
Abstract
A 27-year-old white male, who had sex with other men, presented to the emergency department with 3 days of left shoulder and abdominal pain. He reported no history of trauma to the abdomen. On abdominal imaging, he was found to have hemoperitoneum from a ruptured spleen; he underwent splenectomy. Causes of atraumatic splenic rupture can be divided into six main categories: infectious, neoplastic, inflammatory, congenital or structural, iatrogenic, and idiopathic. Work-up of the atraumatic splenic rupture revealed that his HIV antibody was newly positive. He had a documented negative HIV antibody 3 weeks prior to the current admission. CD4 cell count, obtained after splenectomy, was 904 cells per microliter and the HIV-1 plasma RNA level was 4657 copies per milliliter. Spleen pathology demonstrated an enlarged spleen with increase in the number of small to intermediate size lymphoid cells in the red pulp, and reactive follicular lymphoid hyperplasia, with numerous secondary lymphoid follicles and reactive germinal centers in the white pulp. T-cell receptor (TCR) gene rearrangement studies demonstrated a positive TCR beta gene rearrangement, without a TCR gamma gene rearrangement, consistent with a clonal CD8+ T-cell population. The case gives rare insight into what happens in the spleen during acute HIV infection and encourages HIV testing in those presenting with atraumatic splenic rupture. Counseling patients with acute HIV to avoid potential trauma should also be considered.
Case Report
A 27-
Past medical history was significant for depression, bulimia, obesity, and abdominoplasty after losing 140 lbs by lifestyle modifications. He had no drug allergies. His only medication was Zoloft® (Pfizer, Inc., New York, NY).
The patient lives in California and works as a nurse. He smokes 1 pack of cigarettes per week, consumes alcohol occasionally, and denied illicit drug use. He reported no recent travel. He was sexually active with men. He had a documented negative HIV serum antibody test in the hospital electronic medical record 3 weeks earlier.
On presentation, he was afebrile with a temperature of 36.7°C, blood pressure of 105/70, heart rate of 84, respiratory rate of 18, and oxygen saturation of 100% on room air. His physical examination was notable for diffuse abdominal tenderness to palpation without peritoneal signs. Admission labs were significant for a hematocrit of 28%, but other cell lines were normal, with white blood cell count of 7.6×103 cells per microliter and platelet count of 148,000×106 per liter. His coagulation labs were within normal range, with international normalized ratio (INR) of 1.2 and partial thromboplastin time (PTT) of 25.2 sec. Other routine laboratory tests including creatinine and liver function tests were also normal. An abdominal computed tomography (CT) revealed hemoperitoneum, suspected to arise from a large perisplenic or subcapsular hematoma (Fig. 1).
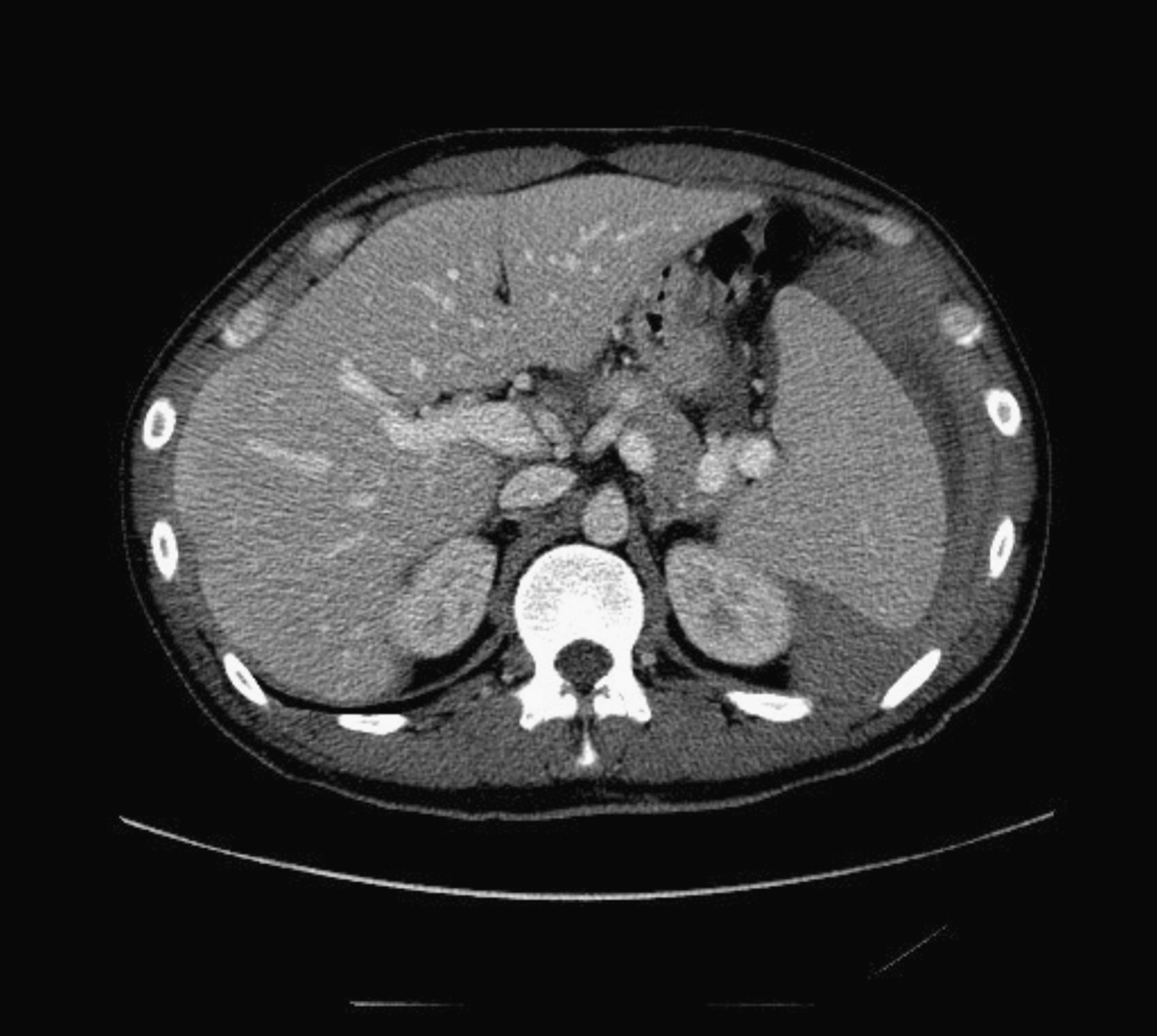
Abdominal computed tomography (CT) scan of a 27-year-old man presenting with abdominal pain secondary to splenic rupture, subsequently determined to be due to acute HIV infection.
The patient was admitted to the general surgery service. His hematocrit remained stable and he was initially managed conservatively with intravenous fluid resuscitation. An abdominal CT angiogram showed no active extravasation of blood, no visceral artery aneurysms, and no tumors within the abdomen. However, given his continued pain and new fevers, a diagnostic laparoscopy was performed on hospital day two. This revealed a large hemoperitoneum, splenomegaly with an associated subcapsular hematoma, and a ruptured splenic capsule. A laparoscopic splenectomy was performed. The rest of his hospital course was unremarkable and he was discharged 2 days later.
On pathologic evaluation, the spleen was enlarged by approximately two- to threefold, measuring 25×14.5×5.6 cm and weighing 597 grams (normal adult spleen weight is approximately 200 grams). Splenic architecture was preserved overall, with discrete zones of white and red pulp, and distinct cords and sinuses within the red pulp. However, there was a marked increase in the number of small to intermediate size lymphoid cells in the red pulp, along with scattered large lymphoid cells that were infiltrating both red pulp cords and sinuses. The splenic white pulp showed reactive follicular lymphoid hyperplasia, with numerous secondary lymphoid follicles and reactive germinal centers. Lymphoid cells of the periarteriolar lymphoid sheath of the splenic white pulp, as well as the red pulp stained strongly positive for the T-cell marker, CD3. The great majority of these T-cells stained positive for CD8 markers; the ratio of CD4:CD8 cells in the spleen was 1:20 (Fig. 2). In situ hybridization for Epstein Barr virus (EBV)-encoded RNA showed no nuclear staining in lymphoid cells. T-cell receptor (TCR) gene rearrangement studies demonstrated a positive TCR beta gene rearrangement, without a TCR gamma gene rearrangement, consistent with a clonal cell population.
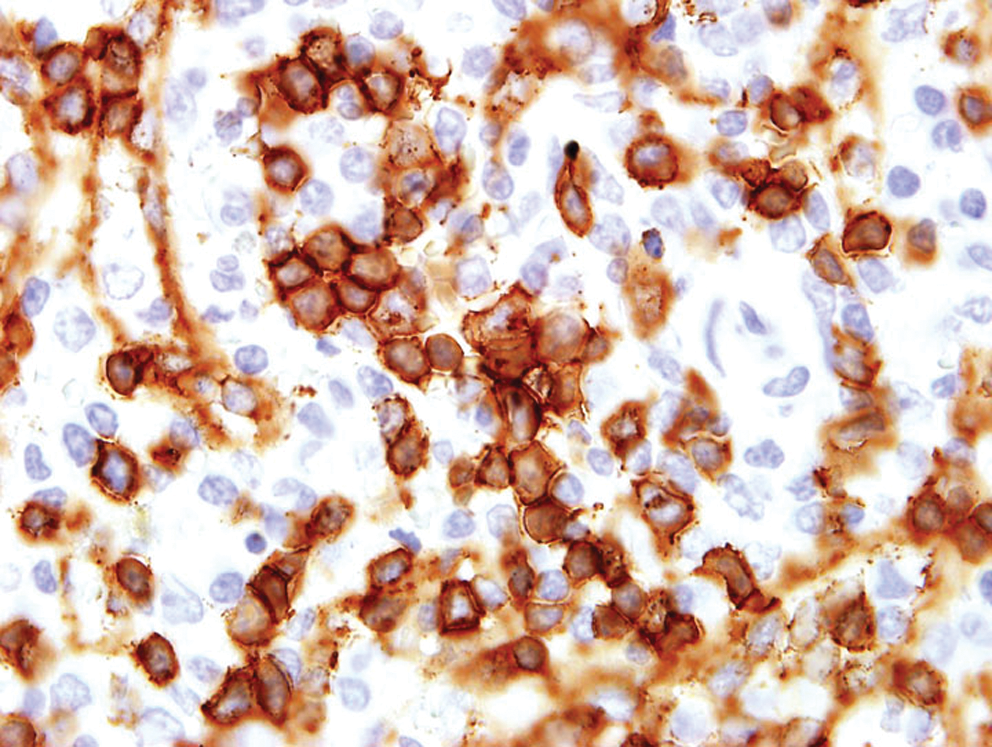
Increased numbers of CD8+ T-cells in splenic red pulp of a patient with atraumatic splenic rupture secondary to acute HIV infection. CD4:8 T-cell ratio estimated at 1:20. (Color image can be found at
Several serologic studies were sent to rule out infectious causes of atraumatic splenic rupture. EBV IGG was positive, but EBV IgM was negative. Cytomegalovirus (CMV) IgG was positive; CMV polymerase chain reaction (PCR) was not performed. A viral hepatitis panel was negative. Two weeks after the patient's initial presentation, the HIV antibody test and confirmatory Western blot returned as positive. The western blot, while positive, lacked the p31 band. This finding, along with his negative antibody test 3 weeks prior to presentation, confirmed acute HIV infection. Subsequently, a CD4 cell count was found to be 904 cells per microliter and the HIV-1 plasma RNA level was found to be 4657 copies per milliliter.
Some of the pathologic features, especially the TCR beta gene rearrangement, raised suspicion T-cell lymphoma of the spleen, particularly hepatosplenic T-cell lymphoma. The patient was seen in the oncology clinic. To rule out lymphoma, a chest CT was performed and revealed no calcified pulmonary nodules; he only had scattered hilar and mediastinal lymph nodes consistent with old granulomatous disease. A bone marrow biopsy showed no features concerning for malignancy. After HIV genotyping and discussion of early antiretroviral treatment, the patient opted to initiate treatment with coformulated tenofovir/emtricitabine/efavirenz (Atripla®, Bristo-Myers Squibb, New York, NY).
Discussion
We describe the case of a young man who presented with atraumatic splenic rupture in the setting of confirmed acute HIV seroconversion. Atraumatic spontaneous splenic rupture is a rare but potentially fatal entity. It is defined as rupture of the spleen without antecedent trauma with findings of normal or abnormal splenic pathology under gross and histologic observation.
Causes of atraumatic splenic rupture can be divided into six main categories: infectious, neoplastic (e.g., acute myelogenous leukemia, non-Hodgkin's lymphoma, idiopathic thrombocytopenic purpura, angiosarcoma, and malignancies that metastasize to the spleen); inflammatory (e.g., chronic pancreatitis, amyloidosis, polyarteritis nodosa, and lupus); congenital or structural (e.g., hemangiomas, pregnancy, and portal hypertension); iatrogenic (e.g., anticoagulation, granulocyte colony-stimulating factor, and hemodialysis); and finally idiopathic. 1
The most common infectious cause of atraumatic splenic rupture reported in the literature is infectious mononucleosis, and in fact, atraumatic splenic rupture is the leading cause of death in Epstein Barr virus-linked infectious mononucleosis. 2 There are case reports of spontaneous splenic rupture from other viruses, including CMV, influenza, and dengue. Bacterial causes that have been reported include tuberculosis, typhoid fever, and syphilis. Among protozoa, malaria is the most common etiology. Echinococcal cysts, schistosomiasis, and leishmaniasis are among other infectious causes of splenic rupture.
Splenic rupture has been reported in patients with HIV in association with splenic lymphoma, 3 splenic Kaposi's sarcoma, 4 splenic tuberculosis, 5 and splenic Mycobacterium avium complex infection. 6 However, there has been only one prior case report of spontaneous rupture of the spleen in the setting of confirmed acute HIV infection. 7 In that case, a 60-year-old man was admitted with hypotension, and found to have a ruptured spleen. Evaluation of the spleen after splenectomy revealed lymphoid infiltration of the subendothelial layer of the intratrabecular veins. This patient had a negative HIV antibody test, but had high level of p24 antigen in the serum. (One other case report describes a 25-year-old injection drug user who died from an atraumatic splenic rupture and was found to be HIV positive on postmortem examination, although the stage of infection was not determined). 8
There have been five published case reports of splenic rupture after vomiting. 9 –13 These cases were attributed to food poisoning (2 cases), constipation, a reaction to a metrizamide injection, and ibuprofen. On examination in each of these cases, the spleen was macroscopically and histologically normal with no evidence of acute viral infection. In the case presented here, although vomiting could have been a trigger, the splenic rupture occurred in the setting of acute HIV infection.
The CD4:CD8 ratio of 1:20 seen in our patient has been described in splenic rupture caused by EBV as well, and likely represents a rigorous antiviral response. This ratio of CD4:CD8 T cells mirrors what is seen in the peripheral blood a few weeks after acute seroconversion with HIV. The clonality of the T cells prompted a search for malignancy, as described above. This was unrevealing and malignant symptoms have not developed in the many months since his presentation. Clonal expansions of T cells have been reported in the early phase of HIV infection. 14 The T cell clonality in our patient could be attributed to massive response of the patient's immune system against an HIV “superantigen” causing a clonal proliferation of T cells.
The pathophysiology of splenic rupture in the setting of acute HIV infection is unclear. In EBV infection, where splenic rupture is better defined, there is extensive infiltration of the splenic parenchyma with lymphocytes that extend through the trabeculae, capsule, and blood vessel walls. This is thought to compromise the splenic architecture by making the splenic capsule and fibrous support network more fragmented, as well as increasing portal venous pressure. 15 These mechanisms, as well as endothelial cell dysfunction or acute vasculitis, may also play a role in spontaneous rupture caused by acute HIV. 16
We report a unique case of atraumatic splenic rupture in the setting of confirmed acute HIV infection. For physicians and surgeons who diagnose and manage atraumatic splenic rupture, we propose that acute HIV infection be considered as a possible etiology, especially in patients with HIV risk factors. In these cases, HIV viral load should be sent in addition to HIV antibody testing. This case also raises questions about whether to counsel those with acute HIV to avoid trauma that could precipitate splenic rupture.
Footnotes
Acknowledgments
The authors thank Dr. Mike McCune, Dr. Christopher Pilcher, and Dr. Vivek Jain for their review of the manuscript and their insightful comments.
Author Disclosure Statement
No competing financial interests exist.