
Abstract
Kaposi's sarcoma (KS) in women with HIV infection is observed to have increased from recent studies. To understand the gender-related differences of AIDS-KS in Nigeria, we conducted a prospective study of the clinical, virologic, and immunologic features of newly diagnosed AIDS-KS patients. Prevalence was similar in both genders. There were differences in the distribution of the lesions and the CD4 count in women was significantly lower.
Introduction
K
To understand better the gender-related differences of AIDS-KS in Nigeria, we conducted a prospective study of the clinical, virologic, and immunologic features of newly diagnosed AIDS-KS patients. This study provides essential data on the demographic and clinical patterns of AID-KS seen in Ibadan, Nigeria.
Methods
Confirmed HIV-1–infected patients with clinical and histologically proven KS were recruited into the study between October 2008 and September 2009. Patients were recruited from the medical outpatients and antiretroviral (ARV) clinics of the University College Hospital Ibadan, Nigeria. The hospital is located in the southwest of the country and serves as a referral center for an estimated catchment population of approximately 20 million. Relevant biodata and information to assess the route of HIV transmission and other associated comorbidities were obtained. The morphology of the lesions and sites of involvement was also documented.
Cutaneous involvement was classified as local when confined to one anatomic site and extensive when involving two or more sites. Investigations done included blood counts, CD4 T-cell and HIV-1 viral loads (VL). KS was staged into good and poor prognosis categories according to the AIDS Clinical Trial Group (ACTG) criteria, which is based on the clinical pattern, CD4 count, and systemic symptoms of the patients. 8 Results were analyzed using SPSS package version 16 (SPSS, Chicago, IL).
Results
A total of 13 adult patients with AIDS-KS of 2689 newly diagnosed HIV patients (prevalence of 0.5%) were recruited within the study period. All were heterosexual. The ratio of men (n=7) to women (n=6) was 1:1. The women were significantly younger (mean age 35 years, standard deviation [SD]=10.64) than men (mean age 38 years, SD=4.76; p=0.03; Table 1).
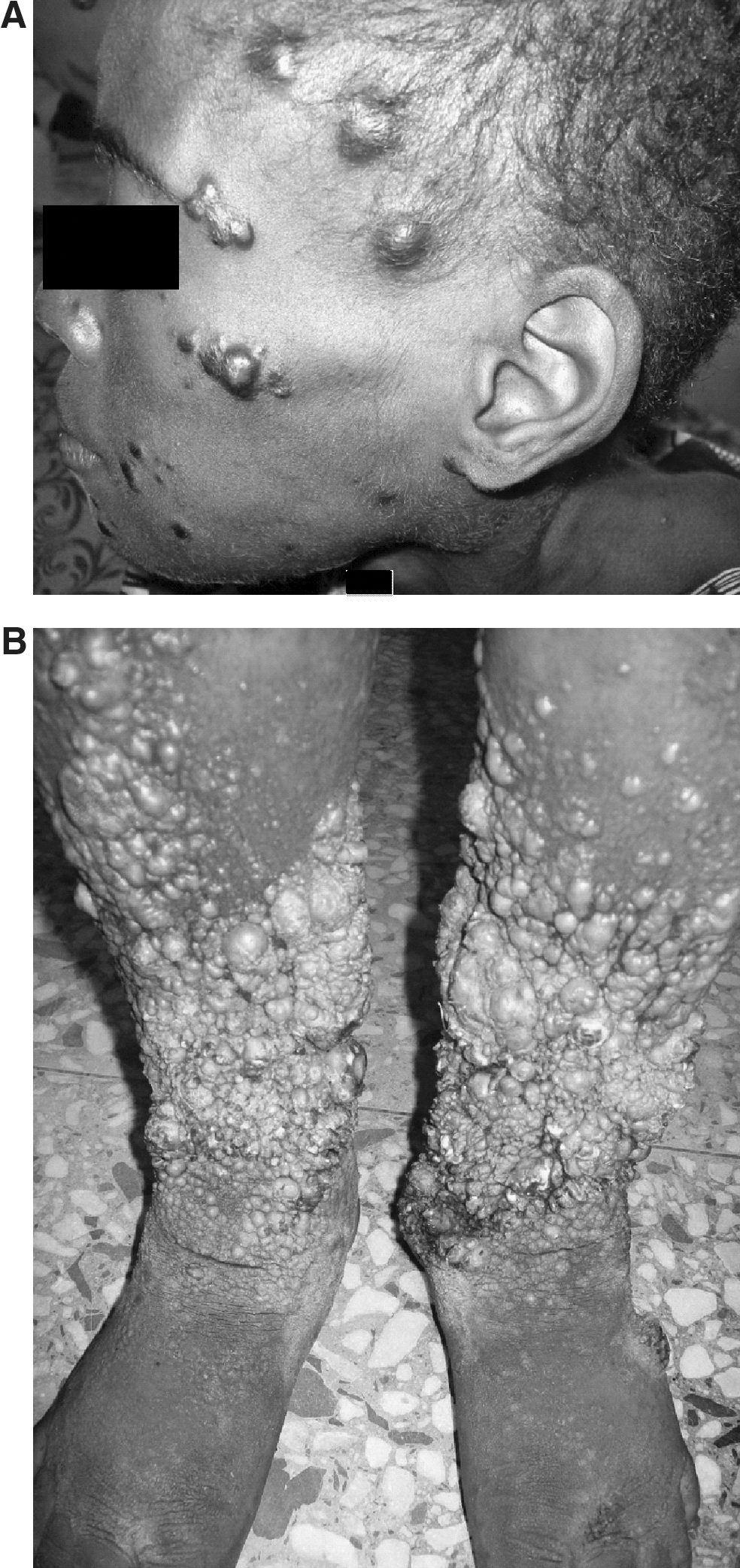
The mean duration of the lesions before presentation for the men was 9.57 months (SD=5.68 95% confidence interval [CI)=4.3–14.8) and for the women 7.67 months (SD=4.08, CI=3.4–11.9). One male and one female had localized cutaneous involvement on the right lower limb and face, respectively. The types of presenting lesions were similar in both genders; macules, papules, plaques, nodules, and tumorous lesions. Hyperkeratotic lesions were seen mainly on the lower limbs. The number of KS lesions on the lower limbs was obviously higher in the males. Females presented with KS lesions on the face and neck region, facial lesion was seen in only one male patient (Fig. 1).
When classified into “good” and “poor” risk groups using the ACTG clinical staging system for KS only one male was found to have good disease prognosis. He had localized lesion on the left leg, a CD4+ count of 260 cells/mm3 and no other systemic illness, although his HIV-1 viral load was 1.4 million copies per microliter.
The mean peripheral blood CD4+ T-cell count for the subjects was 199 (range, 13–743, 95% CI=90–309) cells/mm3 There was an observed significant difference between the males and females. Males had a mean CD4+ T-cell count of 268 (range, 82–743, 95% CI=60–475) cells/mm3 and females, 120 cells/mm3 (range, 13–203, 95% CI=50–190; p=0.02). In contrast there was no significant association between gender and differences in log10HIV-1 VL (p=0.29). The mean HIV-1 VL for the entire subjects was 4.90 log10 (range, 2.30–6.34, 95% CI=4.10–5.70) when compared with 4.79 log10 (range, 2.30–6.34, 95% CI=3.17–6.40) and 5.03 log10 (range, 4.04–5.75, 95% CI=4.28–5.78) copies per milliliter of plasma for males and females, respectively.
Five of the patients (4 women and 1 man) died within the course of the study. They had severe bone marrow suppression and clinical evidence of KS dissemination into the gastrointestinal and respiratory tracts respectively. These patients were also managed for tuberculosis. Three patients (2 men and 1 woman) who had localized and few extensive KS lesions responded to protease inhibitor combined antiretroviral therapy (ART) with a gradual regression of the lesions. Vincristin, cyclophosphamide, and adriamycin were given to three patients (3 men) with extensive and tumorous lesions. They had absence of comorbidities and showed no response to ART. The lesions reduced to approximately half its size following one course of chemotherapy that they received within the study period. Two patients were lost to follow-up.
Discussion
Our findings are similar to those from other African countries like South Africa, Tanzania, Uganda, and Zimbabwe with respect to high prevalence of females with AIDS-KS while endemic KS remains a male dominated disease. 6 The reason is yet to be fully understood, and may be related to a higher titer of HHV8 in HIV-infected women or to a gender difference in the pathophysiology of HIV; since a high percentage of the people living with HIV infection are women. 4 The women in our study presented at a younger age group. This may be explained by the epidemiology and transmission patterns; with young women having a higher biological vulnerability to HIV-1 and other sexually transmitted infections such as HHV8 than young men. Also sexual relations between young women and older men, who are more likely to be infected than younger men is quite common. 9 Further research into the relationship between HIV and HHV8 is needed for a better understanding of this trend.
The morphology of the lesions was similar in both sexes. Hyperkeratosis was commoner on the lower limbs. It was interesting to observe the dissimilarity of the distribution of these lesions anatomically between the two genders. The lesions were observed more on the head and neck region for the women and lower limbs for the men. The reason is not quite clear. Women also seen at follow-up (within 3 months), had developed visceral KS (gastrointestinal, lungs, and bone marrow) and were generally unresponsive to treatment. This was also observed in Uganda. 10
Our study demonstrated a significant difference in the CD4+ counts p=0.02 between the two gender and thus, an increased disease severity in the women. This gender-related correlation between disease severity and CD4+ T-cell count is in agreement with an Italian study 11 but at variance with the South African and Zimbabwe studies. 6 In the South African study, the gender difference in CD4+ T-cell count was not significant but they were able to establish a relationship between the count and advanced KS disease/poor disease prognosis.
In conclusion, our investigation highlights and strengthens previous studies of AIDS-KS in women. Most importantly is that the prevalence of KS in women living with HIV infection is similar to that of men. Women appear to have a more aggressive progression of the illness especially when there is significant immunosuppression. Thus, their low CD4 counts may be responsible for their advanced presentation. We suggest early commencement of antiretroviral therapy even with high CD4 counts especially when there are other factors predisposing to KS such as HHV8.
Footnotes
Author Disclosure Statement
No competing financial interests exist.