
Abstract
We report the case of a 59-year-old man who moved from Cape Verde to Massachusetts at the age of 29. He had multiple sexual contacts with female partners in Cape Verde and with West African women in Massachusetts, as well as multiple past indeterminate HIV-1 antibody tests. He presented to our facility with 2–3 months of inappropriate behaviors, memory impairment, weight loss, and night sweats, at which time he was found to have an abnormal enhancing lesion of the corpus collosum on brain magnetic resonance imaging (MRI). Laboratory testing revealed a CD4 count of 63 cells/mm3, positive HIV-2 Western blot, serum HIV-2 RNA polymerase chain reaction (PCR) of 1160 copies per milliliter and cerebrospinal fluid (CSF) HIV-2 RNA PCR of 2730 copies per milliliter. Brain biopsy demonstrated syncytial giant cells centered around small blood vessels and accompanied by microglia, which correlated with prior pathologic descriptions of HIV-2 encephalitis and with well-described findings of HIV-1 encephalitis. Based on genotype resistance assay results, treatment guidelines, and prior studies validating success with lopinavir-ritonavir, he was treated with tenofovir-emtricitabine and lopinavir-ritonavir, which has led to virologic suppression along with steady neurologic and radiologic improvement, although he continues to have deficits.
Introduction
O
Case Report
A 59-year-old right-handed man presented with 2–3 months of inappropriate behaviors and progressive memory impairment. Review of systems revealed unintentional weight loss and night sweats without fever. He had a history of indeterminate HIV antibody testing in the past, a prior episode of proctitis, and a remote history of small bowel resection for obstruction. The patient moved to Massachusetts from Cape Verde at age 29 and had not traveled back to Cape Verde since that time. He reported sexual contact with female partners while living in Cape Verde and with women from Cape Verde after moving to Massachusetts. General physical examination was notable for oral candidiasis. On neurologic examination, the patient was distractable and disoriented with markedly tangential speech. He demonstrated impairment in attention, concentration, and motivation, as well as registration and recall tasks; grasp and palmomental reflexes were present on the right. Language was fluent and visuospatial skills and praxis were intact. Cranial nerves, strength, sensation, coordination, and gait testing were normal.
Laboratory studies revealed white blood cell count 3.81×103 cells/μL, hemoglobin 12.3 g/dL, and albumin 3.4 g/dL. T2-weighted magnetic resonance imaging (MRI) demonstrated a confluent area of signal abnormality within the anterior corpus callosum extending into the right-greater-than-left frontal subcortical white matter with no significant mass effect (Fig. 1A). T1-weighted images following intravenous administration of gadolinium showed abnormal enhancement within the region of T2 signal abnormality (Fig. 1B–F). The callosal lesion showed no reduced or elevated diffusivity. There was no meningeal enhancement.
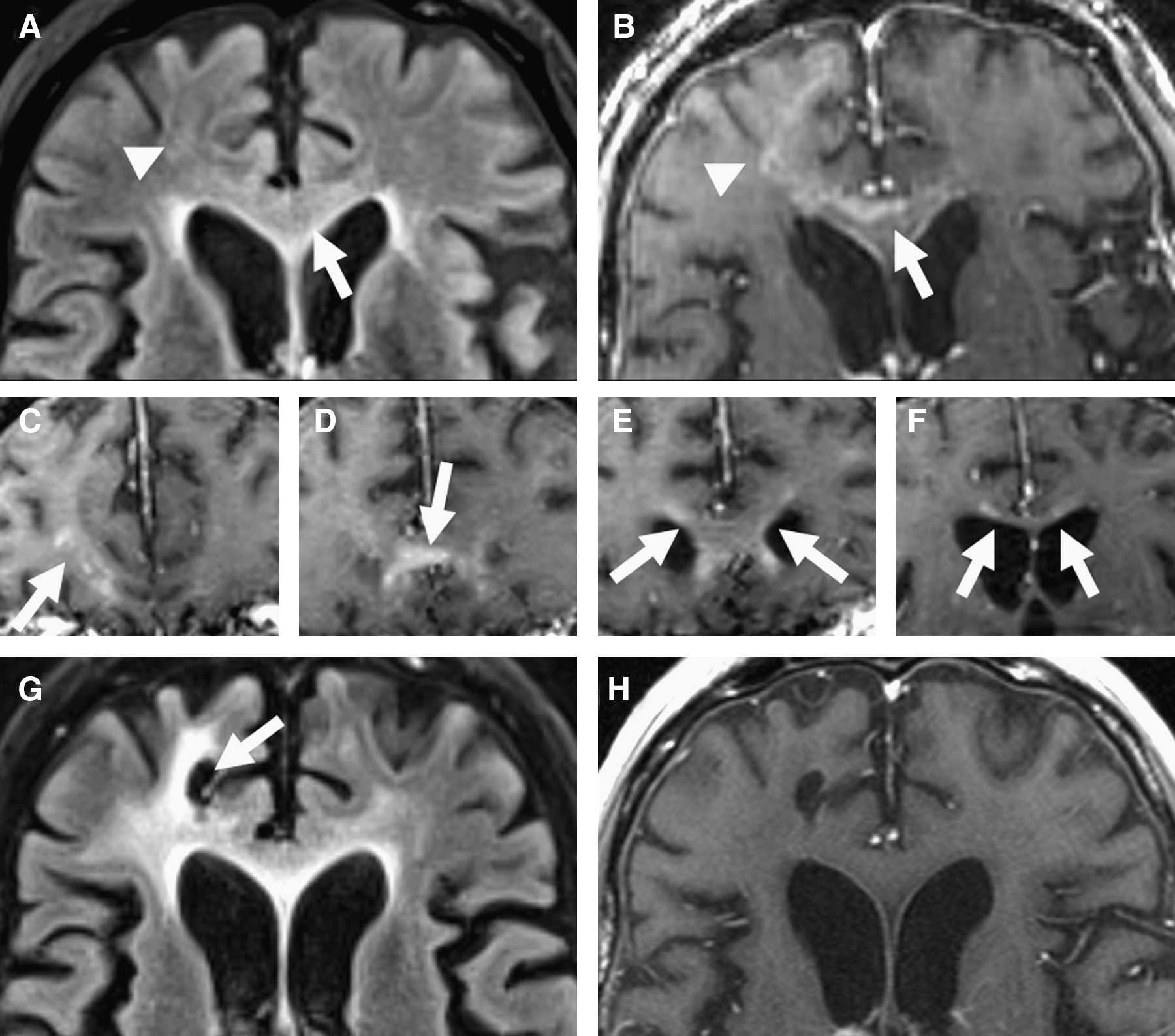
Axial T2-weighted fluid-attenuated inversion recovery (FLAIR) images reveal abnormal hyperintense signal within the genu of the corpus callosum (
Lumbar puncture yielded clear cerebrospinal fluid (CSF) with glucose 51 mg/dL, protein 68.1 mg/dL, red cell count 3 cells per microliter, and white cell count 1 cell per microliter. Studies of the CSF that were negative included: gram stain and culture, Venereal Disease Research Laboratory (VDRL), and polymerase chain reaction (PCR) for herpes simplex virus, Epstein-Barr virus, John Cunningham (JC) virus, and human herpesvirus 6. Cytology, gene-rearrangement studies, and flow cytometry of the CSF showed no evidence of malignancy. Blood tests for cryptococcal antigen and antinuclear antibody were negative. Serum treponemal antibody and Treponema pallidum particle agglutination assay were positive; rapid plasma reagin was nonreactive. Nonspecific enzyme-linked immunosorbent assay (ELISA) of the blood for antibody against HIV (types 1 and 2) was positive. Western blot for antibody against HIV-1 was indeterminate, with strong band at p31 and weak bands at p24 and p40. No HIV-1 RNA was detected by plasma PCR. HIV-2 specific Western blot was positive (Focus Diagnostics, Inc., Cypress, CA). CD4 cell count was 63 cells/mm3 (5% of the total lymphocyte count). Plasma viral load was 1160 copies per milliliter and CSF viral load was 2730 copies per milliliter by previously described quantitative HIV-2 PCR testing methods. 5
A stereotactic biopsy of the right frontal subcortical white matter was performed due to suspicion of lymphoma or other infiltrating neoplasm. Pathologic evaluation of the biopsy specimen revealed syncytial giant cells primarily centered around small blood vessels and focally accompanied by microglia, most consistent with HIV encephalitis (Fig. 2). Immunohistochemical stain for CD163 (activated macrophages) revealed the lesion to be composed entirely of macrophages and active microglia without evidence of other inflammatory cells.
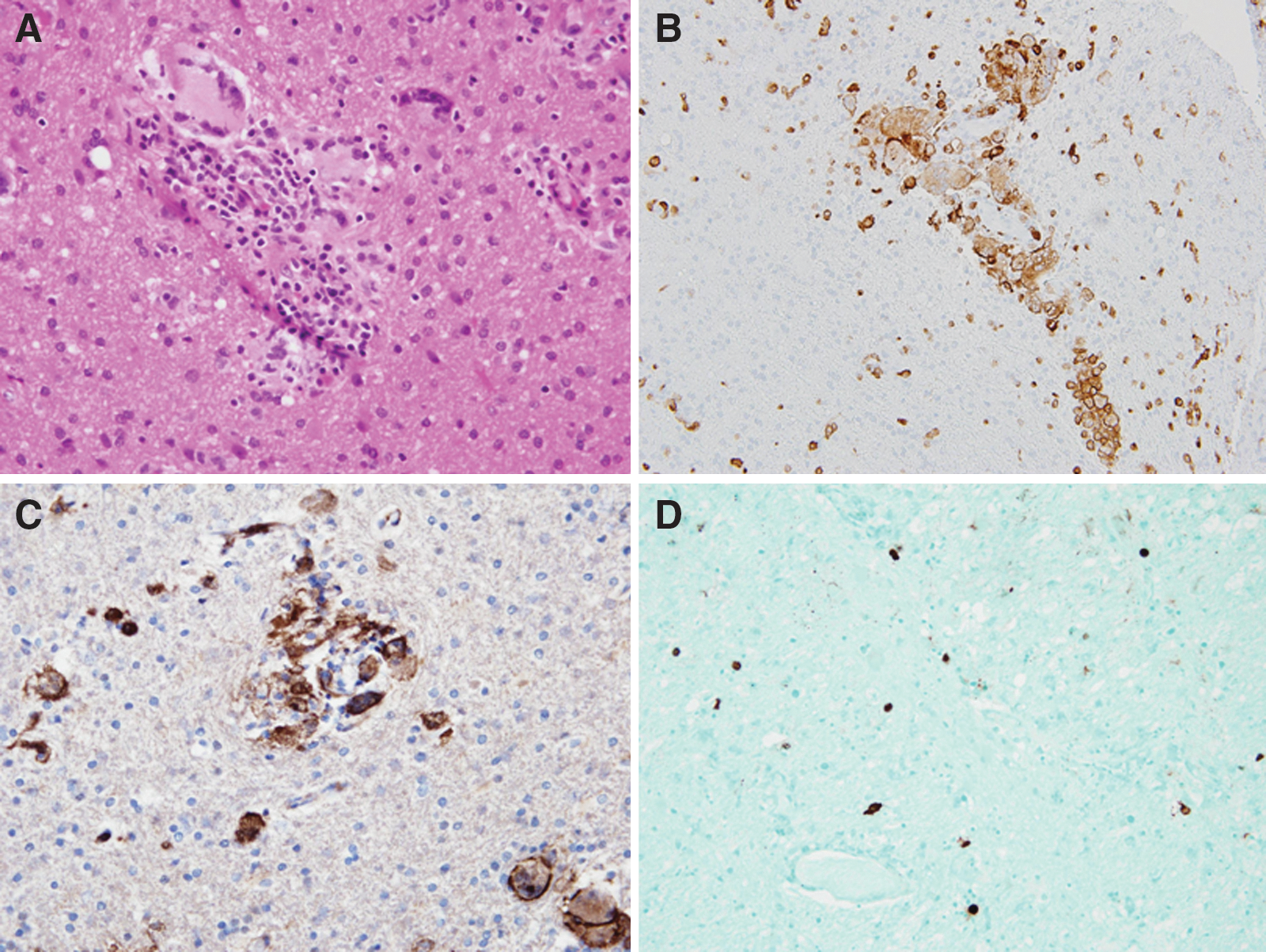
Histologic images from the brain biopsy performed in this patient are shown. A hemotoxylin and eosin stained section (400×magnification) demonstrates the presence of macrophages, giant cells, and a microglial nodule which were the only abnormalities found in the tissue (
Immunohistochemical stain for HIV-1/2 p24 antigen was performed and most intensely stained within macrophages and syncytial cells. Immunohistochemistry for JC virus was positive in rare scattered cells.
Antiretroviral therapy was initiated with tenofovir-emtricitabine and lopinavir-ritonavir. The patient also received empiric intravenous penicillin for possible neurosyphilis. Genotype assays of the serum and CSF isolates (done by previously described HIV-2 genotype resistance assay methods) later demonstrated non-nucleoside reverse transcriptase inhibitor resistance and reduced protease inhibitor susceptibility. 6 Repeat plasma testing after one month of antiretroviral therapy demonstrated undetectable HIV-2 RNA (<100 copies per milliliter). 5 Three months after beginning therapy, brain MRI demonstrated an interval increase in abnormal T2 hyperintensity throughout the right greater than left frontal subcortical white matter with resolution of the abnormal enhancement in this region (Fig. 1G and H). These changes were felt to represent resolution of active inflammation and persistence of encephalomalacia from prior inflammation. Four months into treatment, his CD4 cell count had increased to 183 cells/mm3 and cognition had modestly improved, but deficits in memory and executive function persisted. Neurologic examination was notable for continued impaired attention, perseveration on clock drawing, and the presence of utilization behavior and frontal release signs with intact language, calculations, and visuospatial skills.
Discussion
Central nervous system (CNS) complications of HIV-1 infection have been well described and neuropathologic abnormalities have been found at autopsy in as many as 80-90% of HIV-1–infected patients. 7 Neurologic disease associated with HIV-2 is less well understood; reports are uncommon and often limited to opportunistic infections. 4,7 Descriptions of HIV-2 encephalitis are especially unusual. Our patient was evaluated for other CNS infections, autoimmune processes, vasculitides, and malignancies but none were found. Imaging characteristics, negative CSF VDRL, and pathology from brain biopsy made it unlikely that the cause of his symptoms was neurosyphilis, despite positive serum treponemal antibodies. Brain biopsy did reveal scattered glial nuclear positivity with antibody to polyoma virus (which recognizes JC, BK, or SV40 virus proteins), but the paucity of positively stained cells, lack of demyelination, and negative CSF JC virus PCR made progressive multifocal leukoencephalopathy (PML) extremely unlikely. Antibody positivity may relate to focal incidental activation or latency rather than active disease, as latent JC virus has been shown to exist in the brains of individuals without PML. 8
To our knowledge, this is the first reported case of HIV-2 encephalitis diagnosed by brain biopsy in a living patient. The histopathology of HIV-2 encephalitis was described in a 2003 case series in which brain specimens from eight patients were reviewed at autopsy (six HIV-2 infected and two HIV-1/HIV-2 dually infected). 9 HIV-2 p26 was detected in brain tissue in four of the HIV-2 cases and one of the dually infected using immunohistochemistry. The productively infected cells were either microglia or infiltrating macrophages. The pathology of our patient was comparable to that described in this report and was also similar to that of HIV-1 encephalitis, which typically involves collections of multinucleated giant cells, microglial nodules, and macrophage aggregates around small blood vessels in the central white matter. 10
Two prior case reports describe patients with HIV-2 encephalitis confirmed by pathology at autopsy. 7,11 First, a 27-year-old Senegalese woman was diagnosed with HIV-2 in the setting of Pneumocystis jirovecii pneumonia and suppressed CD4 count and subsequently developed CMV and Toxoplasma retinitis that resolved with treatment. She then developed progressive cognitive decline, depression, and aggression with cortical atrophy on computed tomography, and no other CNS infection was identified. Histopathology on autopsy demonstrated changes consistent with HIV-2 encephalitis and HIV-2 was detected in brain tissue by immunohistology, PCR and in situ hybridization. Second, a 31-year-old Portuguese woman developed diplopia and photophobia followed by fever, malaise, and gait instability then forgetfulness and hallucinations. She was found to have an enhancing right parietal mass and seropositivity for HIV-2 infection and later died. Autopsy demonstrated multiple abscesses (including the right parietal lobe) with Toxoplasma bradyzoites and tachyzoites. Additionally, microglial nodules, multinucleated giant cells, and perivascular mononuclear cell infiltration were seen diffusely throughout the subcortical white matter, basal ganglia, and brainstem.
Very few studies have compared rates of encephalitis caused by HIV-2 infection to HIV-1. In one Cote D'Ivoire study that included autopsies of HIV-1–positive, HIV-2–positive, and HIV-negative patients, encephalitis secondary to HIV-2 appeared to be more common: 7 of 40 patients with HIV-2 (18%) had multinucleated giant cell encephalitis compared to 1 of 174 patients with HIV-1 (1%). 12 Other comparisons have found equivalent rates of encephalitis between HIV-1 and HIV-2 but did not establish whether HIV directly caused the encephalitis. 13 Based on these limited data and rare case reports, it is difficult to compare the relative neurotropism of HIV-1 and HIV-2.
Optimal treatment for HIV-2 infection is less clearly defined than for HIV-1 and is hindered by lack of randomized clinical trial data and no commercially available viral load or resistance assays (our viral load and resistance tests were performed by a research laboratory). In terms of antiretroviral therapy, most guidelines and experts recommend two NRTI's along with a ritonavir-boosted PI; HIV-2 is known to be intrinsically resistant to NNRTI's. 1 Genotype resistance testing for our patient demonstrated high-level resistance to nevirapine, efavirenz, fosamprenavir and nelfinavir. One study demonstrated positive response at 2 years in 29 HIV-2–infected patients taking regimens with lopinavir-ritonavir, which led us to choose this agent. 14 Our patient responded well to tenofovir-emtricitabine plus lopinavir-ritonavir, with virologic suppression, immunologic recovery, radiologic improvement, and slow clinical improvement, although he remains far from his baseline.
Another important aspect of the case is that the patient had a history of prior indeterminate HIV-1 antibody tests but had never been tested for HIV-2. It is important to remember that routine ELISA tests at most institutions do not differentiate between HIV-1 and HIV-2 and reflexive Western blots are specific to HIV-1. The CDC recommends checking specific HIV-2 tests for the following persons: sex partners of a person from a country where HIV-2 is endemic, sex partners of a person known to be infected with HIV-2, persons who received a blood transfusion or nonsterile injection or shared needles in an endemic country, children of women with risk factors for HIV-2 or known to be infected with HIV-2, or when there is suspicion for active HIV disease with an HIV-1 Western blot that is negative or results in an unusual pattern. With HIV-2 infection, the HIV-1 Western blot often shows an indeterminate pattern with GAG bands and POL bands but no ENV bands. 15 Studies have shown that African immigrants in the United States are unlikely to seek routine HIV testing (only 4% diagnosed by routine testing in one study), commonly present with late-stage HIV disease, and are frequently infected with non-subtype B strains. 16 This underscores the need for careful consideration of infection in at-risk patients.
In conclusion, neurologic disease attributable to HIV-2 infection is not well described in the literature and the limited accessibility of diagnostics and treatment data makes it a challenging clinical illness. It is essential to consider HIV-2 as a possible cause of infection in patients from at-risk countries or with indeterminate HIV antibody results. It is also important to remember that while most often a protracted and mild illness, HIV-2 can sometimes progress to severe disease and significant neurologic impairment as in the case presented.
Footnotes
Acknowledgments
HIV-2 RNA PCR and genotype testing performed at the ISO/IEC 15189:2007 accredited diagnostic laboratory of the Erasmus MC, Department of Virology. HIV-1/2 p24 antibody was a kind donation of Dr. Dana Gabuzda and immunohistochemistry was performed by the laboratory of Dr. Geraldine Pinkus. We would like to extend special thanks to Dr. Umberto de Girolami for assistance with the pathology in this case.
Author Disclosure Statement
No competing financial interests exist.