
Abstract
Metabolic syndrome (MetS) is associated with development of type 2 diabetes mellitus and increased risk for cardiovascular disease. However, a few studies have assessed its prevalence and risk factors among HIV patients from developing countries. The aim of this study was to identify independent risk factors for metabolic syndrome by the criteria of the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) among HIV-infected men and women. A cross-sectional study enrolled patients, aged 18 years or older, who sought to confirm the diagnosis or sought treatment in the outpatient service of a public health care center in southern Brazil. From June 2006 to December 2008, certified research assistants conducted interviews using standardized questionnaires and anthropometric measurements. Fasting blood sample was collected, use of highly active antiretroviral therapy (HAART) was ascertained, and MetS was characterized by AHA/NHLBI criteria. In the total, 1240 of 1295 HIV-infected patients were included. MetS prevalence was 24.7% and was similar among men and women. Among men, age, education, physical activity, body mass index (BMI), and HAART use were independently associated with MetS, while among women, there were associations with age, BMI, and use of protease inhibitors. In conclusion, high prevalence of MetS was detected in HIV-infected men and women. In both genders, age and BMI were directly and independently associated with MetS. The association between the use of HAART and MetS was confirmed among men but not among women.
Introduction
H
The overall prevalence of MetS ranged from 4% to 45% among HIV/AIDS patients, depending on diagnostic criteria and characteristics of the population. 7 –10,12 In seven Latin America countries, 8.4–25.4% of patients with HIV on HAART for at least 1 month had MetS 13 according to the NCEP-ATPIII criteria. 14 However, 4.1% 8 up to 20.8% 5 of treatment-naïve HIV-infected patients had MetS, and the prevalence increased exponentially among the past (42.1%) and current (33.9%) protease inhibitors users. 7
Predictors of MetS have been rarely reported taking into account confounding factors 7 in studies conducted in developing countries 13,15 and using the updated set of criteria from American Heart Association and National Heart, Lung, and Blood Institute (AHA/NHLBI). 16 This study aimed to investigate MetS and its independent predictors among HIV-infected men and women, according to the AHA/NHLBI criteria in southern Brazil.
Methods
A cross-sectional study was conducted among HIV-infected patients, aged 18 years or older who sought health care at one of the three largest public HIV/AIDS reference centers in Porto Alegre, Southern Brazil. Pregnant women, patients with mental retardation and under the restriction of freedom were excluded. The project was approved by the Ethics Committee of the institution, and all patients signed an informed consent.
The data collection was performed at the routine visit by certified physicians and research assistants. For quality assurance purposes, a 5% random sample of the interviews was repeated. A standardized questionnaire was used to investigate demographic, socioeconomic, clinical characteristics, use of HAART, and other risk factors for MetS. Demographic (age, calculated from the birth date, self-reported skin color), socioeconomic (years at school, measured as the number of years of successfully completed formal education), and lifestyle (physical activity and smoking) characteristics were recorded. Skin color was categorized as white or non-white. For patients who have been smoking 100 or more cigarettes during their lifetime, exposure was calculated by number of packs smoked per year, 17 and categorized as 20 or more or less than 20 packs per year. Physical activity was investigated using the International Physical Activity Questionnaire, 18 and those performing 30 min or more of moderate to vigorous physical activity at least 5 days per week (150 min/week) were considered active 19 ; those who perform less than 150 min/week were considered physically inactive. Time of HIV infection was calculated tracking the time from the diagnosis of HIV infection based on patient information and confirmed by laboratory test or medical record. HAART was determined by use of three or more antiretroviral drugs in the past 12 months, recorded in the pharmacy dispenser or medical record. The use of protease inhibitors and non-nucleoside reverse transcriptase inhibitor was accessed for the past 12 months.
Laboratory tests were performed with 12
Weight (kg) and height (m) were measured with patients wearing light clothes and bare feet, using anthropometric scale (Filizola® adult model 31, Filizola Industries S.A., São Paulo/SP, Brazil) with 100 g precision and anthropometric ruler with 0.5 cm. Anthropometry was performed in duplicate, and the average of two measurements was adopted in the analysis. Body mass index (BMI) was calculated by dividing weight (kg)/squared height (m), and categorized as less than 25.0, 25–29.9 (overweight), or≥30.0 kg/m2 (obesity). Waist circumference was determined with a flexible inelastic tape measure placed in the midway between iliac crest and lower costal margin 2 ; hip circumference was measured in the greatest gluteal protuberance, at the level of great trochanter. Central obesity was determined by waist circumference 90/80 cm or greater for men and women, respectively.
The sample size calculation was based on that at least 15% of patients under no HAART (approximately the prevalence on the Italian general population) and 22% of patients on HAART would present MetS, 8 being necessary to study at least 510 patients in each group, with 80% of power and 95% confidence interval.
ata were presented as mean and standard deviation (±SD) or frequencies and were compared by analysis of variance or Pearson's χ2 test, using the Statistical Package for Social Sciences (SPSS, Chicago, IL; version 16.0). The analysis between risk factors and MetS were conducted separately for men and women, using the modified Poisson regression. The results were expressed as risk ratios (RR) and 95% confidence intervals (95% CI), nonadjusted and controlling for confounding factors. Those were selected among characteristics associated with MetS, in the bivariate analysis, using a p value≤0.2, as the cutoff. Determinants of antiretroviral therapy—CD4 and viral load—were not included in the full model as confounding factors, due to collinearity with HAART use, but their effect was determined in separate models with control for all assigned confounding factors. The trend toward significance was defined for 0.05<p value<0.1.
Results
There were 1240 HIV-infected patients included of 1295 potentially eligible; 15 refused and 40 were excluded due to being in restraint of freedom, under the influence of alcohol, being pregnant, or having no time to perform the evaluation. Participants were, on average, 38.6±10.1 years old and approximately half of them were men. The overall prevalence of MetS was 24.4% (95% CI: 19.8–29.5) according to the AHA/NHLBI and 17.2% (95% CI: 12.1–22.3) by NCEP-ATPIII, and among patients aged 60 years or older, these rates increased to 62.5 and 45%, respectively.
Table 1 shows characteristics of HIV-infected men and women and, as can be seen, men were more likely than women to be older, self-reported as white race, and having higher educational attainment. They also had increased tobacco smoking overload and time since the HIV infection diagnosis have been established. On the other hand, among women the average of BMI, central obesity and physical activity prevalence were higher. However, prevalence rate of MetS did not vary between men (24.2%) and women (24.7%).
AHA/NHLBI, American Heart Association/National Heart, Lung, and Blood Institute; HDL, high-density lipoprotein; HAART, highly active antiretroviral therapy; SD, standard deviation.
Predictors of MetS are presented in Table 2. There were increasing prevalence of MetS with age, BMI, use of HAART, and undetectable viral load for men and women. However, white race, physical inactivity, high CD4 count, and protease inhibitor use were risk factors among men, but educational attainment was associated with MetS only for women. Antiretroviral classes of protease inhibitor and non-nucleoside reverse transcriptase inhibitor showed a borderline association with MetS for men and women.
American Heart Association/National Heart, Lung, and Blood Institute criteria.
Mets, metabolic syndrome; HAART, highly active antiretroviral therapy.
Table 3 shows that several risk factors were independently associated with MetS among men, such as aging, low education attainment, physical inactivity, BMI≥25 kg/m2, use of HAART, and non-nucleoside reverse transcriptase inhibitor. The control for confounding factors partially reduced the risk for MetS due to age and physical inactivity, but it increased due to overweight and obesity, and use of non-nucleoside reverse transcriptase inhibitor. White males had higher prevalence of MetS than non-white ones in the bivariate analysis, but the association became non-significant after the control for age and other confounding factors.
American Heart Association/National Heart, Lung, and Blood Institutecriteria.
Non adjusted RR.
RR adjusted for age, race, years at school, smoking, physical activity, years since diagnosis of HIV infection, BMI, and use of HAART.
RR adjusted for the all confounding factors, except HAART.
RR, risk ratio; CI, confidence interval; BMI, body mass index; HAART, highly active antiretroviral therapy.
Table 4 shows that among women, the risk of MetS increased with aging and BMI, and the associations remained significant even after the control for several confounding factors. However, educational attainment lost its explicative power after the adjustment for confounding factors. The use of HAART had attenuated the magnitude of the risk for MetS and persisted as trend toward the association, while protease inhibitor turned over significant. The lack of association between race and MetS was confirmed for women.
American Heart Association/National Heart, Lung, and Blood Institute criteria.
Unadjusted RR.
RR adjusted for age, race, years at school, smoking, physical activity, years since diagnosis of HIV infection, BMI, and use of HAART.
RR adjusted for the all confounding factors, except HAART.
RR, risk ratio; CI, confidence interval; HAART, highly active antiretroviral therapy.
Figure 1 explores the association of viral load and CD4 count with MetS according to the use of HAART in separate analyses conducted for men and women. Risk ratios and 95% CI, obtained from modeling with full adjustment for confounding factors, confirmed the independent associations of viral load and CD4 count with MetS for males on HAART. The analysis of viral load with MetS conducted in women produced an independent association only for those on HAART use. Nevertheless, HIV infected HAART-naïve women with low CD4 had, approximately, double the risk of MetS in comparison with those with higher CD4 count.
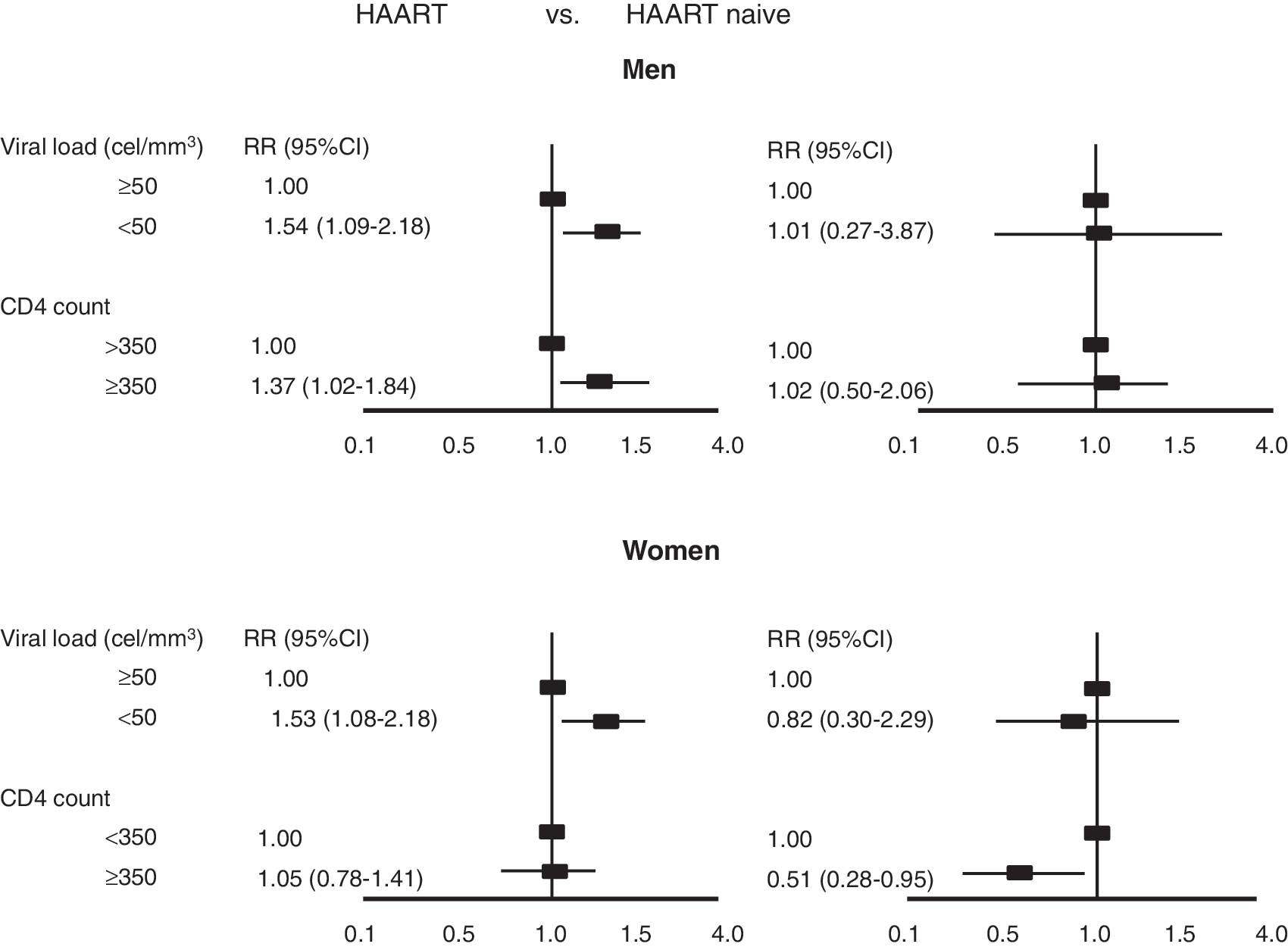
Viral load and CD4 count associated with metabolic syndrome according to highly active antiretroviral therapy (HAART) and by gender.
Discussion
In this large sample of HIV-infected patients, we were able to confirm that age and BMI were robust and independent predictors of MetS, presenting a dose-response relationship for both men and women. The independent association of MetS with HAART and non-nucleoside reverse transcriptase inhibitor use could be verified for men. Nevertheless, among women, control for confounding factors attenuated the magnitude of HAART use or even allowed the emergence of a positive and independent risk factor: protease inhibitors.
The associations of MetS with aging, 7,8,15,22 –24 BMI, 7,9,15,22 and exposure to antiretroviral drugs 7,9,10 have been reported for HIV-infected patients. In this article, we went further evaluating risk factors for MetS, separate for men and women, and using the new definition recommended for the AHA/NHLBI. In addition, we also explored the role of viral load and CD4 on MetS taking into account HAART use.
The prevalence of MetS detected in this study was similar 9,21 or higher 7,8,12 than that described in others studies, possibly due to the less restrictive criteria used to define MetS, 16 the ratio of men to women, and the increased number of patients on HAART. A previous study conducted in HIV-infected patients aged 70–79 years old detected a 38% prevalence of MetS–NCEP III criteria. 22 In this study we do not have enough HIV patients with such age range, but among those aged 60 years or older, 45% had MetS by the same criteria. Although the use of HAART increased MetS prevalence, the effect was not uniform and varies across pharmacological classes of antiretroviral. For instance, HAART was a clear risk factor for MetS among men, but had only a trend toward association in women. The analysis of classes of antiretroviral was carried out only for protease inhibitor and non-nucleoside reverse transcriptase inhibitor, which have been used by most patients on treatment in the last 12 months. Even so, the independent effect of specific antiretroviral drugs was not confirmed in a Danish study. 10
Some risk factors such as white race do not have a specific mechanistic role, but in Brazil it is likely to act as a marker of higher socioeconomic status. So, among men, white race was associated with higher prevalence of MetS in the nonadjusted analysis, but after the control for age and years at school, it became nonsignificant. Among women there was no association with race even in the bivariate analysis.
This study showed that the association of MetS with viral load and CD4 count was modified by the use of HAART. A previous study identified that persistent viremia was a predictor of MetS. 21 However, Squillace et al. 23 conducted their analysis on a sample of HIV-infected patients on stable antiretroviral therapy regimens. Therefore, they could not detect this effect modifier. Another study conducted on a sample of HIV-infected patients, 76% being on HAART, did not address this association, but identified that undetectable viral load was a protective factor for low HDL-cholesterol, particularly among those on HAART. 25
Obesity is considered a major risk factor for the increased prevalence of MetS by the NCEP-ATPIII 14 and IDF 2 criteria. In this study, this association was confirmed for men and women, and it was independent of other risk factors. However, in this study men and women had higher prevalence of obesity than previously reported. 26,27 In a study conducted in six U.S. cities, among HIV-positive and HIV-negative women, it was detected similar prevalence of obesity by infection status. 27 In contrast, markers of advanced HIV-infection (AIDS diagnosis, elevated viral load, low CD4 count), and the report of antiretroviral therapy were independently associated with lower BMI. 27 Even that insulin resistance and central body fat 28 are in the pathway of metabolic syndrome, the former has been independently associated with all criteria of MetS.
Some limitations should be considered when interpreting the results of this study. A cross-sectional study does not allow establishing temporality between exposure and outcome, and physical activity may, for example, result rather than being associated with the risk of developing it. Thus, reverse causality might potentially explain some associations, but it is unlikely for age and other exposures of interest. The strength of this study was the large sample size, have been carefully conducted, in a developing country, and have shown that men and women have high prevalence of MetS, even that different predictors could be responsible. Finally, the lack of one underlying cause for the abnormalities linking the components of metabolic syndrome has been argued, and it reinforces the concept that MetS does not represent a syndrome. 11 In addition, metabolic syndrome is not fully understood for HIV-infected patients. However, the anticipation of early diagnosis for its components should be part of the good clinical practices. Consequently, doing so it might contribute to slow or even reduce its impact on the development of cardiovascular disease.
Footnotes
Acknowledgments
This study was supported by grants and fellowships from the Ministry of Health/Secretariat of Health Surveillance/National STD and AIDS Programme (MOH/SHS/NAP), National Counsel of Technological and Scientific Development (CNPq), the National Institute for Science and Technology for Health Technology Assessment (IATS/CNPq) in Brazil, Fundo de Apoio a Pesquisa (FIPE) do Hospital de Clínicas de Porto Alegre.
The authors thank the personnel staff, physicians, and patients of the Hospital Sanatório Partenon, Therapeutic Assistance Service, for their collaboration to make this study possible.
P.A., A.B, and M.L.I. conducted the research and analyzed the data. P.A., F.H.W., and N.B. wrote the manuscript. S.F. analyzed the data, reviewed/edited the manuscript and contributed to the discussion. A.B. contributed to the discussion.
Author Disclosure Statement
No competing financial interests exist.