] and Digit Symbol-Coding [DSC]), executive function (Color Trails Test 2 [CT2], Stroop Colour-Word test [SCW], Wisconsin Card-Sorting Test [WCST], and category fluency-including an animal list and a fruit and vegetable list).
Control data for neuropsychological testing was obtained from 94 HIV-negative participants. These participants were recruited from voluntary counseling and testing services at the same primary care clinics. Other than being HIV negative, as confirmed by a recent rapid HIV test and confirmatory serologic test done at the study visit, inclusion and exclusion criteria were identical to those applied to HIV-positive participants. The CD4 cell count was obtained from the clinic records. Data from the 94 HIV-negative controls were used to generate z-scores for establishing the degree of impairment for each test. No published norms are currently available in South Africa, and as most participants spoke isiXhosa, we elected to generate control data from similar community participants.
The IHDS was administered by medical officers trained in HIV neuropsychiatry. A uniform approach was ensured through the study leader. The IHDS was administered during the same visit as the study neuromedical assessment.
Determination of neurocognitive disorder status
We used the above neuropsychological test battery, and an evaluation of functional assessment (the Patients' Assessment of Own Function [PAOFI] and the Quality of Life and Enjoyment Satisfaction Questionnaire [QLESQ]), to classify participants into one of four HAND categories, based on the updated criteria published by Antinori and colleagues 22 : no impairment, asymptomatic neuropsychological impairment (ANI), mild neurocognitive disorder (MND), and HAD. Individuals who scored more than two standard deviations (SDs) below the mean on at least two domains of function, and were noted to have significant functional impairment on self-report, were classified as having HAD. Those who displayed impairment between one and two SDs, were classified either as MND or ANI, depending on the presence or absence of functional impairment. The remaining participants were classified as nonimpaired. The final classification was conducted by a consensus panel comprising two HIV neuropsychiatrists and a neurologist.
Statistical analysis
Data were analyzed using STATA 11 (Stata Corporation, College Station, TX). The HIV-positive and HIV-negative groups were compared with respect to age, level of education, and neuropsychological test characteristics using unpaired t tests, and with respect to gender distribution using a Fisher's exact test. The HAND categories of HIV-positive participants were compared using Kruskal-Wallis tests for differences between medians of multiple groups. The difference between the means of the HAD group and the remaining participants were compared using an unpaired t test. The ability of the IHDS to predict HAD was established using a receiver operating characteristic curve, and cutoff scores calculated from this. Correlations between the IHDS total score and subtest scores were calculated for each neuropsychological test, and r values reported. p Values were regarded as significant at the 5% level.
Results
The demographic characteristics of the HIV-negative and HIV-positive groups are shown in Table 1. There were significant between-group differences in terms of age and level of education, but not gender distribution. There were also significant between-group differences in performance on a number of neuropsychological tests within each domain. In order to establish whether age and education effects contributed significantly to total IHDS scores, we conducted unadjusted and adjusted associations for these variables, together with HIV serostatus. In the unadjusted models for HIV positive and negative participants, age was not significantly associated with IHDS total score (p = 0.178, coefficient −0.0, 95% confidence interval [CI] −0.14–0.03 and p = 0.073, coefficient −0.4, 95% CI −0.09–0.01, respectively). Level of education was a significant predictor of IHDS total score in unadjusted association for the HIV-negative group (p = 0.014) but not the HIV-positive group (p = 0.096). In an adjusted model including age, education, and HIV serostatus, only education was significant (p = 0.014).
Effect size of between-group differences in test/subtest performance HIV-negative vs. HIV positive participants.
IHDS, International HIV Dementia Scale; FT, Finger Tapping Test; GP, Grooved Pegboard Test; HVLT, Hopkins Verbal Learning Test; BVMT, Brief Visuospatial Memory Test; MAT, Mental Alternation Test; TMTA, Trail Making Test part A; WCST, Wisconsin Card-Sorting Test.
Regarding the screening test (IHDS), the only test for which there was no significant between-group difference was the Luria sequence nondominant hand (p = 0.94). HIV-positive participants performed significantly more poorly than HIV-negative controls on all other neuropsychological tests, other than the MAT (p = 0.75), CT1 (p = 0.61), and CT2 (p = 0.35).
The neuropsychological test performance characteristics of the HIV-positive participants classified into HAND categories is shown in Table 2. In this analysis, we found significant between-group differences on all neuropsychological tests, except for the FT nondominant subscore of the IHDS (p = 0.10) and the MAT (p = 0.06). Participants with HAD had lower mean total IHDS scores than the remaining participants, with means of 9.69 (SD = 1.97) and 10.67 (SD = 1.11), respectively (p < 0.00).
ANI, asymptomatic neuropsychological impairment; MND, mild neurocognitive disorder; IHDS, International HIV Dementia Scale; FT, Finger Tapping Test.
Correlations between the IHDS total and subtest scores, on the one hand, and each neuropsychological test, on the other, are shown in Table 3. We identified significant correlations between the IHDS total score and the FT-ND, HVLT, BVMT, MC, CT1, CT2, and category fluency (fruit and vegetables) z scores. The CT1 was significantly correlated with all components of the IHDS.
IHDS, International HIV Dementia Scale; FT, Finger Tapping; GP, Grooved Pegboard; HVLT, Hopking Verbal Learning Test; BVMT, Brief Visuospatial Memory Test; MAT, Mental Alternation Test; TMTA, Trail Making Test part A; CT1, Color Trials Test 1; CT2, Color Trails Test 2; WCST, Wisconsin Card-Sorting Test.
We conducted a number of receiver operating characteristic analyses to establish the ability of the IHDS to discriminate between varying degrees of HAND, including normal neuropsychological function. The receiver operating characteristic curve of the IHDS using the HAND categories of HAD together with MND versus other categories as gold standard is shown in Fig. 1. The area under the curve (AUC) was 0.64. The varying cutoff scores for the IHDS are presented in Table 4. At a cutoff score of 10 or less, the sensitivity and specificity of the IHDS was 45% and 79%, respectively. Using a cutoff of 11 or less, the sensitivity and specificity of the IHDS was 72% and 46%, respectively. The ability of the IHDS to discriminate between HAD and normal participants was similar (AUC = 0.60, with a sensitivity of 74% and specificity of 33% at a cutoff of ≤11).
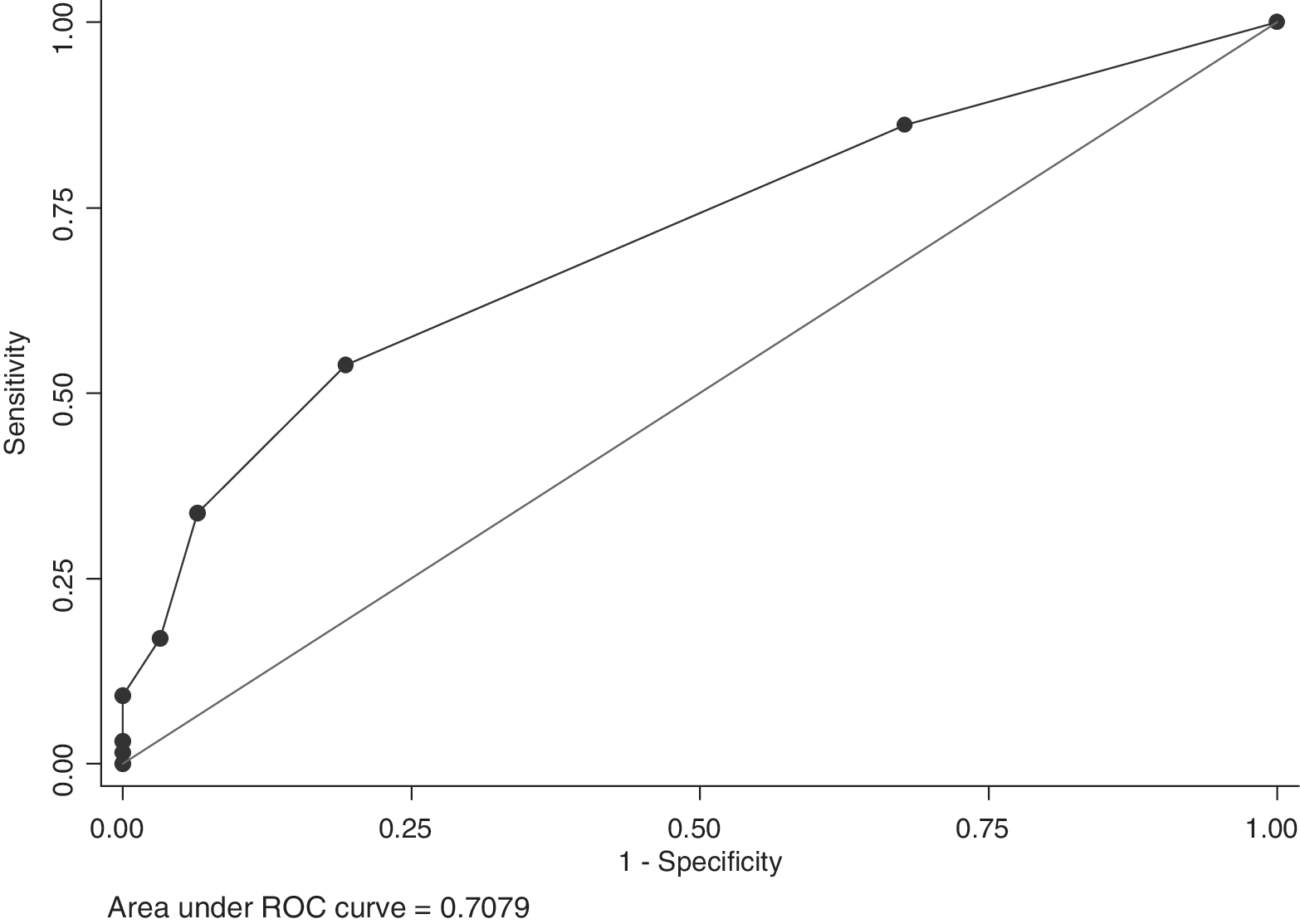
Receiver operating characteristic curve of total International HIV Dementia Scale (IHDS) compared to HIV-associated neurocognitive disorders (HAND) categories (American Academy of Neurology disorder categories versus asymptomatic groups). Standard error (SE) = 0.051; 95% confidence interval 0.607– 0.808). Using a cutoff score of 10 or less, the sensitivity of the IHDS was 81% and the specificity was 54%.
PPV, positive predictive value; NPV, negative predictive value.
Discussion
In South Africa where HIV is highly prevalent, and rates of severe HAND are in excess of 50%, access to a screening tool for cognitive impairment has both clinical and research relevance. 7 In this study we identified that the IHDS discriminates modestly when used to diagnose severe HAND (including HAD and MND). We utilized a detailed neuropsychological battery that was sensitive to differences between HIV-negative and HIV-positive controls. When we compared IHDS and neuropsychological test performance in the HIV-positive participants across categories of HAND, we observed that the battery discriminated well across different groups, and for a number of test domains. In a receiver operating curve analysis using a cutoff score of 11 or less, the IHDS was 53% sensitive and 80% specific. The IHDS correlated moderately with individual neuropsychological tests.
The ROC analysis revealed that the IHDS performed satisfactorily, although a cutoff score of 11 or less provided a better sensitivity. When we used a cutoff score of 10 or less, the sensitivity and specificity was 45% and 79%, respectively. It may be more beneficial to retain the higher sensitivity and therefore use the cutoff of 11 or less rather than 10 or less, in order not to miss cases. In the original description of the IHDS, cutoffs of 0 or less yielded sensitivities of more than 80%, with moderate specificity. 15 The performance of the grooved pegboard test nondominant has previously been reported to yield a sensitivity and specificity of 71% and 46%, respectively, using a cutoff of 1.5 standard deviation (SD) below adjusted means. Others have reported sensitivity and specificity of 77% and 65%, respectively. 18 The IHDS therefore could be useful tool, although clinicians in South Africa may need to consider using the higher cutoff score of 11.
HIV-positive individuals in this study performed worse than their HIV-negative counterparts on most tests of neuropsychological function, including the IHDS. Of note, there were no differences in performances on the hand sequence component of the IHDS, the MAT, CT1, and CT2 tests. Overall, then, our battery was sensitive to HIV-associated neuropsychological impairments. Of interest is that both groups of participants in our study performed better on CT1 and 2 than participants in Uganda. 15 This may be explained by lower levels of education in that study's participants (9.7 for controls and 8.7 years for HIV-positive participants). In addition, in the Ugandan study, no differences in motor performance were reported. These included the GPT and timed gait tests, while in our study, we did find differences in this domain. 15 One possible explanation is that regional and clade differences account for these domain-specific differences. The HIV epidemic in Uganda is known to be predominantly made up of clades A, D, and D, while in South Africa clade C is predominant. 23,24 Previous studies of participants with clade C HIV have also reported abnormalities on GP. 25
The IHDS, together with individual neuropsychological tests, discriminated well between HAND categories. This suggests that these tests are suitable in differentiating different forms of HAND. The mean total IHDS score for individuals with HAD was 9.67, compared to 10.67 for other participants. In the group analysis, the finger-tapping test of the IHDS did not discriminate well across all categories, though the performance in the HAD group was worse than the other three groups (mean of 3.19, versus 3.64, 3.72 and 3.63, respectively; p = 0.10). The finger-tapping test used in the battery, however, did discriminate well between the groups. When we compared participants with disorder (HAD and MND) with those without disorder (ANI and normal), only the IHDS total score showed a trend to significance. This suggests that an adapted brief screening tool might include other measures such as bedside tests of executive function.
The correlation between the IHDS total score and subtest scores, on the one hand, and individual neuropsychological test scores, on the other, varied from weak to moderate. We expected the total IHDS score to correlate more strongly with nondominant hand performance on the GP-nondominant test, as reported by Sacktor and colleagues. 15 However, as noted above, this difference might be explained by regional and clade-specific differences in test performance. We also expected the IHDS finger-tapping test to correlate more strongly with the similar neuropsychological test, but the results were weak. The IHDS recall test correlated moderately with the HVLT test. The weaker correlations that we found might be explained by differences in test internal construct validity and ecology being different. To date there has been little or no research describing construct validity of these neuropsychological tests in South Africa; and in isiXhosa speakers in particular.
This study had several limitations. First, our sample size was not very large. We did not believe this is a significant weakness as we were able to identify statistically significant differences between groups in terms of cognitive status. Second, while our group has taken care in translating and adapting the neuropsychological test battery to ensure its suitability for South Africans, we have not undertaken to establish construct validity. Third, we found significant differences between HIV-negative controls and HIV-positive participants with respect to age and level of education. The difference in age was not predictive of total IHDS score in either group, while the level of education did predict IHDS score in only HIV-negative participants. In the original description of the IHDS, the HIV-negative control group were also significant younger than the HIV-positive participants, but the authors did not establish whether age was an independent determinant of performance. 15
We believe this study contributes to our knowledge about HAND in southern Africa. Specifically, that neuropsychological impairment is frequent and severe in South Africa. Furthermore, the IHDS may be a useful screening tool, although efforts to understand the modest level of specificity requires further study. Individuals with HAD clearly perform worse on the IHDS, as well as on most tests included in our detailed battery as expected since performance on cognitive testing is utilized in the diagnostic classification. Nonetheless, as a brief tool, the IHDS performed satisfactorily in comparison to the detailed battery and was able to discriminate across different severities of HAND. Further research into refining the IHDS and incorporating it as a brief screening tool in to primary care is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.