
Abstract
We assessed HIV prevalence and associated behaviors and risk factors among men who have sex with men (MSM) in Beijing, China. Five hundred MSM were recruited for a biological and behavioral survey using respondent-driven sampling (RDS) in 2009. Serologic specimens were tested for markers of HIV and syphilis infection. A computer-assisted personal interview (CAPI) administered questionnaire gathered information including demographic characteristics, sexual behaviors, HIV testing, and social norms concerning condom use. The adjusted HIV prevalence was 8.0%, syphilis 22.0%. HIV testing and disclosure was low; only 39.3% had HIV tested in the past 12 months, 49.7% knew their own HIV status and 22.8% knew their last male partner's HIV status. HIV infection was associated with syphilis, ever having sex with a woman, not knowing the HIV status of the most recent male partner, and never buying condoms in the past 12 months. Stronger endorsement of positive social norms around condom use strongly and predicted lower prevalence of HIV infection. Compared to surveys of similar design in the recent past, HIV continues to spread rapidly among Beijing's MSM. Our results identify points of intervention that, if addressed in time, may still alter the course of the epidemic including the promotion of HIV testing and partner disclosure, syphilis control and particularly changing social norms around condom use.
Introduction
I
Since the introduction of voluntary counseling and testing (VCT) for the general population and specific testing interventions for MSM, increasing numbers of MSM have tested for HIV and learned their HIV status. 11 Emerging data from around the world point to widespread sexual harm reduction practices among MSM based on knowing their own and their partners' serostatus. “Serosorting” or “seroadaptation,” for example, entails selecting partners, limiting roles in anal sex, or engaging in condom use on the basis of concordant HIV status thus reducing the risk for HIV transmission or acquistion. 12 –17 However, these methods to reduce HIV infection risk have not been formally evaluated for their efficacy; some may be ineffective, some may increase risk. Their very presence and applicability in the Chinese context have not been studied.
A challenge in conducting research among MSM is they are a stigmatized, hidden population in all areas of the world, difficult to access and therefore many surveys rely on convenience sampling. The respondent-driven sampling (RDS) method is a recruitment/sampling approach using long chains of referral for obtaining a more inclusive and, purportedly, more representative sample from hidden populations. 18,19 RDS has been used successfully among MSM in China. 22,36 For the present survey to obtain more reliable estimates of HIV and syphilis prevalence and more detailed behavioral data, we used RDS recruitment and analysis among the MSM population in Beijing, China.
Methods
Participants
A cross-sectional study was conducted among MSM from September 2009 to October 2009 in Beijing. Participants were eligible if they were male, 18 years age or older, a Beijing resident, had sex with another man in the past 12 months (sex can be defined as oral, anal, or mutual masturbation), had a valid study recruitment coupon, had not previously participated in the survey, and were able to provide written informed consent. The study was approved by the Committees for Human Research of the National Center for AIDS of the China Center for Disease Control and Prevention, Vanderbilt University and the University of California San Francisco.
Recruitment
Study participants were recruited using respondent-driven sampling (RDS). Seven MSM were selected to function as recruiter “seeds” and were diverse with respect to the types of venues that they frequented (e.g., bars, parks, bathhouse, and the Internet). Seeds were evaluated for their commitment to the goals of the study and motivation to recruit three eligible peers in their social network. Seeds were each asked to recruit up to three participants, who in turn were asked to recruit a subsequent wave of up to three participants, and so on, until our target sample size was reached and equilibrium was achieved on key variables (age, educational attainment, marital status, occupation, residence, income, anal sex role, number of male sex partners). Equilibrium is achieved when the composition of the sample reaches stability and does not change as recruitment continues to the point sample size is achieved. Equilibrium was achieved in four waves of recruitment or less for all key variables. All subsequent participants had to be a member of the recruiter's social network and meet the eligibility criteria for the study. Each participant was given three recruitment coupons/cards with study information to hand to potential recruits. To keep track of social networks, each card had a number code that connected participants back to the initial seeds. Participants were compensated 30 Yuan (CNY) for their participation in the study, as well as 20 Yuan (CNY) for each eligible participant they recruited who subsequently completed a study interview.
Measures
After providing informed consent, participants completed a CAPI administered questionnaire in a separate room of the Beijing CDC clinic. Trained health professionals conducted the interviews. Each study participant was assigned a unique and confidential identification code for the questionnaire and specimens. Questions included demographic information (e.g., age, ethnicity, education, marital status, occupation, residence, income, and health insurance status), sexual behaviors (e.g., age of the first sex with male and female partners, self-identified sexual orientation, role in anal sex, and the number and types of male and female sex partners in the past 6 months), HIV testing information, and drug using information. We also asked partner by partner sexual behavior (i.e. an assessment of sexual behavior on a partner by partner basis as opposed to an aggregate assessment across all partners), condom use, and HIV status awareness questions for up to three male partners and two female partners within the prior 6 months. A five-item condom use social norms scale was adapted to the China context from previously validated instruments from North America through development with focus group discussions, key informant interviews and pilot testing in the field. 20,21 Items in the scale included such questions as “My friends always use condoms when having anal sex with new partners”, with a 6-point Likert-like scale to record responses (social norms score ranges from 1 to 6 for answering questions of strongly disagree, somewhat disagree, slightly disagree, slight agree, somewhat agree, strongly agree, respectively). The internal reliability of the scale was tested by the Cronbach α (0.925) and assessed for its linear relationship with HIV infection. The complete CAPI administered questionnaire was also pilot tested among MSM volunteers in the real-life survey setting.
Laboratory testing
Serologic specimens collected from participants were tested for syphilis (rapid plasma reagin [RPR] test, Shanghai Rongsheng, China) with confirmation of positive tests by the Treponema pallidum particle assay (TPPA) test (Fujirebio inc., Japan), and HIV-1 antibody (enzyme-linked immunosorbent assay [ELISA], Vironostika HIV Uni-Form plus O, bioMerieux, Holland) with confirmation by Western blot confirmation (HIV Blot 2.2 WBTM, Genelabs Diagnostics).
Data analysis
Survey data were analyzed to produce population point estimates using RDSAT software version 5.6 (
Variables significant at a level of p<0.10 in bivariate analyses were considered candidates for multivariate models. Multivariate logistic regression models were constructed (using RDSAT-generated HIV result weights) to select independent factors for HIV infection, while controlling for potential confounding factors. Both adjusted odds ratio (AOR) and confidence interval (CI) were obtained for each explanatory variable in the final model.
Results
A total of 501 participants were recruited for the study in 2 months; 43.4% (501/1154) of the distributed coupons were actually returned and the holder interviewed. Figure 1 shows the fewest and the highest number of waves achieved was 2 and 13, respectively. One participant was referred to the VCT clinic due to ineligibility (younger than 18 years old). All 500 eligible participants completed the questionnaire and provided blood samples. Table 1 outlines the characteristics of the sample. The median age was 29 years. Most were Han (96.0%) and received a high school (35.6%) or above education (32.9%). Only 4.8% received a primary school or no education. Most men were unmarried (72.8%) and had fulltime jobs (82.5%). The majority (61.2%) of the participants reported having two or more sexual partners in the past 6 months. By self-reported sexual orientation, 61.7% identified as homosexual, 34.7% as bisexual, and only 1.7% as heterosexual. Although most of the participants had known locations for HIV test (89.0%), only 39.3% had HIV tested in the past 12 months. About half (49.7%) of participants know their own HIV status and only 22.8% knew their last male partner's HIV status. Very few (0.1%) acknowledged noninjection drug use; none injected drugs. The adjusted prevalence of HIV was 8.0% (95% CI 4.6–12.2%), 22.0% (95% CI 16.8–27.0%) for syphilis, and 4.2% (95% CI 1.8–7.2%) for HIV and syphilis coinfection.
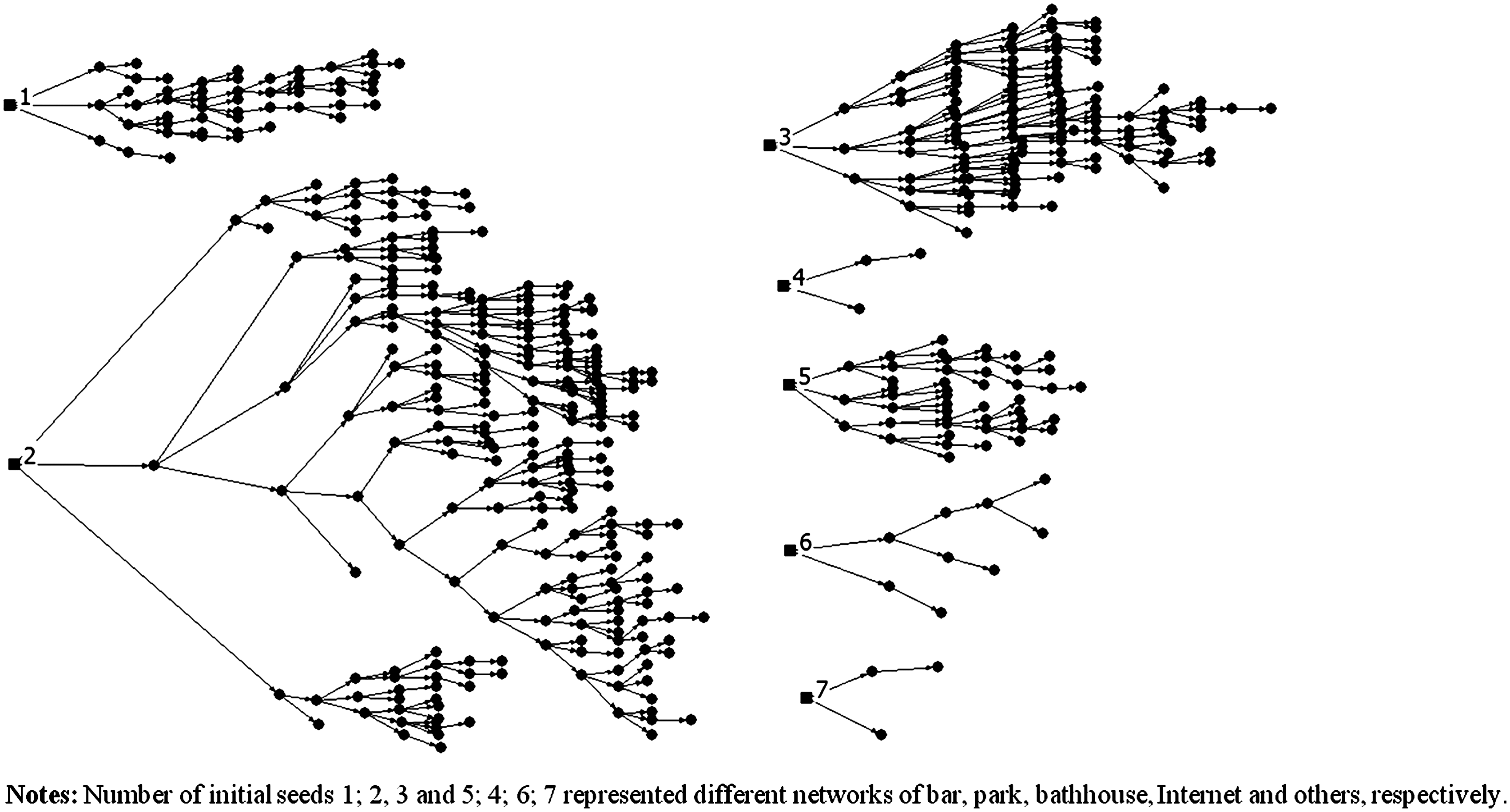
The spread from the various initial seeds.
Composition of the sample when the sample reached stability.
Subgroups do not always add up to totals due to missing data.
Composition of the sample at the end of data collection.
MSM, men who have sex with men; CI, confidence interval.
Table 2 presents the crude and RDSAT-adjusted results of bivariate associations of demographic, sexual risk, and the condom use social norms scale. Significant bivariate predictors of HIV infection were age (older than 25 years), married, lived in Beijing less than 1 year, ever had sex with a woman, had more than one male sexual partner in the past 6 months and syphilis-positive. HIV infection was significantly less likely among MSM who had health insurance, had a regular male partner in the past 6 months, discussed HIV status with the last male partner, known the HIV status of the last male partner, self-reported HIV status to the last male partner and bought condoms in the past 12 months.
Subgroups do not always add up to totals due to missing data.
MSM, men who have sex with men; CI, confidence interval; AOR, adjusted odds ratio.
Table 3 presents adjusted results of multivariable logistic regression for HIV infection. In multivariable analysis, increased risk of HIV infection was associated with being syphilis-positive (AOR 4.7, 95% CI 2.3–9.8), having ever had sex with a woman (AOR 2.7, 95% CI 1.1–6.8), not knowing HIV status of the last male sexual partner (AOR 7.9, 95% CI 1.0–60.9), and not buying condoms within the past 12 months (AOR 2.2, 95% CI 1.0–4.8). Decreased risk of HIV infection was strongly and significantly associated with higher score on the condom use social norms scale (AOR 0.8 per point, 95% CI 0.7–0.9). Figure 2 illustrates the HIV prevalence with the condom use social norms scores among Beijing MSM.
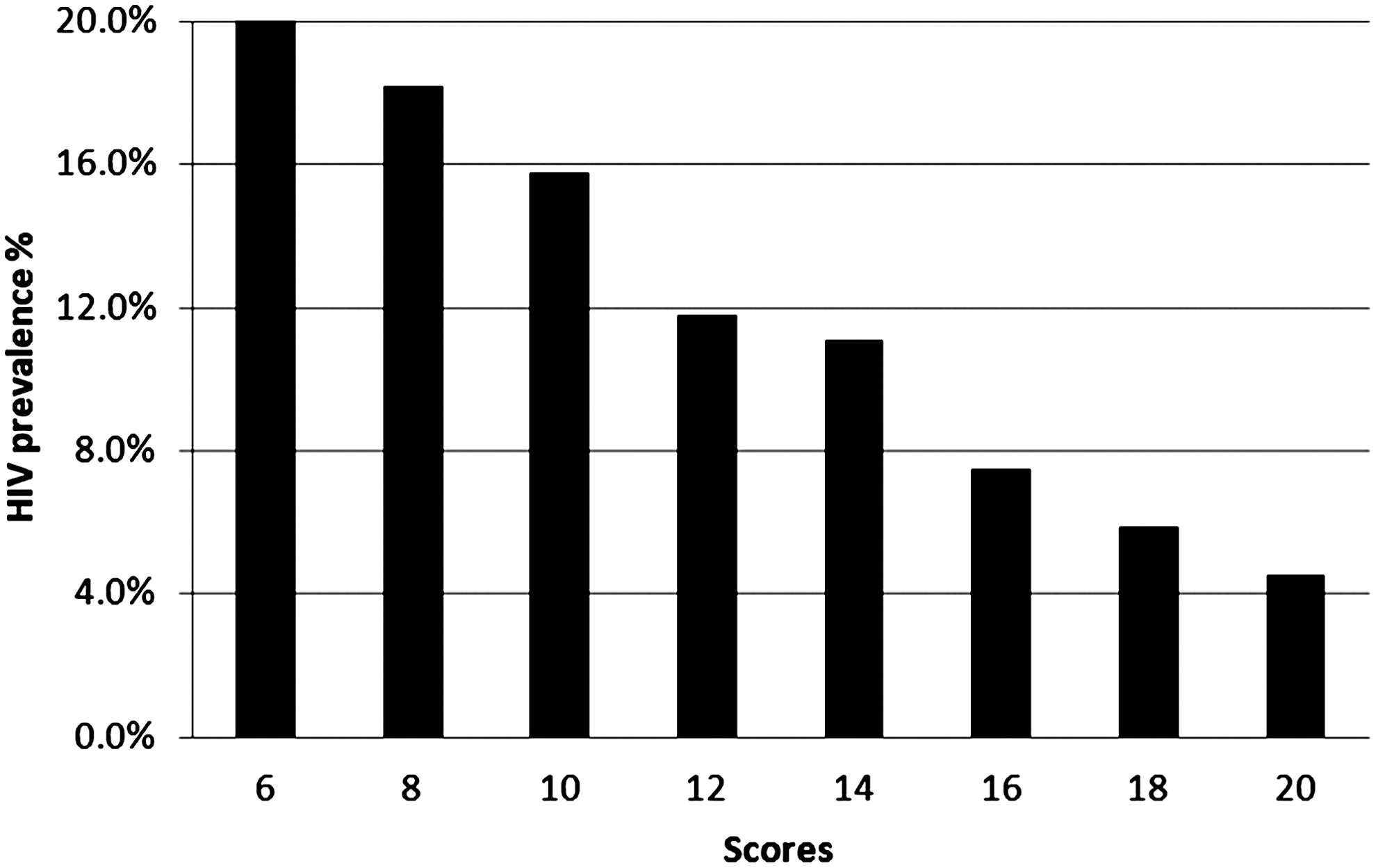
HIV prevalence among men who have sex with men (MSM) with condom use social norms scores in Beijing.
MSM, men who have sex with men; AOR, adjusted odds ratio; CI, confidence interval.
Discussion
Our 2009 survey found HIV prevalence among MSM in Beijing at 8.0%, continuing a progressive increase from 0.4% in 2004 to 5.8% in 2006 determined by previous surveys in Beijing using identical RDS methods. 22 HIV prevalence among MSM in Beijing is still rising. Our finding is consistent with China's current HIV prevalence trends due to increasing sexual transmission over the earlier predominant injection related mode, with high syphilis prevalence, and with homosexual transmission increasing rapidly in many major urban areas of the country. 2,9,46 In our survey, only about half (51.4%) of participants had ever tested for HIV. Although this was higher than previous surveys conducted in Beijing, it was still lower than in Western countries. 23 –26 Awareness of one's HIV-positive status has been a key to preventing onward HIV transmission among MSM from the perspectives of changing behavior after testing and prevention with positives interventions. 27 Moreover, identifying HIV-infected MSM is a necessary first step in linking them to HIV care for the benefits to their own health and also for the potential of lowering viral loads and therefore infectivity through anti-retroviral treatment. 15 We also found in our survey that only a minority (22.8%) of MSM knew the serostatus of their most recent partner and this lack of knowledge was associated with being HIV-infected. These low levels of knowing one's own serostatus and even lower levels of knowing one's partners' serostatus speak to difficulty of achieving a level of “serosorting” or “seroadaption” as measured among MSM in the West. 12,14,28 –32 Therefore, the multiple health and preventive benefits of HIV testing and serostatus disclosure have not been realized for MSM in China.
Our study is also the first to show that HIV prevalence was strongly associated with condom use social norms among Chinese MSM. Given the strong correlation we found between a preventive effect and increasing score, interventions to change social norms around condom use may affect sexual behavior among MSM when using condoms. 33,34 Interventions of this type might utilize peer based health education and counseling. 47,48 In addition, our finding also showed that persons buying condoms in the past 12 months had a lower HIV prevalence compare to those who never bought condoms. Our study and the previous studies among Chinese MSM showed high proportion of unprotected sex with male and female. 4,35,36 Therefore condom promotion and distribution may both be effective in preventing sexually acquired HIV infection in China.
Two findings bear further examination. In bivariate analysis, having female partners and being in Beijing less than 1 year were associated with higher HIV prevalence. The former finding was also held significance in the multivariate analysis. The relationship between having female partners, sexual orientation and identity, and is likely to be complex and may be rapidly changing with respect to HIV risk in China. 37 –40 Although evidence is not likely to prove that having sex with a woman would be of higher risk of acquiring HIV than with another MSM, particularly given the prevalence of HIV among other populations of women in China, there is the concern of HIV transmission to women and other sexual networks. 41,42 In the Chinese context, due to marriage, family, parenthood and other traditional concepts, many MSM had to get married with homosexual orientation, so they may both have sex with men and with women who are their wives and often the mother of their child. 43,44 A comprehensive HIV control strategy for MSM should also pay attention to prevent HIV transmission to women and children.
This study was subject to several limitations. First, there are limitations to RDS that have been previously noted. 45 For example, seeds for RDS recruitment are purposefully selected and do not guarantee the inclusion of all networks of MSM. Beijing is a particularly large city and RDS may not be able to reach across all geographic areas and across all networks. Second, we recognize that, although data were collected by CAPI, some high-risk behaviors and self-reported HIV status may have been underreported due to discrimination or stigma, leading to potential underestimation of prevalence and associations with these variables and HIV infection. Third, the multivariate analysis was conducted by using exported weights for the dependent variable (HIV infection). However, standardized guidelines for RDS data multivariate analysis are still under development and require validation.
Conclusions
Our study showed that HIV continues in a phase of rapid growth among MSM in Beijing, yet at 8% there is still opportunity for prevention. Meanwhile, high proportion of MSM have sex with women and are not Beijing permanent residents. Our findings reinforce the need for a multidimensional approach to prevent further spread of HIV infection both among these men and to their heterosexual partners in Beijing, and to at-risk groups in other geographic areas. One area of strong appeal is to increase resources and efforts to make HIV testing opportunities more accessible and to reduce barriers to testing so that infected persons can learn their status and obtain appropriate medical care and prevention services.
Footnotes
Acknowledgments
Y.R., Y.X. was the PI for the study; S.F., H.L. was the lead author for the paper; Y.R., Y.X., X.H., H.F.R., W.M.F., J.S., W.M., and Y.J. contributed the design of the study; H.L., X.M., Y.S., X.H., C.L., and S.F. oversaw data collection at the study site; SF performed all the statistical analyses and all the authors contributed to the write up. All authors read and approved the final manuscript.
This study was supported by grants from the National Natural Science Foundation of China (81161120428), the National Institutes of Health (# R01 AI078933 and #5D43TW001035-13), the Ministry of Science and Technology of China (2012ZX10001-002) and Chinese State Key Laboratory for Infectious Disease Develop Grant (2011SKLID102).
Author Disclosure Statement
No competing financial interests exist.