
Abstract
Mood disorders are more frequent among people with HIV infection than among non-HIV–infected individuals of the same age, socioeconomic status, and HIV risks. They have been associated with worse adherence and clinical outcomes, yet remain underdiagnosed and undertreated in sub-Saharan Africa. We explored the relationship between mood disorders using the 10-item depression scale of the Centers for Epidemiological Studies (CES-D10) and the 22-item Impact of Events Scale-Revised (IES-R) for posttraumatic stress disorder, and a range of demographic and HIV-related variables among 252 consecutive subjects on antiretroviral therapy (ART). The study was conducted in the Genito-Urinary Medicine Clinic of the Medical Research Council's Gambia Unit. These screening tests were positive in 7% and 30%, respectively, of the patients, with higher scores (more depression or more post-traumatic stress) associated with female gender, more advanced WHO clinical stage, and lower Karnofsky Perfomance Scale rating. Higher CES-D10 scores were also seen among those on their second ART regimen. No relationship was seen with age, time on ART, viral load, or CD4 cell count. Compared to an earlier study at the same site in subjects prior to starting ART, the prevalence of depression in those stabilized on ART was dramatically reduced (by 34%, from 41%) while that of PTSD dropped less (by 13%, from 43%). Integrating the CES-D10 or a similar instrument into patient preparation for ART is recommended in order to identify those who may benefit from further mental health investigations, specific therapy, or closer follow-up during early ART.
Introduction
In general mood disorders have not been well-researched in sub-Saharan Africa. 23 Depression in sub-Saharan Africa has been associated with female gender, older age, disability, low CD4 cell count, difficulty affording ART and not having an independent income. 14,24 –28 Depression is also a known side effect of the antiretroviral (ARV) medicine efavirenz (EFV). 29 PTSD in sub-Saharan Africa has been associated with female gender, disability, and not having an independent income, as well as alcohol consumption and being unmarried. 14,24,26 In addition, several studies have found a relationship between mood disorders and CD4 cell count in sub-Saharan Africa. 25,26,30,31 In an earlier study of the prevalence of depression and PTSD among patients with a CD4 cell count over 200 cells per microliter that had not yet started pre-ART counseling, in the same clinic and using the same instruments as the current study, the prevalence of positive screening tests was 41% for depression and 43% for PTSD, in line with the range of values reported in untreated patients with HIV infection. 26
Screening questionnaires exist for both depression and PTSD. The additional value of these types of short screening instruments in HIV care is that they may provide a simple mechanism for identifying a subset of patients at higher than normal risk for adherence difficulties. Identifying these patients allows additional staff time and other resources to be targeted to them, potentially reducing their risk of subsequent treatment failure.
Being treated with ART, 32,33 even receiving pre-ART counseling 4 or being in care and medically stable without the benefit of ART, 24 appears to have a positive impact on mood disorders. In the current study we sought to establish the prevalence of positive screening tests for depression and PTSD among patients stabilized on ART.
Methods
Participants and procedures
The study was conducted at the Genito-Urinary Medicine (GUM) Clinic at the Gambia Unit of the Medical Research Council. HIV-infected individuals had been enrolled as part of an ongoing study cohort prior to the implementation of ART starting in October 2004. The clinical cohort is described in more detail elsewhere. 34 Two hundred fifty-two essentially consecutive adult patients on ART were enrolled into the study from February to May 2010 during routine clinic visits. One hundred thirty-five patients attending the clinic during the trial period were not offered enrollment, primarily because of interruptions in the availability of study forms. Intermittent medical assistant staffing shortages and patients requiring urgent medical care further contributed. All those asked to participate consented.
Questionnaires
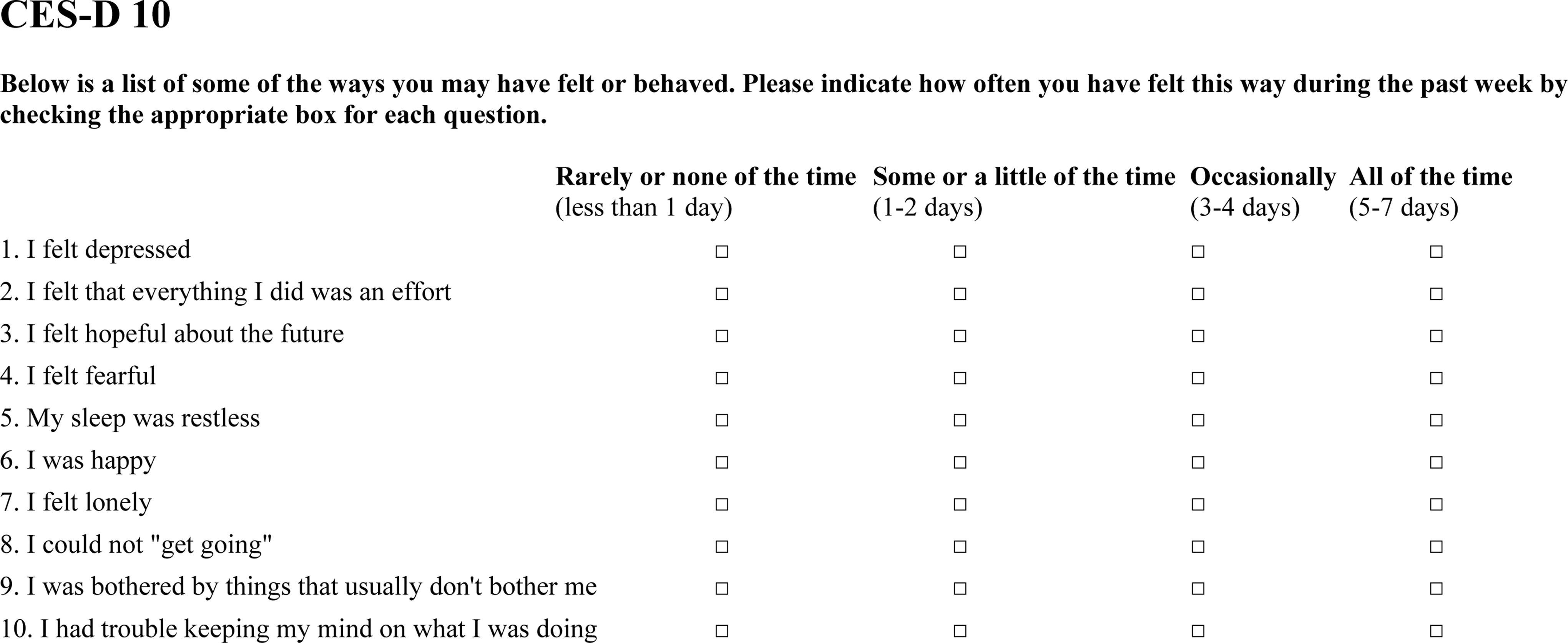
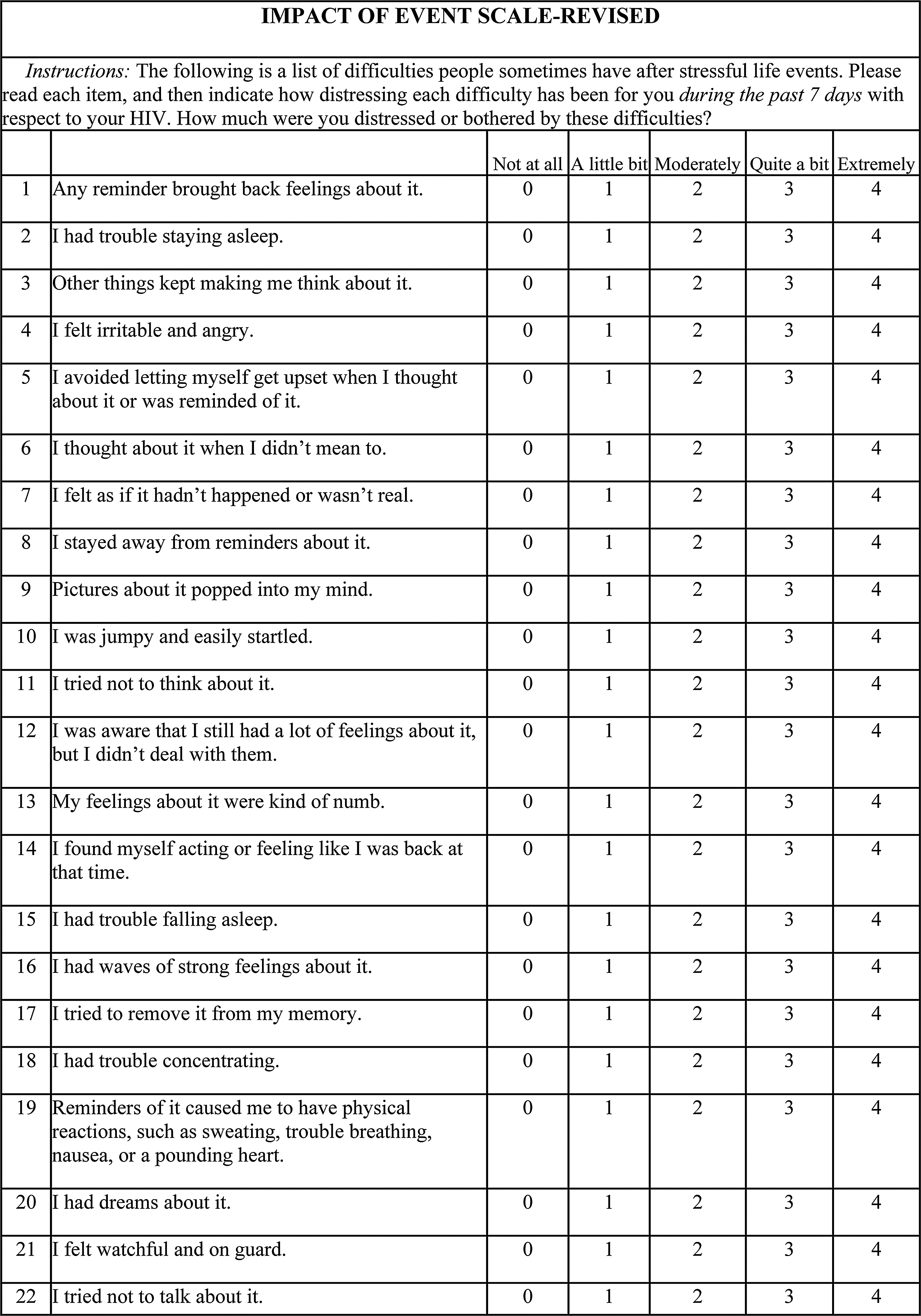
Both the 10-item depression scale of the Centers for Epidemiological Study (CES-D10; Fig. 1) and the 22-item Impact of Events Scale-Revised (IES-R) for PTSD (Fig. 2) are Likert scale screening questionnaires extensively validated and used in sub-Saharan Africa, 5,7,14,24,25,30,35,36 including in a subset of our cohort not yet on ART studied 3 years previously. 26 They were chosen for this study on the basis of this prior experience. Both questionnaires had been translated and back-translated through the two main languages used by GUM clinic patients, Mandinka and Wollof, by a mid-size group of native speakers with substantial experience working in this clinic. They were administered verbally by a medical assistant who recorded the responses prior to subjects consulting with their physician. In sporadic cases of patients literate and/or fluent in English the instruments were administered by the physician or self-administered. After the first week of recruitment physicians were allowed to omit administration of the IES-R questionnaire if they believed it would interfere with patients being seen in a timely manner.
CES-D 10.
Impact of Event Scale-Revised.
Each item of the CES-D10 is scored from 0–3 giving a potential score range of 0–30. A score of 11 or higher is typically taken as a positive screen for depression. Other similar screening instruments exist and several have been used in sub-Saharan Africa; the principle theoretical difference is between those that include constitutional symptoms of depression and those that do not in order to avoid confounding depression with fatigue or other symptoms of physical illness.
The 22 items of the IES-R are scored 0–4, with a potential range of 0–88, where a 34 or higher indicates a positive screen for PTSD. Of the 22 questions in the IES-R 16 make specific reference to an experience or event; patients were instructed to interpret these in terms of their HIV infection. The Harvard Trauma Questionnaire (HTQ) is the only other PTSD screening instrument that has been extensively validated in sub-Saharan Africa; its construction differs from the IES-R in that it enumerates the degree of trauma without allowing for subject's coping, 37 rendering it less suitable to the purposes of the current study.
Patient-related and clinical variables
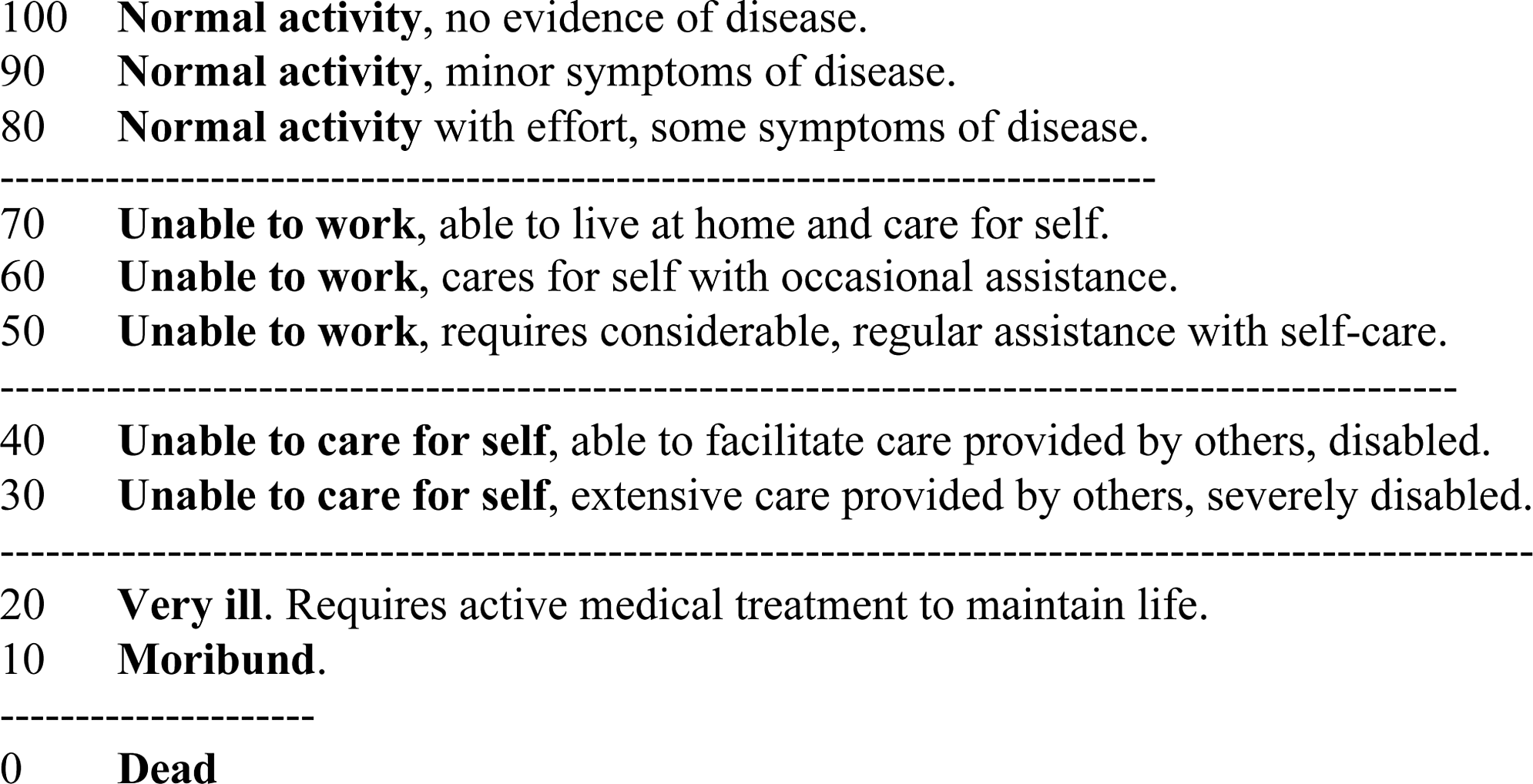
The following variables were recorded at enrollment: age, gender, current and prior CD4 cell counts, time on ART, Karnofsky score (KS) (Fig. 3) 38 , WHO clinical stage, first or second line ART, and the sequential viral load (VL) history. Clinic protocol called for VL to be drawn at baseline, week 12, week 24, and every 24 weeks thereafter.
Karnofsky Performance Score.
Statistical analysis
Questionnaires with missing or duplicate responses were omitted from analyses. Characteristics of subjects for whom CES-D10 or IES-R scores were missing were compared with those for whom scores were available using Fischer's exact test to compare categorical variables and Student's t-test to compare means. Statistical significance was defined as having a p value<0.05. Repeated data from six subjects inadvertently recruited twice were not used. The core analyses treated the raw score on the screening questionnaire as a continuous dependent variable. Associations between clinical data and the scores on the screening questionnaires were analyzed with linear regression. A multiple regression model for each of the mood disorder scores was initiated taking all variables found associated with p values<0.20 and sequentially removing the least predictive variables with p values>0.05. Analyses were performed with STATA 11 (StataCorp, College Station, TX).
Results
The mean age of the subjects was 41; 67% were female. Ninety-three percent were on first-line treatment, typically AZT/3TC/NVP for those with an HIV-1 infection. AZT/3TC/LPV/r for those with an HIV-2 infection. Average time on ART was 28 months, with an average initial CD4 cell count of 164 cells per microliter. Seventy-nine percent were fully suppressed (<100) at the time of their participation in the study, and the average most recent CD4 cell count was 425 cells per microliter. Second-line treatment was typically TDF/AZT/3TC/LPV/r or TDF/ddI/LPV/r for both those who had LPV/r in their first-line regimen and those who had been on an NNRTI.
Characteristics of the study participants are given in Table 1. Not all information was available for all participants.
100 was the lower limit of detection and 5000 defined failure by Gambian national protocols
ART, antiretroviral therapy; SD, standard deviation.
Viral suppression at week 24 is based on the VL between weeks 18–36 nearest week 24. Where both week 12 and week 48 VL were suppressed, the week 24 VL is taken to also be suppressed, in other cases it was coded as missing (33 subjects). Suppression of the most recent VL is limited to subjects with a VL at least 11 weeks on ART.
The CES-D10 and IES-R scores show a moderate degree of correlation (r=0.44, p<0.0001) in the 142 subjects for whom both results are available.
CES-D10
A CES-D10 score was available for 231 (92%) of the subjects. There were no significant differences between the characteristics of those for whom scores were available and those for whom these scores were missing (results not shown). The mean score was 5.5 (95% confidence interval 5.0–6.0). The overall prevalence of a positive screen, a score of 11 or more, was 7%. Of the 7 subjects on EFV the mean CES-D10 was 6.7 with 1 subject scoring 26. As a group these subjects did not differ from the rest (CES-D10 p=0.34, IES-R p=0.90), and were not segregated in the analyses. Two hundred twenty-four (89%) of the respondents answered question “I felt that everything I did was an effort” with a 3 (“All of the time,” i.e., on 5–7 days of the week). If the data from the current study are analyzed without this item, taking a score of 10 or higher on the remaining 9-item instrument as a positive result, the prevalence rounds down to 6% with negligible differences in univariate and multivariate analyses (data not shown).
Associations between the CES-D10 scores and the demographic and clinical variables are given in Table 2, alphabetically. Women and those on second-line ART scored higher on the CES-D10. There was also an association between higher CES-D10 scores and modest HIV disease symptoms as indicated by a KS of 90 or a WHO clinical stage of 2, although these dropped out during multiple regression analysis.
Not included: p value>0.200 in univariate analysis and not included in multiple regression; dropped: initially included, then dropped from multiple regression during sequential removal of variables with p value>0.050.
KS, Karnofsky Performance Score; CES-D10, 10-item depression scale of the Centers for Epidemiological Study; SE, standard error; ART, antiretroviral therapy; VL, viral load.
IES-R
The mean IES-R score was 29.3 with 153 observations (61% of subjects). The number of subjects for whom IES-R results were obtained was lower than that for the CES-D10 in large part because clinic physicians requested its omission during some peak periods to reduce patient waiting times. This was done without awareness of which individuals specifically would therefore not be completing the IES-R. Those with missing IES-R scores did not differ from those for whom the IES-R scores were available (data not shown). Using the standard cutoff of 34 representing a positive screening test for PTSD, 46 of 153 subjects (30%) had a positive screen for PTSD. Associations between the IES-R and the other variables are given in Table 3 in alphabetical order. Women and those with WHO stage over 1 had higher IES-R scores. Higher IES-R appeared associated with lower KS in univariate analysis, although this dropped out during multiple regression analysis.
Not included: p value>0.200 in univariate analysis and not included in multiple regression; dropped: initially included, then dropped from multiple regression during sequential removal of variables with p value>0.050.
KS, Karnofsky Performance Score; IES-R, Impact of Events Scale-Revised; SE, standard error; ART, antiretroviral therapy; VL, viral load.
Discussion
The most important finding of this study is the lower prevalence of depression in people stabilized on ART compared with those recently diagnosed and not yet on ART seen at the same center 3 years earlier. This is consistent with others' work. 24,32 While differences are most likely the result of the ART, only eight patients were subjects in both of our studies so longitudinal analysis was not possible. A selection bias cannot be excluded. Indeed it is possible that subjects enrolled in the course of routine care differ from those who died or were lost to follow-up before or during the period of enrolment. Changes in the local context such as more widespread ART use and lower HIV mortality further limit the interpretation of our results.
The fact that depression and PTSD correlated with each other makes differences between the two in this study worth special consideration. Our finding that depression improves while PTSD is largely unchanged could be the result of more of the PTSD in our cohort predating the subjects' HIV infection, with depression more driven by a response to the HIV infection. If that is the case treatment of the HIV infection might affect depression more directly than PTSD, however recent evidence calls that conclusion into doubt. 39 We found that being on second line therapy was associated with higher CES-D10 scores and not with the IES-R scores. This is consistent with depression's stronger association with adherence. Adherence shortcomings probably drove the need for second line treatment, as there was presumably negligible transmitted resistance in The Gambia during the early years of the ART roll-out. It may also be significant that subjects were monitored with VL, so their switches were not associated with severe, potentially traumatic, or life-threatening illness. Some aspects of PTSD such as greater vigilance may have an adaptive value in the setting of HIV infection, i.e. supporting adherence, while a similarly pathologic degree of depression may not have a redeeming aspect. This hypothetical possibility gains some support from our finding that achieving a documented viral suppression by the twenty-fourth week of ART was weakly associated with lower CES-D10 scores, and higher IES-R scores (analysis with week 24±2 following the clinic protocol, missing=failure, not shown). Whether PTSD helps or hinders adherence might depend on where an individual is in his or her treatment. On a cohort level a selection bias may arise in the study of PTSD in stabilized HIV-infected individuals.
One might anticipate the clinical measures, WHO stage, and KS would be more salient to individuals than CD4 cell counts and VL, and therefore more tightly associated with mood disorders. Our data suggest this is true, despite the small numbers of subjects in our study with WHO stage 3 or 4 disease, or low KS. Advanced WHO stages moreover represent a heterogenous range of clinical symptomatology.
In the current study, but not the prior one, the question “…everything…was an effort” on the CES-D10 was consistently answered in the direction most strongly suggestive of depression. Given the theoretical confounding of physical symptoms related to medical illness and somatic expressions of depression, several studies have omitted somatic questions from depression screening instruments, including this item. 21,25,40 The difference in responses to this question between the current and prior studies at our institution is striking, and difficult to attribute to the HIV infection or the ART treatment. The principle staff member administering this questionnaire was fully fluent in each of the three most important languages spoken by the subjects and was trained in the administration of the CES-D10 in the same way as interviewers in the prior study. Moreover the same Mandinka and Wollof translations were used.
While the analyses were reported with the screening questionnaires as continuous variables, parallel logistic regression analyses were performed taking the results to be binary, i.e. either the subject screened positive or not. These tended to provide similar associations with greater statistical significance, and may be closer to the manner in which the instruments would be used in clinical practice. The probabilities that the null hypotheses are correct are therefore probably overestimated by the analysis used.
Limitations
Patients with urgent medical needs were not enrolled, nor were they precisely counted, although they were few in number: less than 10. Random interruptions in the supply of questionnaires also occurred, making the patients seen not strictly consecutive. In periods of high patient load IES-R administration was left to the discretion of the physician. While this was a random process with respect to patients and did not appear to bias the results, it limited the power of the study to demonstrate associations with IES-R scores. The lack of relationship between EFV use and depression is presumably a function of both the low numbers of people on EFV and the subjects being recruited after a mean of 28 months on ART. This length of time on ART would have provided ample opportunities to substitute for EFV in the event it provoked depression in a subject.
As this study dealt only with the screening tests, rather than confirmed diagnoses, its findings should be seen as suggestions for more detailed work, and its conclusions limited to the implementation of screening.
Implementation
In this Gambian HIV clinic we demonstrated that these mood disorders occur in an important percentage of the patients, however, administering even a brief questionnaire to illiterate patients required approximately 5–10 min of staff time per patient, or the equivalent of nearly one full-time staff member. In this regard the MHI-3 41 or PHQ-2 27,42 combined with the 6-item IES-R 43 may be more practical alternatives to the instruments used in this study. Overlap between depression and PTSD suggests that one questionnaire, e.g., the MHI-5 44 could be used to screen for both in order to facilitate implementation in busy HIV clinics. The differences we found, if confirmed, may limit this 2-in-1 strategy however.
Many HIV clinics in sub-Saharan Africa cannot provide their patients core services to mitigate the impact of first line ART failure, such as VL monitoring, genotypic resistance tests, and second-line ARVs. They may also suffer from limited resources for the management of failing patients. In this setting therefore identification of individuals at risk for adherence problems, with proactive intervention to avoid the long-term complications of failing ART, are particularly important. Concerns about the feasibility of depression treatment in resource-limited settings appears to be misplaced. Such treatment is feasible, 45,46 and can be expected to yield the same benefits in low-resource settings as in high-resource settings. Several treatment modalities for PTSD also exist. 18,19 While evidence of the benefits of PTSD treatment for those infected with HIV are minimal, 17 PTSD treatment in postconflict areas in sub-Saharan Africa has shown promising results. 47,48 As depression is a modifiable risk factor for suboptimal adherence, screening for it among new HIV patients is a vital component of clinical care, even in busy clinics in sub-Saharan Africa.
Footnotes
Acknowledgments
Tumani Corrah, Assan Jaye, Francoise Lequarre, Francis Oko, and Uduak Okomo provided helpful feedback and support for the study. Kristien Velding and Yori Gidron were involved in the earlier study that helped validate these tools for use in this population and demonstrate the scope of the mood disorders problem. Abraham Alabi, Matt Cotten, and others were crucial to the delivery of high-quality, affordable VL results. Gilleh Thomas and others provided data management. Olivier Koole supported the data analysis. Famara Bojang, Tijan Janneh, Lilian Colley, and the rest of the GUM staff, and of course the patients who participated, were crucial to the success of this study. Support from the Global Fund for AIDS, TB, and Malaria made the provision of ART care in The Gambia possible, for which all involved, both patients and MRC staff, were grateful.
Author Disclosure Statement
No competing financial interests exist.