
Abstract
Despite extensive prevention efforts, an estimated 21% of individuals with HIV/AIDS in the United States are unaware of their status, placing them at greater risk for spreading the virus to others. HIV treatment as prevention (TasP) is rapidly becoming an important public health strategy to reduce HIV transmission at the population level. Data for this study were collected on a sample of 11,397 HIV-positive individuals in the Ryan White system, a publicly funded system of care for HIV-positive individuals in Los Angeles County who are uninsured, in 2009 to examine two components of TasP: baseline rates and factors associated with antiretroviral therapy (ART) use and viral load (VL) suppression in a publicly funded system of care. ART coverage among our sample was 90%. In multivariate analyses, those with a higher odds of having unsuppressed VL included: females compared to males (adjusted odds ratio [AOR]=1.25; 95% confidence interval [CI]=1.06, 1.47); African Americans compared to whites (AOR=1.42; 95% CI=1.24, 1.62); men who have sex with men compared to heterosexuals (AOR=1.15; 95% CI=1.00, 1.32); recent substance abusers compared to nonsubstance abusers (AOR=1.35; 95% CI=1.17, 1.55); those recently incarcerated or ever incarcerated compared to those never incarcerated (AOR=1.37; 95% CI=1.15, 1.63; and AOR=1.28; 95% CI=1.09, 1.50); and those retained in care compared to those not retained in care (AOR=1.98; 95% CI=1.76, 2.22). Understanding the key sociodemographic, geographic and behavioral factors associated with ART use as well as HIV VL suppression will be useful for informing the development and deployment of targeted programming and policies that may further enhance the implementation of the TasP approach in communities across the United States.
Introduction
HIV
A number of studies have provided findings to support TasP as an effective strategy for the prevention of new HIV infection. A mathematical modeling study predicted that in South Africa, annual voluntary screening followed by the immediate initiation of ART for those individuals testing positive regardless of their CD4 count could reduce HIV incidence and mortality to less than 1 case per 1000 people per year by 2016, and reduce the prevalence of HIV to less than 1% within 50 years. 9 Additional modeling studies have also supported TasP's potential to substantially reduce HIV transmission. 8,10,11 Recent clinical studies have provided strong evidence for a reduction in forward HIV transmission as a result of early initiation of ART. 12 –16 HPTN 052, the first randomized controlled trial designed to examine the impact of ART on HIV transmission demonstrated that early initiation of ART resulted in a 96% decrease in the risk of HIV transmission among serodiscordant partners and a 41% decrease in HIV-related clinical events. 12 Additionally, an observational study found that the early initiation of ART for individuals with a CD4 count between 500–799 cells/mm3 significantly improved survival rates as compared with deferred therapy, providing support for early treatment to reduce morbidity and mortality. 13 Despite the growing body of evidence of both individual and public health benefits of earlier ART initiation, a number of potential barriers to TasP have also been cited, including scalability, acceptability, drug resistance, and viral load rebound, adherence, side effects, and the short and long term economic costs of TasP. 7,9,10 In order for TasP to succeed as a public health strategy, it is critical to understand the current state of and potential barriers to TasP in highly impacted communities. This includes understanding baseline ART treatment and VL suppression rates, how they vary by subpopulation or geography, and what target groups may require more intensive intervention for the TasP strategy to succeed.
The purpose of this study is to examine two key components of TasP implementation: ART use and VL suppression in a population of HIV-positive persons in Los Angeles County (LAC). Using data from the LAC Ryan White (RW) system of care, which serves approximately 40% of known persons living with HIV/AIDS (PLWH) in the county, we examine the following in a cohort of 11,397 HIV-positive patients: (1) overall ART treatment coverage rates and how they vary by sociodemographics, behavioral characteristics, clinical factors, and geography and (2) factors associated with having unsuppressed HIV VL in bivariate and multivariate analyses. These findings will provide valuable information in helping to assess the feasibility of using TasP in LAC, a large and populous jurisdiction and the second largest epicenter of HIV in the nation. 17
Methods
Sample and data collection
Analysis for this study was performed on a sample of 11,397 HIV-positive individuals who received HIV medical care from the LAC RW system, and had (1) one or more medical visits in the RW system between January 1, 2009 and December 31, 2009 and (2) a valid VL measure during the 2009 calendar year. Of the 14,799 clients who had at least one medical visit in the RW system between January 1, 2009 and December 31, 2009, 12,752 (86%) had a valid VL measure and 11,397 (77%) had complete data on all covariates, which represents the final sample used for the analysis. All data in this study were collected through the Casewatch Millenium™ system (ACMS Inc., Hollywood, CA), which collects patient level clinical, administrative, and utilization data for the LAC RW system of care. Data are entered into Casewatch directly by HIV clinic staff and by electronic interfacing with electronic health records and electronic laboratory records. Casewatch is used for billing and reimbursement of medical care, mandatory reporting to the Health Resources Service Administration (HRSA), as well as monitoring of population health and clinical quality of care.
Measures
Measures included sociodemographics, behavioral characteristics, clinical factors, zip code of residence for geographical analysis, ART use, and HIV VL.
Sociodemographics, behavioral characteristics, and clinical factors.
Sociodemographic characteristics included self-reported gender (male/female/transgender), race/ethnicity (White/African American/Latino[Hispanic]/Asian Pacific Islander/Native American/Mixed race[other]), age (13–24/25–39/40–49/50+), income level (≤100% Federal Poverty Level [FPL]/>100% FPL), mode of HIV exposure (MSM/IDU/heterosexual/other), living situation (permanent housing/nonpermanent housing such as transient or transitional housing/homeless), health insurance status (none/public [Medicaid/Medicare/VA]/private), and being new to the RW system of care (yes/no). Behavioral characteristics were self-reported and included history of substance abuse (recent use within the last 12 months/has used but not within the last 12 months/never used), and incarceration history (recent incarceration in the last 24 months/ever incarcerated greater than 2 years ago/never incarcerated). Clinical characteristics included most recent measure in 2009 of CD4 cell count from electronic laboratory records (<200/201–350/351–500/500+), time with HIV infection (≤1 year/>1 year based on self-reported date of diagnosis), and retention in care (defined as having at least 2 medical visits 90 days apart within a calendar year based on utilization data from billable visits).
Zip code of residence.
Zip codes were used to map the geographical distribution of patients with unsuppressed VL by Service Planning Area (SPA). The LAC Department of Public Health uses eight geographical regions known as SPAs to structure planning and service delivery in LAC. 18 The most recent entry for patient zip code of residence in the calendar year 2009 was used for the analysis. If a patient was homeless or unstably housed, they were assigned the zip code of their shelter or the cross streets where they report sleeping and spending the majority of their time.
ART Use.
ART use was determined by data from one of two Casewatch variables: (1) a patient was currently on an antiretroviral regimen (updated every 3 months) or (2) the patient was receiving antiretroviral therapy from the AIDS Drug Assistance Programs (ADAP) in the 2009 calendar.
HIV VL.
HIV VL measurements were electronically reported to Casewatch directly from laboratories. Specific VL assays reported to the system varied, with the lowest limit of detection of less than 25 copies, and the highest upper limit of detection of 6,000,000 copies. Unsuppressed VL was defined as the most recent viral load measure for the patient in 2009 reported as more than 200 copies/mL. Mean VL was calculated by summing the most recent HIV VL value for each unique patient in 2009, and dividing by the total number of patients in the sample. Mean VL by SPA used the same calculation for the sample of patients with resident zip code in each of the 8 SPAs. To assign a value to VL that were below the lower limit of detection for the assay, the average between 0 and the lower limit of detection was assigned, consistent with the 2011 Centers for Disease Control and Prevention (CDC) recommendations on calculations for in care community VL. 19 For example if a value was reported as less than 48 copies, the value of 24 (0+48/2=24) was assigned to that measurement. VL values that exceeded the upper limit of detection were assigned a value of the highest level of detection of the assay.
Data analysis
We first examined the distributions of all independent and dependent variables. We then examined the bivariate association between ART coverage and sample characteristics. Next, we used ArcGIS (ESRI ArcMap version 9.3; ESRI, Redlands, CA) to map the geographical distribution of patients with unsuppressed VL by SPA using client residence zip code. Using SPA 4 as the comparison group, χ2 test were used to identify significant differences (p<0.05) in unsuppressed VL by SPA, and Wilcoxon-rank sum test for differences (p<0.05) in mean VL by SPA. We then used logistic regression to assess the unadjusted and adjusted odds ratios (UOR/AOR) for the associations between the main outcome variable (unsuppressed VL) and sample characteristics. We conducted a sensitivity analysis to assess whether significant differences existed in the covariates for the adjusted analyses when using models without missing covariates (N=11,397) compared to models with missing covariates (N=12,752). We found no statistically significant differences between the models. The VL suppression rate for patients with missing covariates was 71% compared to 73% for patients without missing covariates. Finally, we developed a number of bivariate and multivariate models that included two- and three-way interactions with several key variables including gender, race/ethnicity, and risk group to test for potential confounding. We did not find any significant interaction effects, thus we do not present the findings from these analyses in the results section. All analyses were conducted using SAS version 9.2 (SAS Institute, Cary, NC).
Results
Sample characteristics
Sample characteristics are presented in Table 1. The majority of the sample was male (84%). Over half were Latino/Hispanic (51%), 23% were white, and 22% were African American. Sixty-five percent were 40 years of age or older, had an income level 100% or less of the FPL, and were MSM. Twelve percent had nonpermanent housing or were homeless, and 61% had no health insurance. Twenty-eight percent of the sample had a history of substance abuse, and 18% had a history of incarceration. Thirty percent had a CD4 cell count less than 351 cells/mm3, and 27% had an unsuppressed VL.
FPL, Federal poverty level, MSM, men who have sex with men; IDU, injection drug use; RW, Ryan White.
Association of ART coverage with sample characteristics
Of the total sample, 90% were currently on ART (Table 2). In bivariate analysis, females were less likely than males and transgender individuals to be on ART. Of all age groups, those 13–24 years of age were least likely to be on ART. MSM were most likely to be on ART while injection drug use (IDU) were least likely to be on ART. Those with a history of substance abuse and incarceration were least likely to be on ART. Individuals with a CD4 cell count less than 350 cells/mm3 were more likely to be on ART than those with a CD4 cell count greater than 350 cells/mm3, however, ART coverage rates were high even among those with CD4 greater than 500 cells/mm3 (86%).
FPL, Federal poverty level; MSM, men who have sex with men; IDU, injection drug use; RW, Ryan White.
Geographic distribution of unsuppressed VL
Twenty-seven percent of the sample had an unsuppressed VL. Percentages varied by geographical region (Fig. 1). When compared to the largest SPA 4 in the metro/downtown area of LAC, the south SPA 6 had the highest percentage of individuals with an unsuppressed VL (32.2%) and mean VL (25,179 copies/mL) while the San Gabriel Valley SPA 3 had the lowest percentage of individuals with an unsuppressed VL (21.9) and mean VL (11,763 copies/mL).
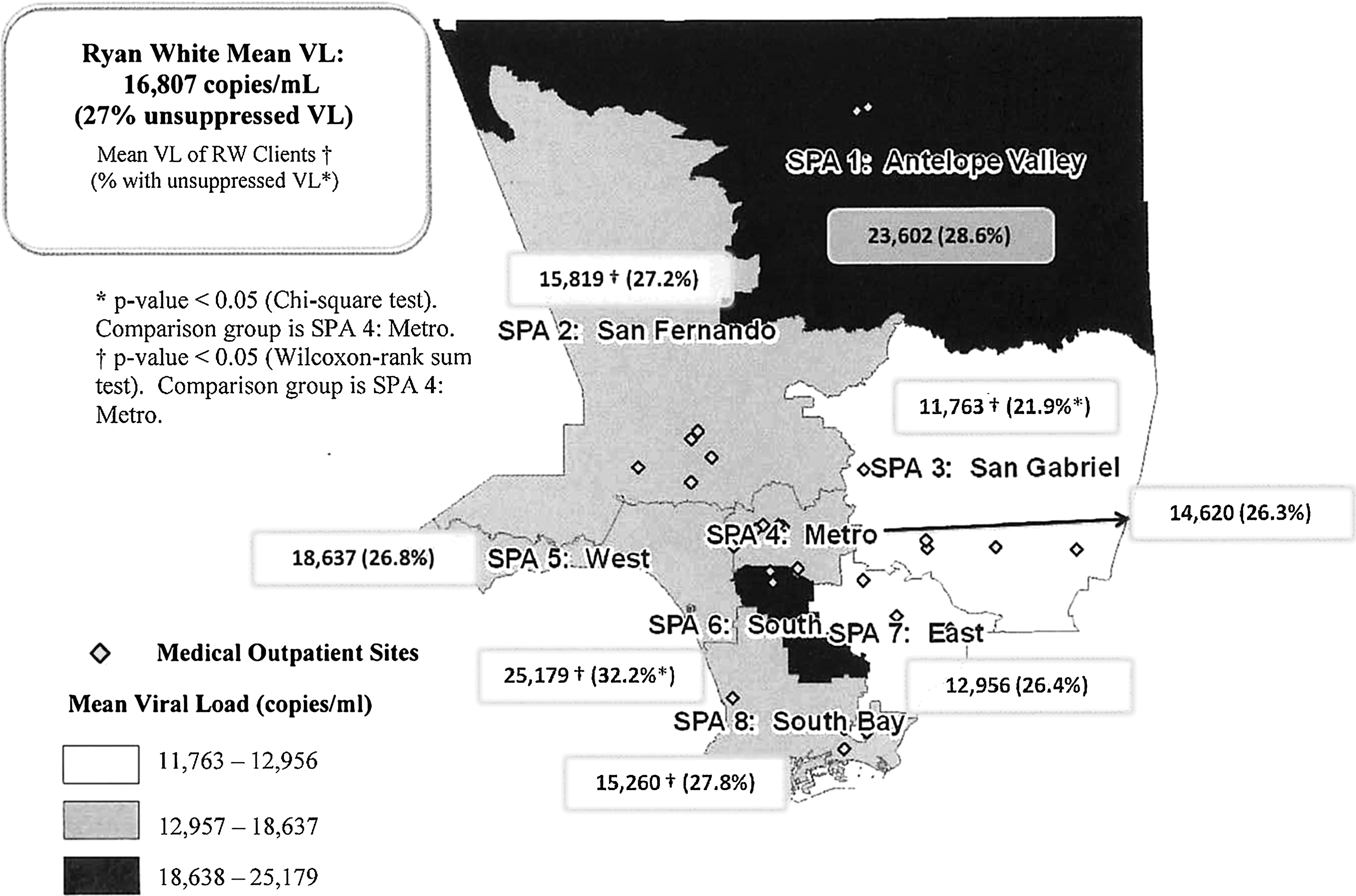
Geographic distribution of mean viral load (VL) and unsuppressed VL.
Association of unsuppressed VL with sample characteristics
The UOR and AOR for the bivariate and multivariate associations of unsuppressed VL with sample characteristics are presented in Table 3. In the multivariate analyses, those with a higher odds of having unsuppressed VL included: females compared to males (AOR=1.25; 95% CI=1.06,1.47); African Americans compared to whites (AOR=1.42; 95% CI=1.24, 1.62); individuals between the ages of 13–24, 25–39, and 40–49 compared to those 50 years of age or older (AOR=3.29; 95% CI=2.54, 4.26; AOR=1.84; 95% CI=1.62, 2.09; and AOR=1.22; 95% CI=1.08, 1.38); those with incomes 100% or less FPL compared to those with incomes greater than 100% FPL (AOR=1.27; 95% CI=1.14, 1.40); MSM compared to heterosexuals (AOR=1.15; 95% CI=1.00, 1.32); individuals without health insurance compared to those with private insurance (AOR=1.32; 95% CI=1.06, 1.64); recent substance abusers compared to non-substance abusers (AOR=1.35; 95% CI=1.17, 1.55); those recently incarcerated or ever incarcerated compared to those never incarcerated (AOR=1.37; 95% CI=1.15, 1.63; and AOR=1.28; 95% CI=1.09, 1.50); individuals with a CD4 cell count less than 200, 201–350, or 351–500 compared to those with a CD4 cell count greater than 500 (AOR=7.46; 95% CI=6.45, 8.63; AOR=2.70; 95% CI=2.38, 3.05; and AOR=1.71; 95% CI=1.52, 1.92); those who have been living with HIV for 1 year or less compared to those living with HIV for more than 1 year (AOR=2.28; 95% CI=1.81, 2.86); and individuals currently on ART compared to those not currently on ART (AOR=1.97; 95% CI=1.69, 2.30). Conversely, Latinos/Hispanics and Asian/Pacific Islanders had a lower odds of having unsuppressed VL compared to whites (AOR=0.87; 95% CI=0.77, 0.98; and AOR=0.60; 95% CI=0.44, 0.81).
p<0.05.
p<0.01.
p<0.001.
VL, Viral load; OR, odds ratio; CI confidence interval; FPL, Federal poverty level; MSM, men who have sex with men; ART, antiretroviral therapy; RW, Ryan White.
Discussion
Our analysis found that overall, rates of ART coverage for PLWHA in the LAC RW system of care were high (90%). While the Department of Health and Human Services (DHHS) adult and adolescent treatment guidelines 20 did not first strongly recommend ART for patients with CD4 counts between 350–500 cells/mm3 until December 2009 (the last month of this analysis), it appears that the majority of patients in our sample (88%) with CD4 counts in this range were on ART at the time of the analysis. Similarly, a majority of patients (86%) with CD4 greater than 500 cells/mm3 in the sample were also on ART. This is likely in part due to successful immune reconstitution achieved by PLWHA who started ART at lower CD4 counts, but may also reflect a trend in provider's prescribing ART based on the emerging evidence of the benefits of earlier treatment, 13 –17 which ultimately informed the December 2009 changes in treatment guidelines. These findings do suggest that achieving high ART coverage rates for those PLWHA who are currently accessing HIV care is feasible, and future studies are needed to better understand the relative role of provider and patient attitudes and behaviors in achieving the universal ART coverage that is a key component of the TasP strategy. The analysis also found that despite high ART coverage rates, a substantial portion of PLWHA taking ART were not achieving HIV VL suppression (27%), which leads to suboptimal treatment outcomes. Given that having PLWHA on treatment achieves a suppressed HIV VL is paramount to the success of TasP, the findings of our analysis highlight the critical role that targeted, effective, evidence-based ART adherence interventions will need to play in a local LAC TasP strategy.
There were significant geographic differences in HIV VL suppression throughout LAC. Our analysis revealed that RW patients living in the SPA 6 south Los Angeles area, as well as the SPA 8 Long Beach area had higher rates of unsuppressed VL when compared to the largest SPA 4 in the metro/downtown area of LAC. These findings inform additional geospatial analysis down to the zip code and census tract level, which are currently underway. Understanding geographic variations in HIV VL are critical to implementing a targeted and effective TasP strategy with available resources, particularly in a jurisdiction as populous and geographically large as LAC. Mapping the geographic distribution of mean VL for this cohort allows us to identify the communities that may have the highest risk of forward HIV transmission due to higher levels of HIV VL among residents. This community level approach to analyzing the VL of our cohort may also inform the alignment of local HIV testing activities to further enhance the disease identification arm of TasP in the highest risk communities.
Factors associated with having unsuppressed HIV VL in the adjusted analysis of our LAC cohort included gender, race/ethnicity, age, income, insurance status, mode of exposure, substance use, incarceration, and clinical variables (HIV diagnoses <1 year ago, CD4 count, currently on ART). Other studies have reported similar findings. 21 –28 For example, females had higher odds of unsuppressed VL than males, consistent with prior studies that have shown HIV-positive women continue to experience treatment disparities in ART access, early ART discontinuation, and some clinical treatment outcomes. 22,23 Similarly, African Americans had higher odds of unsuppressed HIV VL compared with whites, which is also consistent with several studies demonstrating poorer access and treatment outcomes for African Americans living with HIV/AIDS. 22 –28 Interestingly, Latino/as along with Asians had lower odds of having unsuppressed HIV VL when compared to whites. This is in contrast to several studies that have shown disparities for Latinos in HIV care, and may suggest that while Latinos have historically experienced barriers to accessing health care and services, once they attain this access (as reflected by being included in the cohort), they have a higher likelihood of achieving optimal treatment outcomes. Further studies of these outcomes in the highly impacted Latino population are warranted. Also consistent with previous literature, youth, and individuals with recent substance use and incarceration have higher odds of unsuppressed VL. 22,23,29 –32 These findings highlight the importance of developing comprehensive and effective strategies for reducing barriers to engagement, ART use, and adherence support for these often marginalized populations. Targeted interventions across the continuum of care for those at highest risk of having unsuppressed HIV VL are critical to the implementation of a responsive and effective local TasP strategy.
While several aspects of the analysis further inform the implementation of TasP as a public health HIV prevention strategy, there were limitations to our analysis. First, the sample of PLWHA in the analysis included only those who receive care in the RW safety net system of care (approximately 40% of all known LAC PLWHA), and is not generalizable to the PLWHA in LAC who may receive their medical care outside the RW system. Additionally, in order to be included in the sample, individuals had to have at least one medical visit, and one HIV VL performed in 2009. Therefore, individuals who were not in care at all in 2009 and did not have an HIV VL measurement would not be included in the sample. As a consequence of being out of care, these PLWHA are also most likely to have an unsuppressed VL, which means that our sample underestimates the true rates of ART coverage and unsuppressed VL for all PLWHA in LAC. Finally, our measurement of ‘on ART’ utilized 2 data fields entered by medical providers and updated quarterly, and therefore does not reflect real time pharmacy data or account for the time it may take individuals to achieve VL suppression after starting ART.
Conclusion
This analysis provides important information about the ART coverage rates and VL suppression in a large cohort of PLWHA in care in LAC. Understanding the key sociodemographic, geographic, and behavioral factors associated with ART use as well as unsuppressed HIV VL inform the development of targeted programming and policies that may further enhance the implementation of the TasP approach in communities across the US. Additionally, identifying the key populations that experience lower rates of ART use and HIV VL suppression allows for the development and deployment of interventions to optimize access to and retention in HIV care and treatment, with the goal of reducing VL, improving health outcomes for PLWHA, reducing forward transmission, and ultimately curbing the HIV epidemic.
Footnotes
Acknowledgment
This work was supported in part through grants from the Centers for Disease Control and Prevention Division of HIV AIDS Programs [PS10-10181] and the Health Resources and Services Administration [H89HA00016] to the Los Angeles County Department of Public Health.
Author Disclosure Statement
No competing financial interests exist.