
Abstract
The innate proatherosclerotic properties of non-nucleoside reverse transcriptase inhibitors have not previously been examined. Therefore, we performed a pilot study of etravirine (ETR) in healthy volunteers over 28 days. This investigation also allowed us to evaluate the safety of ETR over a period commonly used for HIV postexposure prophylaxis. ETR 200 mg twice daily was given to 28 healthy HIV-uninfected volunteers over 28 days. Flow-mediated dilation (FMD) of the brachial artery and circulating markers of inflammation, coagulation, and metabolism were measured at entry and at day 28. These circulating markers were also measured at day 35. Of the initial 28 subjects, 23 completed both entry and day 28 procedures. Two subjects were discontinued due to development of rash. No other major toxicities developed. The change in FMD over 28 days was minimal and not significant (0.03 [−3.21, 0.97] %; p=0.36). The post hoc estimated detectable absolute change in FMD with the 23 subjects in our study was 2.26%, which is an effect size that has been associated with future cardiovascular event rates in the general population; thus our study had sufficient power to find clinically relevant changes in FMD. In addition, there were no significant changes in any of the circulating markers from entry to day 28 or from day 28 to day 35. ETR did not demonstrate any innate proatherosclerotic properties over 28 days in these HIV-uninfected volunteers. ETR was generally well tolerated. Larger studies are warranted to confirm that ETR can be used safely as part of HIV postexposure prophylaxis regimens.
Introduction
C
Dysfunction of the vascular endothelium results in an impaired availability of endothelium-derived nitric oxide (NO), which is responsible for vascular dilation and the prevention of proatherogenic processes. 7 Endothelial dysfunction, typically measured by flow-mediated dilation (FMD) of the brachial artery, is a key, initial step in the development of atherosclerosis and has been shown to predict future cardiovascular events in most population studies. 8,9
Older generation protease inhibitors and some nucleoside reverse transcriptase inhibitors have been associated with impaired endothelial function. 10,11 However, more recent data suggest that newer protease inhibitors may not be associated with impaired endothelial function. 12,13 This suggests that the therapy-associated impairment of endothelial function is not class specific but rather drug specific. It is, therefore, important to determine the impact of each individual antiretroviral therapy on endothelial function. Studies in HIV-uninfected healthy volunteers can provide insight into the innate properties of a drug without the confounding influence of HIV itself on proatherosclerotic pathways. 14 Although commonly used, non-nucleoside reverse transcriptase inhibitors (NNRTI) have not previously been studied for any potential innate proatherosclerotic properties. Thus, we evaluated in this pilot study the effects of etravirine (ETR) in HIV-uninfected volunteers.
Contrary to efavirenz, a first-generation NNRTI with potentially teratogenic effects, ETR does not appear to have such concerns 15 and thus could be used as part of HIV postexposure prophylaxis (PEP). Thus, this study also provided an opportunity to study the safety of ETR in uninfected subjects over a period typically used for HIV PEP.
Methods
We performed a single-arm, open-label trial of ETR 200 mg orally twice daily, which is the recommended dosage for treatment of HIV infection, 15 for 28 days in HIV-uninfected, healthy volunteers. The 28-day duration was chosen as this period is in line with Food and Drug Administration (FDA)-approved indications for use of antiretrovirals in studies involving healthy volunteers. After eligibility was confirmed at a screening visit, the subjects entered the trial within 28 days of screening. At this entry visit, after laboratories and brachial reactivity measurements were obtained, the subjects initiated ETR dosing. Graded clinical and laboratory toxicities were recorded throughout the trial. Development of any grade 2 or greater toxicity resulted in ETR discontinuation. Adherence at day 28 was assessed by self-reported 3-day recall. This study was approved by the Indiana University Institutional Review Board and listed in ClinicalTrials.gov (NCT00871234). All subjects provided written, informed consent.
All subjects were at least 18 years of age, were neither pregnant nor breastfeeding, had not smoked for 1 year prior to screening, and had negative hepatitis B surface antigen and hepatitis C antibody at screening. In addition, subjects were excluded if they had known vascular disease, hypertension, diabetes, dyslipidemia, untreated thyroid disease, serious infection or other illness treated within 14 days of screening, or received anti-inflammatory medications (including nonsteroidal anti-inflammatory drugs and systemic glucocorticoids) within 30 days of screening.
Brachial artery reactivity testing was performed at entry and at day 28 according to established guidelines. 16 An Acuson CV70™ ultrasound system (Siemens Healthcare, Deerfield, IL) with a 10-MHZ linear-array vascular probe was used to visualize the brachial artery 1–2 cm above the antecubital fossa. FMD was estimated as the larger percent increase in brachial artery diameter measured at 60 and 90 sec after release of a blood pressure cuff (which had been inflated to 250 mm Hg for 5 min around the forearm) compared to the resting baseline value. Twenty minutes after cuff deflation, 0.4 mg of sublingual nitroglycerin was administered; nitroglycerin-mediated dilation (NTGMD) was estimated as the percent increase in brachial artery diameter 3 min after the administration of NTG compared to the pre-NTG value. Brachial artery diameters were measured in triplicate at end-diastole with digital calipers (AccessPoint 2004 software; Freeland Systems, Inc.; Indianapolis, IN). All ultrasound procedures were performed by a single technician, and all vascular measurements were made by a single investigator (S.K.G.). The ultrasound images were not dated and were presented to the ultrasound reader as random sequences to enhance blinding.
Circulating plasma markers of inflammation (interleukin-6 [IL-6], interferon-γ–inducible protein 10 [IP-10], monocyte chemoattractant protein-1 [MCP-1], soluble tumor necrosis factor receptors types 1 [sTNFR1] and 2 [sTNFR2], intercellular adhesion molecular-1 [ICAM-1], vascular cell adhesion molecule-1 [VCAM-1], high sensitivity C-reactive protein [hsCRP]) and coagulation (fibrinogen, plasminogen activator inhibitor-1 [PAI-1] active, von Willebrand factor [vWF]) were measured using a custom multiplex assay (Aushon Biosystems, Billerica, MA) after overnight fasts at entry and day 28 prior to brachial reactivity testing. In the event that any of these biomarker levels significantly changed from entry to day 28, we also made these same biomarker measurements at day 35 (1 week after ETR cessation) to determine if these levels returned toward baseline levels to support temporal causality. Serum lipid fractions, glucose, and insulin were measured (Clarian Pathology Laboratories, Indianapolis, IN) and the homeostasis model assessment-insulin resistance (HOMA-IR) 17 was calculated at these same time points. These laboratories were measured in batch at the end of the trial.
Continuous data are presented as median (quartile 1, quartile 3) whereas categorical data are presented as frequencies and percentages. The Wilcoxon signed-rank test was used to compare within-subject continuous variables. Spearman's rank correlation was used to assess for relationships between changes in circulating biomarkers and changes in FMD. Linear regression was used to assess for relationships between baseline levels in biomarkers and change in FMD. Assuming no change in FMD over 28 days with no intervention, an evaluable sample set of at least 20 subjects was considered sufficient to find a change in FMD with ETR with 80% power and an α of 0.05. 18 A p value<0.05 was considered statistically significant.
Results
A total of 31 subjects were screened for this study. One subject failed screening and 2 others were found to be eligible but then were lost to follow-up prior to study entry. Thus, 28 subjects entered the study and completed entry visit procedures. Two subjects developed grade 2 rashes within 14 days of entry and were discontinued from study participation; rash resolved within 3 days in both subjects. Three other subjects were lost to follow-up by day 28, and then 2 others were lost to follow-up between days 28 and 35. Of the 23 subjects who completed the day 28 study visit, 21, 1, and 1 claimed 0, 1, and 6 missed doses, respectively, in the 3 days prior to this visit.
Of the 28 subjects who entered the trial, 46% were female and 46% were black. The median (IQR) age, body mass index, and systolic blood pressure were, respectively, 40 (28, 47) years, 25.4 (22.4, 31.3) kg/m2, and 114 (102, 123) mm Hg. As shown in Table 1 and Fig. 1, median (IQR) entry FMD and NTGMD in the 23 subjects with data available at both entry and at day 28 were 3.70 (1.39, 6.92) % and 20.10 (14.60, 21.22) %, respectively. The median (IQR) change in FMD from entry to day 28 was 0.03 (−3.21, 0.97), p=0.36 (Fig. 1). NTGMD also did not significantly change from entry to day 28. There were no significant changes in any of the circulating biomarkers or in systolic blood pressures from entry to day 28 or from day 28 to day 35 (Table 1). No significant correlations between changes from entry to day 28 in any biomarker and changes in FMD were found. Changes in FMD were not associated with the baseline level of any biomarker.
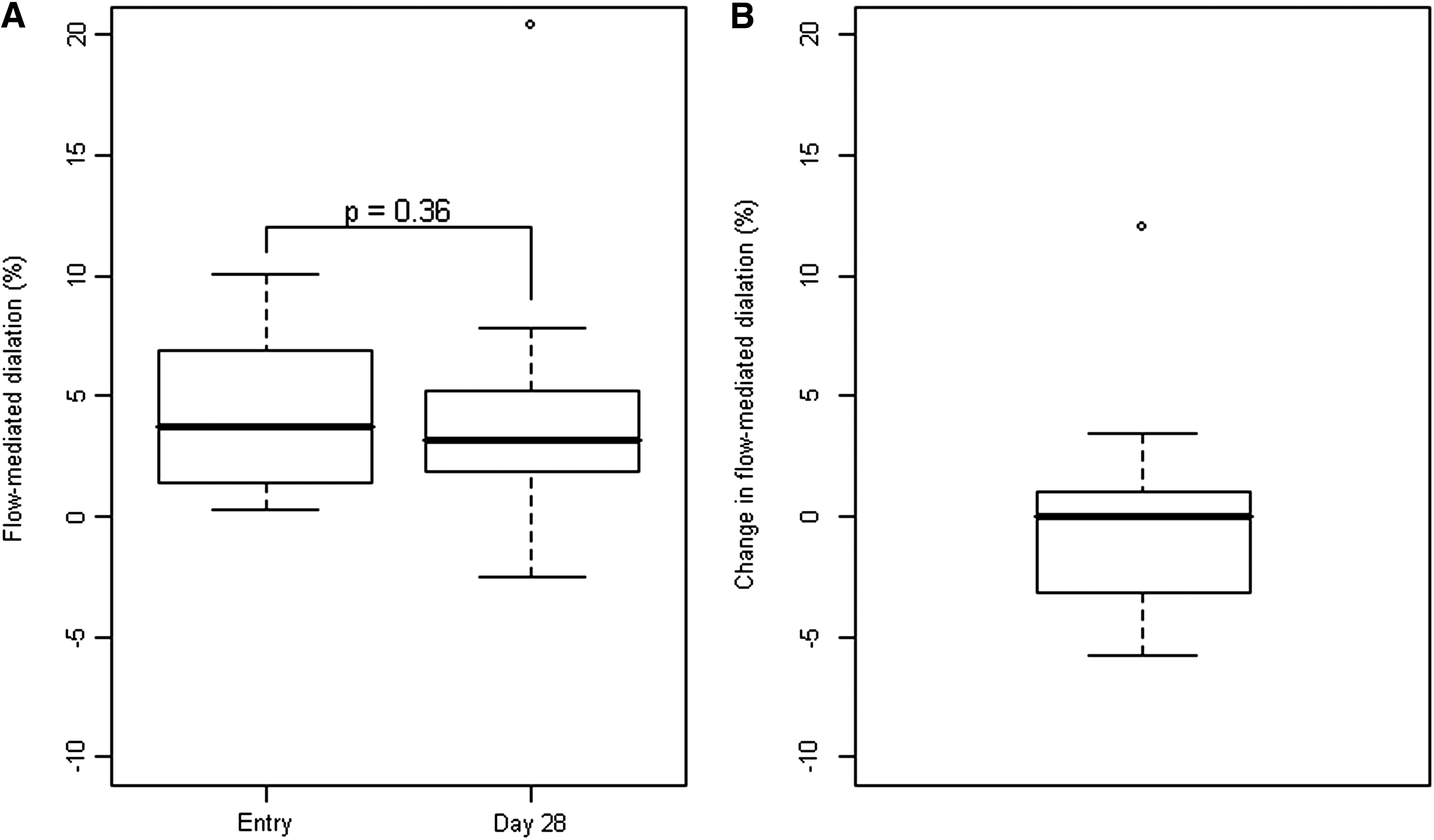
Boxplots of flow-mediated (FMD) dilation of the brachial artery in the 23 subjects who completed the trial. (
Note: Data are shown for the 23 subjects who completed both entry and day 28 study procedures and for the 21 subjects who completed the day 35 study procedures. There were no significant changes in any parameter from entry to day 28 or from day 28 to day 35. ND, not done.
Data are presented as median values (quartile 1, quartile 3).
There were no serious adverse events nor any graded laboratory toxicities. Except for the two subjects with rash, all other clinical adverse events considered at least possibly attributable to ETR were considered mild (grade 1) and were not study treatment limiting. The events reported by at least 2 subjects included: neuropathic tingling or pain in 2 subjects (both resolved spontaneously within 3 days); diarrhea in 2 subjects (both spontaneously resolved within 11 days); nausea or vomiting in 2 subjects (both resolved within 2 days); constipation in 3 subjects (all resolved within 11 days); headache in 4 subjects (all resolved within 12 days); and dizziness in 2 subjects (both resolved within 2 days).
Discussion
We did not find evidence that ETR affected in vivo endothelial function or other assessed cardiovascular disease risk factors in HIV-uninfected volunteers.
The lack of changes noted in lipids in this study corroborates those found in HIV therapeutic trials. 19, 20 We also found that 28 days of ETR did not influence levels of inflammatory markers known to be associated with an increased risk of CVD in the HIV-infected population, namely IL-6 and hsCRP. 21 Furthermore, there were no changes in the coagulation markers fibrinogen, vWF, and plasminogen activating inhibitor-1 antigen. Thus, it was not surprising to find that short-term use of ETR did not affect FMD, a dynamic and physiologic measure of in vivo endothelial function. Supporting the lack of innate effects of etravirine on endothelial function was the absence of changes of other endothelial activation markers such as sVCAM-1 and sICAM-1.
There were no effects on renal function, hematopoetic, or hepatic injury markers in our trial. However, 2 subjects developed grade 2 rashes, which promptly resolved upon ETR discontinuation. This rate of 7% (2/28) is consistent with those reported in the package insert of ETR. 15 ETR has been associated with severe rash, and rarely with death due to Stevens-Johnson syndrome, in HIV-infected patients. All other clinical adverse events were mild and not treatment-limiting. Thus, it appears that use of ETR over 28 days in uninfected persons is generally safe, but larger studies of its use as part of HIV PEP are needed to establish the safety of this agent, especially in regards to rash.
Several limitations of this study should be acknowledged. First, no control group was used in this initial study of ETR. The potential bias in FMD reading without a blinded control group is of minimal concern as aforementioned due to the randomization of sequences (entry versus day 28 scans) presented to the reader. We argue that healthy subjects on placebo without any known CVD risk factors would be expected not to have changes in FMD or other circulating biomarkers over the short period of 28 days, therefore any significant changes within the ETR-receiving group would be highly suggestive of a true effect and would thus warrant future controlled studies. Our findings that neither FMD nor any circulating biomarkers changed strongly suggest that ETR likely does not have any real short-term effects on these CVD markers. We also calculated the change in FMD that we could have detected with the 23 subjects who completed our study protocol. We observed a variability of 3.7 in the change in FMD at day 28 from entry. Using a paired t-test and type I error rate of 5%, a sample size of 23 would have 80% power to detect a mean absolute change of 2.26% in FMD. The detectable median absolute change in FMD would be a litter bigger than 2.26% using the Wilcoxon signed-rank test because of this test's nonparametric nature. Given that changes in FMD of 3% 22,23 have been associated with future cardiovascular events in the general population, we believe that the detectable effect size in our study is clinically relevant.
In addition, we cannot rule out the possibility that a longer duration of etravirine use would eventually have affected FMD or the other circulating biomarkers measured in this trial. However, two other studies found changes in endothelial function measured using alternative techniques within a 4 week period in healthy volunteers given indinavir 24 and lopinavir/ritonavir. 25 These results suggest that changes in endothelial function can occur rapidly. It should be acknowledged that the interactions between HIV infection itself and drug-mediated effects on vascular health are likely to be complex and unpredictable. Finally, it should be noted that the lack of effects of ETR on CVD risk markers found in this study may not be generalizable to other drugs in the NNRTI class.
In conclusion, ETR was generally well-tolerated in this cohort. ETR did not result in short-term changes in inflammatory, coagulation, metabolic, or endothelial function measures in healthy, HIV-uninfected volunteers.
Footnotes
Acknowledgments
We thank Ms. Beth Zwickl for her role in study coordination, Mr. Jeffrey Waltz for his role in vascular ultrasonography, and Ms. Cheryl Denski for her role in data management, all of which was invaluable in completing this study. Most of all, we thank the trial participants for generously donating their time and effort during this trial.
This study was supported through an unrestricted research grant from Tibotec Therapeutics. Tibotec Therapeutics had no role in the design, implementation, analysis, or decision to publish the results of this study. All authors had full access to the data and take full responsibility for the accuracy of the data analysis. Additional procedural support was provided by the Indiana Clinical and Translational Sciences Institute, Indiana Clinical Research Center, UL RR025761.
Author Disclosure Statement
Dr. Gupta is the site Principal Investigator and member of the writing committee for another study sponsored by Tibotec Therapeutics (NCT00757783). All other authors have no disclosures.