
Abstract
Initial validation of the HIV/AIDS Provider Stigma Inventory (HAPSI), piloted on a sample of 174 nursing students, supported the psychometric qualities of a suite of measures capturing tendencies to stigmatize and discriminate against people living with HIV/AIDS (PLHA). Derived from social psychology and mindfulness theories, separate scales addressing awareness, acceptance, and action were designed to include notions of labeling, stereotyping, outgrouping, and discriminating. These were enhanced to capture differences associated with personal characteristics of PLHA that trigger secondary stigma (e.g., sexual orientation, injection drug use, multiple sex partners) and fears regarding instrumental and symbolic stigma. Reliabilities were strong (coefficients α for 16 of 19 resulting measures ranged from 0.80 to 0.98) and confirmatory factor analyses indicated good model fit for two multidimensional (Awareness and Acceptance) and one unidimensional (Action) measure. Evidence of convergent construct validity supported accuracy of primary constructs. Implications for training and professional socialization in health care are discussed.
Introduction
S
This article details the conceptual development and initial validation of a suite of measures known collectively as the HIV/AIDS Provider Stigma Inventory (HAPSI). The HAPSI blends theoretical principles of social psychology and mindfulness used in our previous work conceptualizing the Awareness, Acceptance, and Action Model (AAAM) and piloting a group-level stigma reduction intervention for health care and social service providers. 1 The HAPSI was designed to assist providers across disciplines in gaining insights into their attitudes about and interactions with PLHA in order to identify the presence of stigma related behaviors and optimize clinical outcomes for their patients or clients. Following presentation of the instrument's initial validation with a sample of baccalaureate nursing students, we discuss ways in which the HAPSI can be used in a variety of health care and social service settings.
The earliest example of research characterizing disease-related stigma was completed by Goffman who identified the existence of sources of stigma such as physical deformity, character-related blemishes and tribal affiliations. 2 Goffman's early works provided the basis for many of the current conceptualizations of HIV-related stigma, which differentiate categories of stigma as instrumental (fear of physical contagion), symbolic (values- or morality-based judgment), felt, perceived, or internalized (experiences of prejudice and discrimination), courtesy (felt by providers or families of PLHA), and enacted (discriminatory actions). 3 –5
Researchers have focused on attitudes about PLHA among the general public; experiences among PLHA with families, communities, and health care providers; and concerns about interactions with PLHA among health care providers, including nurses. Fear of occupational exposure to HIV has been a significant source of stress and an antecedent of stigma among providers. 6 –11 Courtesy stigma, or the prejudice and discrimination directed at caregivers for their work associated with PLHA, has also been a concern. 12
Prejudice toward PLHA among health care workers and lay people was described by researchers in the 1980s and 1990s, and later studies confirmed that individuals at risk for HIV or living with the disease delay or fail to access care to avoid judgment and rejection by providers, families, and the general public. 3,13 –15 A meta-analysis of 24 North American studies of stigma among PLHA revealed significant medium-sized correlations between stigma and low social support, poor physical health, poor mental health, age, and income. 16 In summary, the literature indicates the importance of recognizing the effects of stigma as a key influence on individuals' health status. As described below, becoming aware of and accepting the consequences of one's own potential for stigmatizing clientele in health care or social service settings is crucial to improving care for PLHA.
Early research in the nursing domain indicated important correlations between HIV/AIDS and secondary individual variables. 17 Factors considered to be personal choices (e.g., drug use, multiple sexual partnerships, same-sex relationships) by providers resulted in negative views of PLHA. Subsequent studies established the effect of individual reflections about PLHA's personal characteristics and behaviors (e.g., sexual orientation, drug use) on nurses' attitudes toward them. 18,19 Although there were correlations between HIV/AIDS and existing stigmatized statuses (e.g., gay and other men who have sex with men [MSM] and intravenous drug users [IDU]), nurses generally possessed empathetic and positive reflections regarding PLHA. 20 –22
Research has also indicated, however, substantial prejudice toward PLHA and fear of providing direct care to known HIV infected persons by some nurses. 23,24 Studies have continued to indicate evidence of stigma in health care settings around the world. 25 –28 These studies have documented instances in which providers insult patients; refuse, delay, or neglect their care; violate confidentiality; and overprotect themselves from physical contact. Research conducted in various countries of student nurses' attitudes about PLHA and their concerns about working with them 19,29 –31 points to the importance of enhancing education about universal precautions and actual patterns of occupationally related infection of health care workers, including dentists, 32 to reduce fears about transmission. In summary, although the literature indicates some level of empathy for PLHA, symbolic bias associated with sexual orientation, promiscuity, and drug use, as well as the persistence of concerns about occupational exposure, signify that substantial challenges remain in the effort to decrease stigmatizing behaviors among nursing professionals.
Although it has been well established that PLHA anticipate and experience stigma within health care, research on the measurement of provider stigma has been limited, largely due to the absence of systematically collected data on the precise structural nature of HIV-related discrimination in health care settings. 33 Theorizing, exploring, and documenting the determinants of stigma in health care settings is essential for the creation of antistigma interventions. Measuring stigma is essential to quantify the presence and progression of stigma and discrimination in health care settings, compare stigma cross-culturally, determine social trends in stigma-related barriers to provision of lifesaving treatment options, and evaluate antistigma campaigns. 15 A variety of attempts have been made to develop such measures either alone, or as a component of an intervention. 34 –39
AIDS stigma measures and scales have been used to assess the general public's attitudes toward PLHA 40 as well as the anticipation of and lived experiences with stigma by PLHA, including psychological and social support factors as well as barriers to health care. 35,41,42 Some scales have been used to assess health care providers' stigmatizing attitudes. 43 There are also examples of scales designed to capture nurses' fears about HIV and their attitudes about serving PLHA. An early nursing-specific short scale was developed to assess the willingness to care for and attitudes toward PLHA, MSM, and IDU, 17 and the Nursing Willingness Questionnaire measured nurses' willingness to care for a hypothetical male adult patient with AIDS. 44 More recently, a 21-item stigma index was developed with health care providers in India that included questions about attitudes toward PLHA, including personal contact and judgment, and attitudes toward health care practices with PLHA, including testing, informed consent, disclosure, infection control, and patient rights. 45 Also, in a rigorous set of validation studies that took place in 5 countries in Africa, a 19-item scale was developed to measure nurses' stigmatizing tendencies and experiences of courtesy stigma. 38
In summary, a variety of tools have been developed to measure stigma among health care providers. As detailed below, the HAPSI adds to this menu of instruments, and deepens the focus on instrumental and symbolic constructs by assisting providers in assessing their awareness of negative attitudes associated with subgroups of PLHA, accepting the potential consequences of carrying such views into client or patient interactions, and acting intentionally to prevent their prejudice from escalating to enacted discrimination.
The HAPSI is grounded dually in Link and Phelan's 46 widely used social psychological stigma framework as well as our original Awareness, Acceptance, and Action Model (AAAM), which is based in principles of mindfulness. 1 Link and Phelan proposed that humans attach negative attributes to everyday differences among people such as gender, race, and class. In turn, these labels become stereotypes that are used as evidence to create and reinforce outgroups as a way to “separate us from them,” and ultimately, to enact status loss and discrimination in order to maintain physical and social distance (instrumental and symbolic stigma respectively). Supporting Link and Phelan's proposition that these dynamics are played out in power situations (and as asserted by Parker and Aggleton 47 that power is integral to stigma), we believe nurses and other providers have inherent power over their patients due to their role as gatekeepers to treatment. Societies worldwide charge medical professionals and healers to reinforce social and cultural mores, which, when taken to unchecked levels by providers themselves, may result in both unintended and purposeful manifestations of AIDS stigma. Understanding one's potential to violate ethical principles of justice, beneficence and nonmaleficence is critical, especially when providers are not fully aware it is happening. A mindfulness approach can be helpful in prompting awareness of stigma.
Mindfulness originated from the ancient philosophical traditions of Asia. It has been used with behaviors and illnesses thought to be responsive to mind–body health interventions, as a way to promote thoughtful responses rather than automatic reactions, through the cultivation of meaning derived from reflections about troubling situations. In this article, we provide only a brief overview of the AAAM, which was developed from tenets of mindfulness, to set the stage for how we conceptualized the constructs for our suite of measures. 1 At the level of Awareness, we believe providers should look deeply for internal thoughts and feelings and listen to patients presenting for services, who are at risk for HIV or who have an existing diagnosis. Through active listening and reflection, providers may identify, for example, their fears about occupational exposure, concerns about social association, and prejudice based on associated statuses and histories (e.g., sexual orientation, substance abuse) along with presumptions about behavior that may have led to the patient's infection (e.g., having multiple sex partners, needle sharing). The second level, Acceptance, invites providers to acknowledge the potential consequences of their stigmatizing attitudes and behaviors, not only as they affect the well being of their patients, but as they reflect on themselves as humans and as health or social service professionals. Finally, Action calls upon providers to act intentionally and with compassion to override their potential for stigmatizing their patients through unchecked reactivity. Compassionate action can be realized through positive interactions with patients as well as through the modeling of positive behaviors in the presence of colleagues and lay people alike.
Methods
Scale conceptualization and development
Psychometric studies of novel instruments are needed to capture multiple domains of AIDS stigma, particularly ones that focus on enacted stigma (i.e., discrimination) and compound or layered stigma that integrates concerns about AIDS stigma and preexisting social prejudice about marginalized groups. 48 Thus, we integrated the well-respected social psychological stigma framework of Link and Phelan 46 and our own mindfulness model. The HAPSI “nests” Link and Phelan's 46 four components of labeling, stereotyping, outgrouping, and discriminating within our mindfulness model of AAAM. 1
In our prior work toward developing mindfulness exercises for antistigma workshops, we anchored the social psychological processes of labeling, stereotyping, outgrouping and discriminating within the progression of first becoming self-aware of one's stigmatizing tendencies and then accepting the implications of those tendencies on a path to intentional action or unintentional reactivity. This conceptualization provided an opportunity for respondents to first come to awareness of how their psychological processes of thoughts, feelings, and behaviors are reflective of sociological processes related to stigma (Awareness) and then how these same psychological processes may affect their interactions with patients (Acceptance). This integration aims to reinforce the inherent logic of a recognized social psychological stigma conceptualization by inserting it into a framework designed to guide providers through a sequence of reflections promoting more supportive, less stigmatizing engagement. Thus, as a way both to guide workshop participants in applying these concepts to their lived experiences with patients and to measure attitudes and their change, we developed the HAPSI scales to reflect this blending of Link and Phelan's framework with our AAAM approach.
To elucidate each of Link and Phelan's four components—labeling, stereotyping, outgrouping, and discriminating—we drew from our earlier work described above in developing a stigma questionnaire for delivering antistigma workshops in the United States and the eastern Caribbean as well as in-depth qualitative research. 1,25,49 As part of the AAAM workshop approach, we asked participants to gauge their feelings of warmth toward populations traditionally associated with HIV/AIDS (MSM, IDU and other drug users, sex workers). For that questionnaire, we drew from Herek's feeling thermometer and other questions about stigma. 50 This is in keeping with recommendations that subgroup membership, physical proximity to PLHA, and personal characteristics (stereotypes about PLHA) may be sources of secondary stigma layered over and above that associated with HIV status. 48
In addition to confirming lesser degrees of warmth expressed for subaltern groups, our analyses revealed the importance of considering warmth, comfort, distancing, condemnation, myths about transmission, and ability to effectively counsel PLHA among health and social care providers. 49 In addition, to construct an extensive item pool for the HAPSI, we drew upon our qualitative studies of provider stigma in the Eastern Caribbean wherein we explored the fit of the four components of the Link and Phelan framework. 25
As a result, free-standing but related measures were proposed for Awareness, Acceptance, and Action. Figure 1 illustrates the structure of the three scales and provides construct definitions. Table 1 includes sample items. All HAPSI items were designed to be assessed using a 7-point Likert-type response scale where 1=completely disagree and 7=completely agree. The first scale, Awareness, was defined as “ ‘looking deeply,’ noticing the full range of our experiences when encountering or thinking of PLHA.” Within Awareness, subscales were proposed for each of Link and Phelan's constructs of labeling, stereotyping, outgrouping, and discriminating. Of these, Label and Discriminate were further deconstructed into subscales reflecting whether stigmatizing tendencies were colored by assumptions about the patient's status (Associate), and by whether the provider was concerned about instrumental (Transmit) or symbolic (Censure) consequences of contact as determined important in prior work 49 and recommendations made in published reviews of existing stigma theory. 48 Stereotype was deconstructed to address three primary personal characteristics often associated with HIV/AIDS—male homosexuality, injecting drug use, and having multiple sex partners.
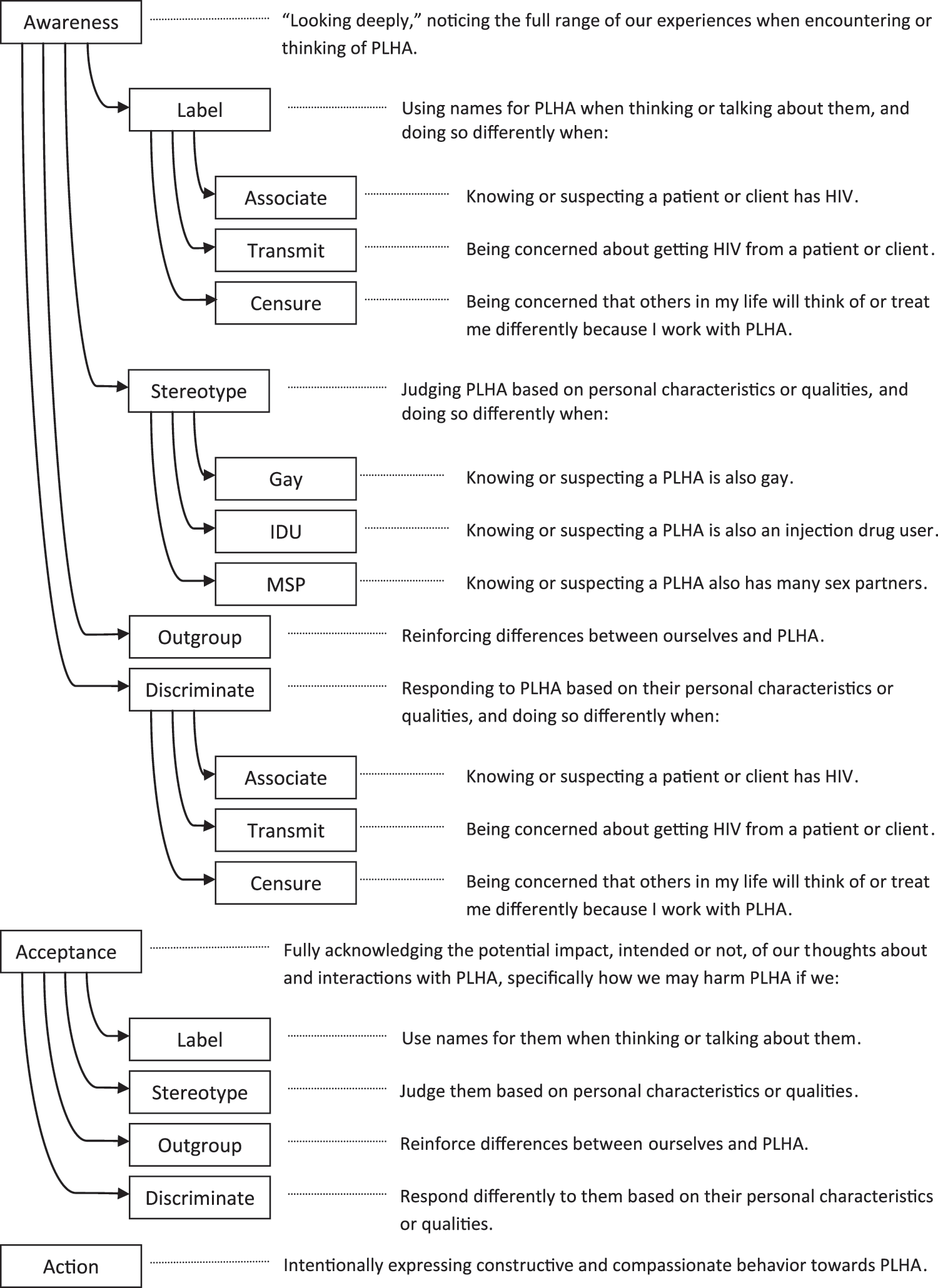
HIV/AIDS Provider Stigma Inventory (HAPSI) scale and subscale structure with construct definitions.
HAPSI, HIV/AIDS Provider Stigma Inventory; PLHA, People living with HIV/AIDS; IDU, injection drug use; MSP, many sex partners.
Following the principles of mindfulness, Acceptance, the second scale, shifts the emphasis to consequences of one's own thoughts and interactions. In specific, we defined Acceptance as “fully acknowledging the potential impact, intended or not, of our thoughts about and interactions with PLHA.” Parallel to the proposed Awareness scale, we likewise deconstructed Acceptance into four social psychological subscales and subgroup personal characteristics.
The third scale, Action, reflects the final mindfulness principle of AAAM and focuses on proactive, constructive, and compassionate behavioral responses rather than unintentional reactions. We defined Action as “intentionally expressing constructive and compassionate behavior toward PLHA.” Items proposed for Action included a variety of ideas gleaned from participants in our AAAM workshops, as well as our own collective experiences working as providers and consultants in HIV/AIDS care and prevention. For example, some social service and health care providers suggested they intentionally strive to stop negative talk about PLHA or encourage colleagues and supervisors to abide by confidentiality.
Content validation
Following development of item pools reflecting the structure described above, 15 expert panelists were invited to critique the fit between proposed items and their intended construct definitions. Ten panelists responded, including national, state, and regional experts in social service and health care delivery for PLHA. Each rated item/construct match on a scale from 1=not at all to 5=very well, and most provided detailed comments on the wording and the intent of proposed items. Ratings were based on broad construct definitions, with language variations designed to differentiate personal characteristics and fears linked to instrumental or symbolic stigma. When inspecting individual items, our criterion for retention was a mean rating across experts of 3.5 or more. The goal was to identify general endorsement of items at this preliminary stage, reducing the number of items used in the full sample validation and the resulting more rigorous critique. Based on panelists' feedback, the initial total pool of 192 items was reduced to 109. A table of mean item ratings for proposed items is available from the first author.
Data collection instrument
In addition to the reduced item pool, questions were included to capture respondent demographics and to provide a set of variables for testing evidence of construct validity. Given the novelty of the proposed constructs and the length of the data collection instrument, considerations regarding respondent burden led to the inclusion of one standardized scale and a set of single-item indicators for use in validation hypotheses. The standardized scale was the AIDS Attitude Scale (AAS), which can be deconstructed into subscales reflecting tendencies to avoid or empathize with PLHA. 39 Previous studies reported mean alpha coefficients on nursing samples of 0.89 for avoidance and 0.87 for empathy. Examples of single-item indicators include “I am more likely to think or feel negatively about PLHA who have many sex partners” (Awareness) and “If I treat my patients or clients differently because of their personal characteristics or qualities, my interactions with them may be less helpful” (Acceptance). Further details on these measures and the single-item indicators are provided with the results, below.
Sampling and data management
The initial testing of the HAPSI was accomplished with a purposive sample of nursing students attending a large baccalaureate program in the southeastern United States. This initial sampling with nursing students would provide pilot data allowing examination of the proposed HAPSI constructs and structure, and, if successful, set the stage for a second wave of validation on a more experienced clinical sample.
The university's Institutional Review Board (IRB) approved the study. Undergraduate third-year baccalaureate nursing students were invited to participate in the study. The prospective participants had received clinical and didactic training regarding the biological and social care related premises of HIV/AIDS treatment endeavors. At this level of their training, all of the prospective subjects had worked in a hospital offering direct care to patients with a variety of disorders. Per IRB approval, students were provided a cover sheet outlining the purpose of the study and their rights. Rather than signing a consent form, students were advised that completing the questionnaire constituted voluntary agreement to participate. Although recommendations for desirable sample size for confirmatory factor analyses (CFA) vary widely, 51 we targeted 200 respondents for this pilot validation. Ultimately, 184 responses were received, and of these, 10 were discarded as unusable due to extreme outliers or excessive patterns of missing data.
Inspection of the remaining 174 cases revealed that responses were essentially normally distributed with few instances of substantially missing data for individual item responses for the 109 proposed items. Twenty-six items had missingness more than 2%, and none exceeded 2.9%. Examination of missingness was conducted with SPSS Missing Values 17.0, and Little's MCAR test revealed that data were missing completely at random (χ2=2222.098, df=2155, p=0.153). To maximize case retention for subsequent analyses, missing values for proposed HAPSI items were replaced with the estimation maximization (EM) method. Frequency distributions identified 12 items with extreme skewness (>3) or kurtosis (>10) indices. 52 These were removed from the final analyses, which were conducted with LISREL 8.8 (Scientific Software International, Inc., Lincolnwood, IL) and SPSS 17 (SPSS Inc., Chicago, IL).
Results
Demographics
As shown in Table 2, nursing student respondents were primarily female and young. Approximately 75% were white, with smaller percentages divided among African American, Hispanic/Latino(a), or another race. Few (24%) were currently working, and of those describing their motivations to work, few (n=5) specified a desire to help PLHA. Only 15 had worked in HIV/AIDS care, and their mean years of service was slightly less than 1. Relatively few reported personal family, friend, or caregiving associations with PLHA.
SD, standard deviation; PLHA, people living with HIV/AIDS.
Item redundancy
Bivariate correlations were computed among individual item responses, and a conservative threshold (r≥0.80) was used to assess excessive redundancy in item content. Twenty-six such cases were found (with r ranging from 0.80 to 0.89), and after careful content inspection and consideration of the reliability analyses reported below, 17 items were flagged for removal from the final pool.
Reliability
Estimates of internal consistency were computed as Cronbach α coefficients. Inspection of α-if-item-deleted statistics in relation to initial coefficients for each proposed HAPSI construct identified items that, if removed, would enhance the overall consistency of a scale. This contributed to the flagging of 11 items for removal from the final pool. Taken together, analyses of response distribution, redundancy, and alpha-if-item-deleted (some of which led to flagging an item more than once) resulted in an 81-item instrument. Table 3 summarizes the resulting scale and subscale reliabilities and reports the number of items retained for each global HAPSI scale. Because Cronbach α tends to underestimate reliability for multidimensional scales, 51 stratified alpha coefficients were computed for each HAPSI component containing an underlying subscale structure.
Stratified α.
SD, standard deviation; SEM, standard error of the mean.
Only two reliability coefficients (Outgroup, α=0.69; Discriminate/Transmit, α=0.70) might be classified as “minimally acceptable. 53(p95) One (Discriminate/Censure; α=0.76) is “respectable.” The remaining are “very good”; five report reliability coefficients ranging from 0.80 to 0.89, and 11 range from 0.90 to 0.98. Standard errors of measurement (SEM) were computed to estimate the range of true scores around an observed score. One standard for such estimates proposes that they should be less than or equal to 5% of the possible scale score range. 54 For HAPSI items, in which responses range from 1 to 7, desirable SEMs would be 0.3 or less. Inspection of Table 3 reveals that six HAPSI components met this standard.
Factor structure
Confirmatory factor analyses were conducted to examine the hypothesized multidimensional structures of the Awareness and Acceptance scales, and the unidimensional structure of the Action scale. Target criteria were χ2/df ratios <2 or 3, Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) >0.90, root mean square error of approximation (RMSEA) <0.08, and standardized root mean square residual (SRMR) <0.10. 52 As reported in Table 4, initial models for Awareness and Acceptance met these standards with the exception of RMSEA (0.084 and 0.081, respectively). Results for Action identified problems with χ2/df (ratio=5.79) and RMSEA (0.18).
Permitting 9 error covariances.
Permitting 6 error covariances.
Permitting 38 error covariances.
CFI, Comparative Fit Index; TLI, Tucker-Lewis Index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual.
Inspection of modification indices allowing for correlated error variances consistent with proposed scale content led to respecified models for each scale. Error variances were allowed to correlate only when they were associated with significant changes in model fit and were not incompatible with the theoretical composition of proposed factors (i.e., when covariances were within a targeted item pool rather than crossing from one to another). 55,56 Resulting coefficients demonstrated improved model fit in each case. Finally, in recognition of their multilayered structures, second-order factor analyses were conducted for Awareness and Acceptance. Resulting indices indicated acceptable model fit in both cases.
Convergent construct validity evidence
To examine whether HAPSI scales measured what they were intended to measure, bivariate correlations were computed to test hypothesized relationships among HAPSI scores and responses to standardized scale scores and single-item indicators. First, performance of the AIDS Attitude Scale (AAS) 43 subscales on avoidance (AASav) and empathy (AASem) in the present sample were examined through computation of coefficient alpha. Results (AASav α=0.83, AASem α=0.89) were similar to those reported in previous research and indicated that the measures were appropriate for use in the present study.
We hypothesized that the AASav scores, indicating tendencies to avoid association with PLHA, would correlate positively with higher scores on Awareness HAPSI scales reflecting greater tendencies to stigmatize PLHA. This was true in each case (for the Awareness global score [r=0.66], and its subscales Label [r=0.58], Stereotype [r=0.59], Outgroup [r=0.55], and Discriminate [r=0.58]). Effect sizes estimating the magnitude of these relationships were computed as r 2 statistics, and ranged from 0.30 for the association with Outgroup to 0.44 with global Awareness. Likewise, we hypothesized that the AASem scores, indicating tendencies to empathize with PLHA, would be negatively correlated with HAPSI Awareness scale scores. Resulting correlations were statistically significant for global Awareness (r=−0.15) and subscales Outgroup (r=−0.16) and Discriminate (r=−0.15). Associated effect sizes were trivial (ranging from 0.02 to 0.03).
We also hypothesized that Label subscale scores Associate, Transmit, and Censure would be positively correlated with single-item indicators characterizing PLHA as gay, IDU, or having many sex partners (MSP). Associated prompts read “I am more likely to think or feel negatively about PLHA who are gay (or “use injection drugs,” or “have many sex partners”). All correlations were statistically significant, with effect sizes ranging from 0.14 to 0.29. Likewise, we hypothesized that Stereotype subscales Gay, IDU, and MSP, and Discriminate subscales Transmit and Censure would be positively correlated with single-item indicators expressing concerns about instrumental or symbolic stigma. Associated prompts read “I am more likely to think or feel these ways if I fear I may catch the virus from PLHA, or if I fear that others in my life will treat me differently for working with PLHA who are also gay, injection drug users, or have many sex partners.” Again, all correlations were statistically significant, with effect sizes ranging from 0.19 to 0.44.
Similar hypotheses were tested for global and subscale Acceptance scores. All correlations were statistically significant. Effect sizes were generally small (≤0.06), although more substantial for Label (r 2=0.13). The unidimensional Action score, representing more compassionate actions in relation to PLHA, was hypothesized to correlate positively with AASem. The result was statistically significant with a more substantial effect size (r 2=0.22). Complete results of analyses of convergent construct validity evidence for each of the three scales are available from the first author.
Discussion
Overall, the HAPSI scales achieved strong psychometrics. Content validity was generally supported by expert panelists, and psychometric coefficients revealed strong evidence of reliability and confirmation of hypothesized factor structure. Initial evidence for construct validity supported claims that the scales measure what they were intended to measure. Although the Awareness Outgroup subscale was marginal, its performance is adequate for cautious use, and warrants further investigation.
We contend that the evidence of encouraging psychometric qualities in this initial validation of the HAPSI is based on careful adherence to scale development methodology, dual integration of a solid and well-regarded theoretical framework for understanding stigma 46 and self-reflection (i.e., mindfulness principles), the inclusion of content gleaned from the collective experience of the authors in delivering stigma workshops and in direct service provision and as tailored by an expert panel. The result is a suite of measures that can be used to differentiate multiple manifestations of stigma, including instrumental, symbolic, courtesy, and enacted. Specifically, the scales tap concerns about occupational exposure, judgment based on stereotypes about PLHA that are rooted in secondary stigmas about having multiple sex partners, drug use and homosexuality, as well as concerns about being judged by families and others for caring for PLHA. In addition, our conceptualization and psychometric achievement of two separate scales for Awareness and Acceptance is useful for discerning not only nurses' self-perceived negative attitudes and actions directed at PLHA, but also their self-assessment of the consequences of their prejudice and discrimination. A more unique contribution is the creation of the Action scale to measure proactive and compassionate care. In keeping with the AAAM, we can better understand the degree to which individuals are willing to engage in helpful behaviors to decrease stigma in health care provision.
All scales were scored by computing the mean of included items. Higher scores indicate more of the tendency or quality assessed. For Awareness and Acceptance, such scores indicate greater stigma or discrimination; for Action, such scores indicate more compassionate engagement with PLHA. Although the HAPSI will be used as an outcome measurement for our provider stigma intervention, it should also be useful in early professional training. The HAPSI could be used by researchers or instructors to increase the understanding of students and novice professionals regarding the connections between their personal fears and tendencies and the impact of such qualities on the care they deliver to others. Our hope is that the HAPSI will be a valuable assessment tool to be used in conjunction with intensive antistigma interventions or more simply as a way for providers to become mindful of and address their mixed feelings about working with PLHA. It is important to emphasize that the HAPSI was designed to encourage reflection on subtle issues. Indeed, the Awareness and Acceptance scales include a variety of complex notions and complicated stems for items that require careful reading and consideration. The results reported here and our anecdotal experiences in piloting the instrument suggested that respondents are able to track and respond appropriately to the items as designed.
The HAPSI provides a valid and reliable form of measurement for use among nurses as well as other health care and social service providers, and offers a measurement strategy that is especially appropriate for interventions that integrate the mindfulness principles detailed above and elsewhere. 1 Professional socialization is perhaps one of the most important components of training in health care and social services. It is essential that this initial period of socialization integrates not only the technical skills related to the care of PLHA, but also the interpersonal skills necessary to promote their continued involvement in treatment. Failure to do so will facilitate the persistence of stigmatizing behaviors among entry level professionals with little experience or preexisting desire to care for PLHA.
Limitations
Generalizations beyond this initial validation should be undertaken with caution given the nature of the student sample, which was homogenous due to respondents' common level of training, education, and clinical exposure. Respondents had limited clinical experience, and reported only modest motivations to work with PLHA. As with all validation studies, which are inherently sample-dependent, replications on broader and more diverse samples are recommended. In addition, the utility of scales focusing on attitudes can be strengthened through tests involving behavioral applications. The goals of this project were ambitious, resulting in a long data collection instrument. This may have inhibited some respondents from participating. This restricted the available space for a more thorough inclusion of construct validity indicators; however, the relative absence of measures of provider stigma also limited a more extensive assessment of construct validity. Revalidation on a sample of more experienced health care and social service practitioners as well as testing the utility of the HAPSI with behavioral indicators, including simulations and direct observation of provider–patient interactions, will address this limitation and add indicators assessing concurrent criterion validity.
Footnotes
Acknowledgement
The authors thank the 10 expert panelists who provided critical assistance with conceptualization.
Author Disclosure Statement
The authors report no real or perceived vested interests that relate to this article (including relationships with pharmaceutical companies, biomedical device manufacturers, grantors, or other entities whose products or services are related to topics covered in this article) that could be construed as a conflict of interest.