
Abstract
Task shifting to community health workers (CHW) has received recognition. We examined the performance of community antiretroviral therapy and tuberculosis treatment supporters (CATTS) in scaling up antiretroviral therapy (ART) in Reach Out, a community-based ART program in Uganda. Retrospective data on home visits made by CATTS were analyzed to examine the CATTS ability to perform home visits to patients based on the model's standard procedures. Qualitative interviews conducted with 347 randomly selected patients and 47 CATTS explored their satisfaction with the model. The CATTS ability to follow-up with patients worsened from patients requiring daily, weekly, monthly, to three-monthly home visits. Only 26% and 15% of them correctly home visited patients with drug side effects and a missed clinic appointment, respectively. Additionally, 83% visited stable pre-ART and ART patients (96%) more frequently than required. Six hundred eighty of the 3650 (18%) patients were lost to follow-up (LTFU) during the study period. The mean number of patients LTFU per CATTS was 40.5. Male (p=0.005), worked for longer durations (p=0.02), and had lower education (p=0.005). An increased number of patients (p=0.01) were associated with increased LTFU. Ninety-two percent of the CATTS felt the model could be improved by reducing the workload. CATTS who were HIV positive, female, not residing in the same village as their patients, more educated, married, on ART, and spent less time with the patients were rated better by their patients. The Reach-Out CHW model is labor-intensive. Triaged home visits could improve performance and allow CATTS time to focus on patients requiring more intensive follow-up.
Introduction
A
Community-based care using peer workers could represent a high standard of care for chronic diseases by getting services closer to people and providing a support system within the community. 4 In 2006 the World Health Organization launched the “treat, train, and retain initiative.” 5 Task shifting is a key component of this initiative with the role of community health workers (CHW) to fill the HRH gaps receiving more recognition. 5,6 Several African countries have since invested in new cadres of CHWs, arguing that they preferentially reach those at high risk and the poor who are less likely to use health facilities. 7
Although CHW programs have improved access, coverage, and health outcomes, 8,9 large-scale CHW programs have also been hampered by lack of sustainability and poor quality of care. 10 –12 It is therefore timely to evaluate the capacity of community systems to cope with the task-shifting strategy without compromising potentially effective models.
This evaluation was done to assess the performance of CHWs labeled as community antiretroviral therapy and tuberculosis treatment supporters (CATTS) by Reach Out Mbuya HIV/AIDS Initiative (ROM). We draw lessons from ROM's experience in scaling up a peer-led community-based model while documenting how the model has responded to the increasing patient load. We also propose strategies to improve the model with reference to critical areas that are considered useful to support CHW models. 6,9 –11
Materials and Methods
Study setting
This evaluation is part of a larger study to evaluate ROM's model of care and focuses on the performance of CATTS. ROM provides comprehensive HIV services including antiretroviral therapy (ART) to the urban poor in Kampala, Uganda and has been fully described. 13
Thr peer-led approach at ROM
The model is structured to facilitate links between the community and the facility through a community network of care (CNC) as shown in Fig. 1. The CNC comprises CHWs with different roles. Community supporters, normally less educated, help the very sick patients with household chores. Community ART and tuberculosis (TB) treatment supporters (CATTS), mother to mother supporters (M2M), and adolescent supporters are the core of the model and carry out monitoring of patients at home based on daily feedback from the nurses and doctors. These are patients who have excelled in taking their own medication and in understanding the basic concepts of self-management of HIV (expert patients).
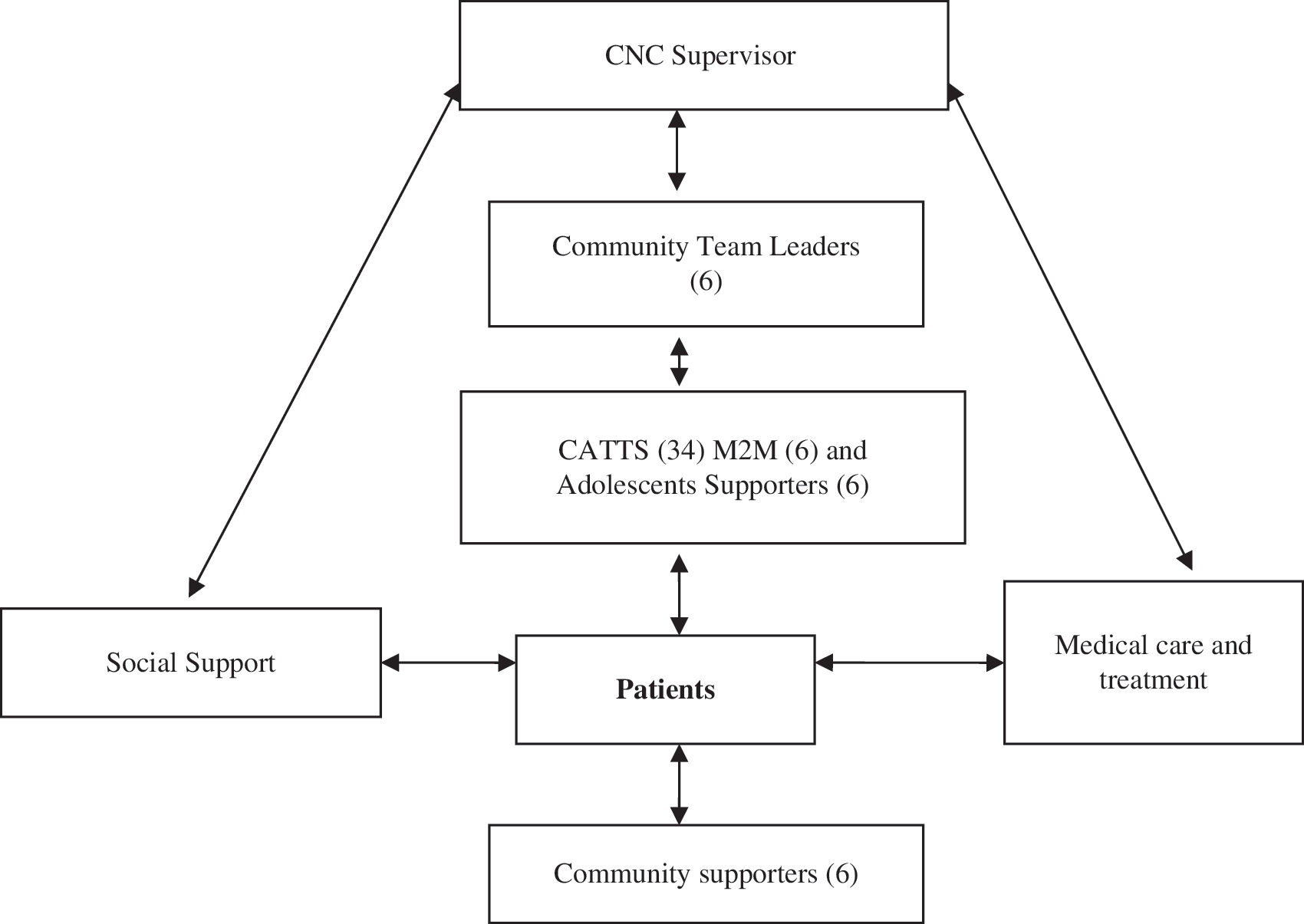
Structure of community network of care.
Each patient is attached to a CATTS staying within or closest to their community prior to enrolment. In 2002 each CATTS supported 5–10 patients but by 2008 each had 60–150 patients. The role of CATTS was initially to support patients for adherence to medication and to refer difficult cases for medical, psychosocial, or socioeconomic support. With the increasing number of pregnancies and the loss to follow-up of prevention of mother to child transmission of HIV (PMTCT) recipients and adolescents, one CATTS per community was trained in PMTCT or adolescent-specific activities and relabeled “Mother to Mother” (M2M) and “adolescent supporters,” respectively. In the context of this evaluation the CATTS, M2M, and adolescent supporters are all referred to as CATTS. They undertake a 3-week training in home-based care including basic counseling, medication adherence, TB and ART treatment, and drug side effects referral, and record keeping.
The CATTS are supervised by team leaders who each supervise 8–20 CATTS within their communities. The team leaders carry out verification of a sample of patients visited by the CATTS on a weekly basis to ensure proper record keeping and compliance with the model's current standard operating procedures. The team leaders are in turn supervised by a nurse who works alongside a coordinator to ensure that the CNC is responsive to the patients needs.
Members of the CNC hold weekly meetings to discuss their patients. The meetings are scheduled to coincide with the clinic day for that community, which enhances consultations and referrals between CNC and the medical team. Lists of patients requiring intensive home visits including those with an acute illness, drug side effects, and poor medication adherence are generated by the clinicians and given to the CATTS who provide a daily feedback on the patients' health status until their condition stabilizes. Additionally, the patients undertake health education about side effects of drugs so that they can notify the CATTS immediately. Monthly meetings bring together all members of staff and serve as a forum for feedback on community activities.
Initially the CATTS roles focused on using their personal experience. However, by 2007 they received job descriptions with defined roles. The team leaders and CATTS earn USD 310 and 100 per month, respectively. In addition, they receive incentives including free care and treatment, school fees support for their children, nutrition support, bicycles, raincoats, umbrellas, interest-free loans, and participate in various income-generating activities. Between 2002 and 2009 only 2 CATTS had resigned for better pay while 3 had died.
Evaluation procedures
Quantitative and qualitative data were used to evaluate the CATTS performance against the models current standard operating procedures
Ability of CATTS to carry out home visits
We extracted and reviewed retrospective data for August 2007 to October 2009 on home visits made by the CATTS. The CATTS standard home visit operating procedures (Table 1) require that patients be visited for three main purposes broadly categorized as: (1) to ensure adherence to medication and retention; (2) make appropriate and timely referrals; and (3) to ensure appropriate follow-up of patients. The frequency and scheduling of home visits based on the patients' needs determines the caseload and efficiency of the home visits. If the CATTS visit the stable patients more frequently then they will probably compromise the intensity of follow-up required for the more sick patients. The number of patients home visited by each CATTS over the study period was compared with the actual numbers they were expected to visit based on the patients health status to assess their performance. The number of patients lost to follow-up (defined as having not shown up for 3 months after a scheduled clinic appointment) by each CATTS was also extracted from electronic records and evaluated
CATTS, community antiretroviral therapy and tuberculosis treatment supporters; ART, antiretroviral therapy; TB, tuberculosis.
Qualitative interviews
Interview data were collected from 347 randomly selected patients and all 46 CATTS. Semistructured interviews explored the patient's views on the home visits by CATTS. In-depth interviews with CATTS explored their perceptions and satisfaction with the current model of care. Study instruments were pretested and the in-depth interviews tape recorded (with consent) and transcribed into English. During the data collection phase debriefing meetings were held at the end of each day to ensure good quality data and share new emerging issues. Expanded notes were prepared to capture what transpired during the interviews.
Data analysis
Quantitative data analysis
Data were analyzed using STATA, version 11 (StataCorp, College Station, TX). Characteristics of the CATTS were described using medians and interquartile range (IQR) for continuous variables and counts and percentages for categorical variables. Bivariate comparisons were done using χ2 test for categorical variables while the Student's t test and Wilcoxon rank sum test were used for comparing data with normal and non-normal distributions respectively. We analyzed retrospective data on home visits made by CATTS and compared these against the model standard operating procedures as shown in Table 1. Home visits correctly carried out were coded as 1 or 0 if otherwise. The percentage of CATTS who carried out home visits correctly was determined while exploring for characteristics that optimizes their ability to adhere to the model standards. In a bivariate analysis, proportion of home visits correctly carried out for each CATTS was calculated as a weighted sum of all the home visits to obtain scores for each of the CATTS. A type of home visit was considered to be correctly done if for at least 95% of the patients the CATTS had correctly carried out the activity. In addition, variance between number of patients reported as supported by the CATTS and the actual numbers obtained from records was assessed. The number of patients lost to follow-up per CATTS was assessed against CATTS characteristics. Association between scores and the dichotomous variables was tested using the Student's t test while that between scores and other categorical variables was tested using one-way analysis of variance (ANOVA). p Values and 95% confidence intervals were all two-sided and significance level was denoted as p=0.05 or less.
Qualitative data analysis
In-depth interviews were recorded and transcribed verbatim. Transcripts were anonymous analysis was performed by using theme and content using standard qualitative methods. 14 –16 Codes were created to label all information that informed the research questions, which were then organized into themes and subthemes with themes categorized as efficiency or quality. “Representative quotes” were selected to illustrate the identified themes. The study was approved by the Makerere University School of Public Health Institutional Review Board and the Uganda National Council of Science and Technology.
Results
The characteristics of the CATTS and patients are shown in Table 2. Overall, the CATTS are similar to the patient population from which they are drawn but are significantly more educated, older, and are better adherent to medication.
CATTS, community antiretroviral therapy and tuberculosis treatment supporters; ART, antiretroviral therapy; TB, tuberculosis.
Performance of CATTS in carrying out home visits
The number of CATTS doubled from 24 in 2004 to 46 in 2009 while the number of home visits increased from 12,648 to 36,227 (36% increase). The median total number of patients/CATTS during the study period was 67 (range, 21–132). The variance between the number of patients who were home visited by the CATTS during the study period against the number who should have home visits increased with the number of patients under their care (data not shown)
Only 26% of the CATTS correctly followed up patients with drug side effects, only 63% correctly followed up poorly adherent patients and almost none correctly followed up pregnant mothers (Table 1). Stable patients who could be visited less frequently or not at all were visited on a monthly basis and in some cases even more frequently. Majority of the CATTS (42/46) mentioned that they should visit their patients based on their health status need but that the workload and other challenges hindered them from doing so: “Patients change their homes without informing me. I have 75 patients and even if I make a home-visit schedule some patients get acute illnesses, side effects or miss appointments so I have to reschedule my work and the patients who were on my days schedule end up missing their home visit” (female CATTS).
The majority of the CATTS visited their patients to review adherence and ensure retention as shown in Table 1. “I count my patient's pills and check to ensure the ART card is well ticked. If the patient is not taking the pills I advise them on the consequences of poor adherence” (male CATTS).
However, only 15% of the CATTS had actively traced patients who could have been lost to follow-up and only 46% of them had engaged family members in offering support to the patients: “Some of my patients have not disclosed their HIV status and they prefer that I do not visit them at home but rather meet them anywhere else in the community for follow-up” (female CATTS).
The total number of patients lost to follow-up during the study period was 680 of 3650 (18%) of the patients. The mean number of patients lost to follow up per CATTS was 40.5 standard deviation (SD) 29.5. Although age, length of service, and category of CATTS were significantly associated with LTFU in unadjusted analysis (Table 3), they were not significant in the regression model. In a regression model (Table 4), CATTS of male gender (p=0.005), those who had served for more than 6 years (p=0.02), and who received adult literacy (p=0.005) lost more patients. An increasing number of patients supported was also associated with increased loss to follow-up (p=0.01).
The p values are from t test for binary variables and from analysis of variance (ANOVA) for categorical variables.
CATTS, community antiretroviral therapy and tuberculosis treatment supporters; M2M, mother to mother supporters; IGA, income generating activities.
CATTS, community antiretroviral therapy and tuberculosis treatment supporters; CI, confidence interval; LTFU, lost to follow-up.
Patient's perceptions of the CATTS performance are shown in Table 5. Nearly all patients (98%) knew of the presence of CATTS in their communities and the work done by the CATTS was largely seen as satisfactory (87%). Married, female, more educated CATTS who were living with HIV and on ART were more appreciated by the patients. The patients revealed that there was a very close and continuous follow-up by the CATTS that guaranteed adherence support, “I get good counseling on adherence in a way that I don't lose hope. The CATTS encourage me” (female patient). The patients further complimented the referral services by the CATTS for being timely. “I had just started ARVs and got an itchy skin rash, my CATTS called the nurses and they immediately stopped the drugs and sent me to the health centre” (male patient).
CATTS, community antiretroviral therapy and tuberculosis treatment supporters.
CATTS who spend less time with the patients during the home visits were also better appreciated: “I have work to do and I would prefer if my CATTS focused on my problems and then leaves so I can continue my errands” (male patient). The most common challenges mentioned by the patients included long home visiting times (17%) and too frequent home visits (37%).
CATTS' perception of the model
The CATTS mentioned the intensive follow-up schedule (87%), patient movements (40%), missed appointments (10%), and nondisclosure of HIV status (27%) as their main challenges. Regarding their perception of the current model, 65% of the CATTS said it was good, 25% said it was excellent, and 10% said it was poor. The CATTS felt that the system could be improved by reducing workload (92%), improved logistics (42%), better remuneration (25%), and more training 20%.
Discussion
Reach Out's community, peer-led model represents a promising strategy to the HRH crisis. The majority of the CATTS are PLWHA and they were rated significantly better than their non-HIV–positive counterparts by the patients. The use of experiences of PLWHA is an important concept for long-term care, but has not been utilized in many CHW programs 17,21 and ROM's experience reaffirms that PLWHA are better suited to understand and respond to the needs of their peers.
Delegation of tasks from health professionals to CHWs has been found to have a positive impact on health outcomes, is acceptable to the patients, and potentially more affordable. 18 –20 However, confusing terminology has been used to describe various types of nonprofessional health workers. 21 The World Health Organization (WHO) defines a CHW as a member of the community that they serve, someone who has limited training compared to health professionals, and receives support from the health care system without necessarily being a part of it. 21 CATTS follow patients who reside within the same communities as they do, bringing services closer to people who otherwise could not access them. This also allows CATTS to be intimately involved in their patients' lives. They are able to check up on them consistently. Notably, the CATTS are able to look past a façade that some patients may put on when they go to a health facility. However, in our study patients rated CATTS who reside within their communities and spend longer time during home visits significantly poorer. We speculate that this could be as a result of stigma, non-HIV status disclosure, or poor CATTS attitudes. In addition many patients have stabilized and have returned to normal life and frequent visits by the CATTS may interfere with their lives and daily routine. Negative attitudes of health workers have been shown to significantly reduce adherence and retention of patients. 8,11 The ROM peer model enforces the need for a strong relationship between provider and patients that have been built over time. However, the median duration of service of the CATTS was 4.5 years and their attitudes could have changed over time leading to loss of trust by the community. This calls for ongoing assessment of the CATTS' performance and attitudes in the community. The majority of the CATTS refer their patients in a timely manner, which may be attributable to the close geographical proximity between the patients and their CATTS as well as close interaction between the CATTS and the medical teams.
“Expert patients” are found in many ART clinics in Uganda but characteristics of their recruitment, remuneration, training, and roles are determined by the respective clinics with their level of resources. Salaries range from USD 2 to USD 75 per month. 22,23 This fragmentation will affect scale-up of such models and calls for a national regulatory framework. Our study provides some understanding into the motivation and incentives that maintained commitment of the CATTS. Nonfinancial benefits, in addition to training and a salary, contributed to the high retention of CATTS. In addition, the CNC is a well-organized supervisory system with the potential to increase motivation and provide professional development.
ROM, like many other programs, 13,26 is experiencing a decline in patient retention yet CATTS are better placed to actively trace defaulting patients. This is because the CATTS have a wide range of activities, high patient loads, and a follow-up model that is labor-intensive in nature, which makes them inefficient in responding to the health needs of their patients. This highlights the need for robust and simplified treatment algorithms that take into consideration the chronicity of HIV and improves decision making at the community level without compromising quality of care. Obstacles cited by the CATTS were similar to those cited by similar studies 27 and include the increasing workload and the need for better remuneration. Insufficient training and lack of logistical support were also mentioned.
Our findings should be interpreted with caution considering that ROM serves a defined catchment area making patient follow-up easy and cost-effective, which may not be the case for other ART scale-up programs. Additionally, routine program data, with its inherent challenges, were used in this evaluation.
ROM's peer-led CHW model represents a promising strategy to the health systems challenges in Africa. However, if it is to be scaled up, a less labor-intensive long-term care paradigm that ensures lifetime provider commitment is required. Improvement in triage will improve efficiency and will allow CATTS to focus on patients requiring intensive follow-up while allowing stable ones to adopt a self-management care model. Protocols and standardized simplified guidelines that identify patients most in need and integrate the community systems into a strengthened monitoring and evaluation system need to be devised. Above all, community health systems strengthening should be integrated into the broader health systems strengthening strategies if we are to maximize the potential of shifting tasks to community health workers.
Footnotes
Author Disclosure Statement
No competing financial interests exist.