
Abstract
The current study was a meta-analysis of the efficacy of educational, psychosocial or behavioral interventions that were conducted in China to promote HIV/sexual risk reduction. A total of 26 intervention studies qualified for the meta-analysis. Outcome variables for which effect sizes were calculated included condom use with different types of sexual partners, HIV/AIDS knowledge, condom use knowledge, intentions of condom use, condom use self-efficacy, and others. Mean weighted effect sizes were calculated for each outcome measure across reviewed studies; effect size for each outcome measure was weighted by their inverse variance; fixed effects and random effects meta-analytic procedures were used. The Q statistic was used to examine whether the effect sizes were homogeneous in nature and moderating analysis (i.e., the Qb statistic) was used to compare the effect sizes of intervention studies that were different in a number of categorical variables. The reviewed interventions were successful in improving HIV knowledge (d=0.706), condom use knowledge (d=0.620), attitudes toward people living with HIV/AIDS (PLWHA; d=0.625) and in increasing condom use with regular partners (d=0.477), condom use with casual partners (d=0.444), general condom use (d=0.408), and condom use self-efficacy (d=0.584) among target audiences. In addition, moderating analyses on three most examined variables, including HIV knowledge, condom use, and attitudes toward PLWHA, demonstrated that interventions that reported the conduction of formative research and process evaluation, that were peer-led, and that included only one follow-up were more likely to report a positive impact on condom use behavior among target audiences (p<0.001), HIV knowledge (p<0.001), or attitudes toward PLWHA (p<0.001).
Introduction
A number of prevention intervention programs have been conducted to reduce HIV-related sexual risk-taking behaviors among various Chinese populations. Several narrative reviews have compared and integrated the components of the intervention studies, including location, sampling, design, intervention strategies, and outcomes. But we know little about the efficacy of these interventions in reducing HIV-related sexual risk-taking behavior. No study has quantitatively synthesized the existing HIV intervention literature and examined whether these behavioral interventions are effective (efficacious) in reducing sexual risk behavior among Chinese populations. “Future preventive interventions, however, will only have the greatest chance of being effective if lessons learned from past intervention efforts are seriously considered.” 6(p335) Meta-analysis has been introduced to examine the efficacy of intervention studies in behavioral, health, and social sciences. 7 Meta-analysis, which is a statistical technique similar to research synthesis, provides more objective appraisals of the evidence than conventional narrative reviews due to four primary advantages, including using structured discipline on literature searches, representing key findings in a manner that focuses on effect sizes rather than on qualitative summaries or statistical significance, coding study characteristics systematically, and handling large number of study studies. 7
In the current study we sought to quantitatively appraise the overall efficacy of interventions on reducing HIV/sexual risks in China and to conduct a meta-analysis to examine efficacy of the HIV interventions in changing HIV-related knowledge, attitudes, and behaviors among various Chinese populations. We also sought to identify intervention and study characteristics that were associated with the efficacy of HIV behavioral prevention interventions in China.
Methods
Sources of literature
Comprehensive literature searches were conducted to obtain relevant studies. Studies were retrieved from (1) computerized databases, including PsycINFO, MEDLINE, and Academic Search Complete. Dissertation Abstracts, using combinations of the keywords HIV, AIDS, sexual behavior, intervention, campaign, HIV knowledge, safer sex, safer sexual behavior, condom use, HIV testing, China; (2) reference sections of relevant manuscripts; (3) the reference list of the review study conducted by Hong and Li. 2 To exhaust potential intervention studies, this process was iterated between August 2010 when we started the study and upon completion of the initial coding in October 2011 until no new articles were identified.
Inclusion/exclusion criteria
A study staff conducted an initial screening based on title and abstract review. Remaining citations were then screened by two independent coders based on a thorough reading of the full-text articles. Studies were included in this meta-analysis if they met the following criteria: (1) studies that were conducted in China to quantitatively examine any educational, psychosocial or behavioral interventions promoting HIV/sexual risk reduction; (2) studies that were published in peer-reviewed English journals prior to October 2011; (3) studies that provided information needed to calculate effect sizes; (4) studies that employed an experimental (e.g., randomized controlled trial) or quasi-experimental design with an appropriate control group; (5) studies that reported an empirical outcome evaluation that assessed the impact of the campaign/intervention on the following educational, psychological, and behavioral outcomes. The educational outcomes included HIV knowledge and condom knowledge; psychological outcomes were condom use intentions, condom use self-efficacy, attitudes toward HIV, and attitudes toward people living with HIV/AIDS (PLWHA); the behavioral outcomes included condom use, and HIV testing. Some studies also assessed rates of HIV infection. Therefore, HIV infection was included as one outcome variable.
Those interventions focused on only occupational prevention of blood-borne pathogens, antiretroviral treatment programs, testing for only other STDs, or contraceptive-only interventions were excluded. Also, since the focus of this review was on primary HIV prevention interventions, secondary interventions among HIV-infected individuals were excluded. In addition, interventions targeting solely injection drug use or solely on reducing HIV-related stigma, or solely improving attitudes toward people living with HIV/AIDS (PLWHA) were excluded. Studies were excluded if they used a within-subjects design with no control/comparison condition. Studies that were written and/or published in Chinese were excluded from the current review because they were difficult for readers outside of China to access. 8
Article coding
Two independent coders coded all the articles in the final data set on nine dimensions of interest, including location, intervention year, sample, target population, formative research, use of theory, intervention description, process evaluation, and outcomes. Methodological quality (MQ) for each study was also coded on 12 items derived from Miller and Wilbourne's 9 Methodological Quality Rating Scale (MQRS) and Kennedy and collegues' 10 study. Sample items include “prospective cohort,” “random assignment of participants to the intervention,” “follow-up rate of 80% or more,” “control/comparison groups equivalent on sociodemographic measures,” “control/comparison groups equivalent at baseline on outcome measures,” “outcome data collected by personnel blind to treatment condition.” One point was awarded for each of these 12 items. Holsti's 11 formula was used for calculating intercoder reliability. The intercoder reliability ranged from 0.80 to 1.0. The two coders discussed disagreements with the first author and arrived at agreement on all discrepancies.
Publication bias
Publication bias was first examined by generating funnel plots of the weighted mean effect size by standard error. 12 Funnel plot asymmetry was tested by rank correlation test to examine the correlations between standardized effect size estimates and their variances 13 and by linear regression to regress standardized effect size estimates against their precisions that was defined as the inverse of the standard error). 14
Effect size calculation
The standardized mean difference (d), which is defined as the mean differences in groups divided by the pooled standard deviation, was employed as the effect size indicator. However, this effect size index suffers from a slight upward small sample size bias. Therefore, effect sizes were corrected for such a bias using recommended formulas. 7 Available data (e.g., F or t values, summary statistics) were used to calculate effect sizes. When odds ratios were reported, they were transformed to d using the natural logarithm; and when results were reported in percentages, they were converted to odds ratios first and then to d following appropriate formulas. 15
Multiple effect sizes were calculated for individual studies when more than one educational, psychosocial, or behavioral outcomes were reported. These effect sizes were coded and presented separately. If a study contained multiple comparison conditions, the average of the effect sizes was used in analysis. If a study targeted different populations and assessed a same outcome for these different target audiences, the effect sizes were also coded and presented separately. If a study contained more than one follow-up time points of data, the data from the longest follow-up were used to calculate the effect size. In addition, effect sizes with a positive sign indicated that the intervention condition outperformed the control or comparison condition and effect sizes with a negative sign indicated that the reverse.
In the studies that examined condom use, some included general condom use (i.e., without specifying the types of sexual partners), some others asked questions in reference to specific types of partners (e.g., regular, casual). Accordingly, the current study coded the studies that examined condom use into “condom use with regular partners,” “condom use with casual partners,” and “general condom use.” The final set of outcome variables for which effect sizes were calculated included condom use with regular partners, condom use with casual partners, general condom use, HIV/AIDS knowledge, condom use knowledge, attitudes toward PLWHA, intentions of condom use, condom use self-efficacy, attitudes toward HIV, and HIV infection.
Meta-analysis
Effect size for each outcome measure was weighted by its inverse variance. 7 Mean weighted effect sizes were calculated for each outcome measure across reviewed studies and the Q statistic was used to examine whether the effect sizes were homogeneous in nature. Random effects procedure was then employed based on the results of heterogeneity analysis. The Qb statistic was employed to compare the effect sizes of intervention studies that were different by a number of design features including inclusion of formative research (yes/no), use of a theory (yes/no), inclusion of process evaluation (yes/no), type of intervention facilitators (peer-led versus professional-led), and number of postintervention follow-up surveys (one versus two or more). A significant Qb statistic indicates that the design feature can significantly explain the variance and difference in effect sizes. 7 SPSS Macros for Meta-Analysis (SPSS Inc., Chicago, IL) were used to conduct all data analyses. 7
Results
Characteristics of studies
Initial searches resulted in 242 abstracts that were examined more closely for their potential relevance to this review. A total of 70 articles that had the potential to be included in the review were retrieved in full text and examined. Based on our exclusion criteria, a number of articles were subsequently excluded, including 16 studies that used pretest–posttest one group design; 11 (15.7%) studies that had English abstracts but were published in Chinese journals; 5 studies (7.1%) that focused on occupational prevention of blood-borne pathogens, biologic HIV prevention approaches and antiretroviral treatment programs; 6 studies (8.6%) that focused on conceptual development and methodological overview rather than on outcome evaluations of HIV interventions; 1 study (1.4%) that focused only on drug use practices; 3 studies (4.3%) that focused on HIV-infected heterosexual men; 2 studies (2.9%) that focused solely on reducing HIV-related stigma and improving attitudes toward PLWHA. Consequently, a total of 26 articles were included in the final data set for review. On average, studies received 7.3 of 12 possible points for study design and methodological quality. Methodological quality scores for each study are shown in Table 1.
MQ, methodological quality; HBM, health belief model; SCT, social cognitive theory; TRA, theory of reasoned action; PLWHA, people who live with HIV/AIDS; FSW, female sex workers; MSM, men who who sex with men; STI, sexually transmitted infection; STD, sexually transmitted disease; PMT, protection motivation theory; IDUs, injection drug users; CSWs, commercial sex workers.
The 26 studies had a cumulative sample size of N=46,055 (median N per study=1337). Most studies (κ=17, 65.4%) reported mean age of the participants. On average, the study samples of the 17 studies that reported mean age were 22.21 years old (standard deviation [SD]=6.26). Most of the intervention studies were published after the year of 2001 (approximately 50% of publications occurred after 2008). Five studies were conducted in Shanghai, 16 –20 4 studies in Sichuan Province, 21 –24 3 in Fujian Province, 25 –27 2 in Yunnan Province, 28–29 Nanjing, 30,31 and Hong Kong, 32,33 respectively. Other study locations include Guangxi, 34 Henan, 35 Anhui, 36 Hainan, 37 and Beijing, 38 with only one study conducted in each of these locations. Two studies were conducted in multiple provinces. 39,40 And one study used “a large eastern city” to label the location. 41 The target population for these studies included high school students (κ=5), 16,25,27,31,35 female sex workers (κ=2), 22,34 market workers (κ=2), 26,41 farmers/villagers (κ=1), 29 both villagers and students (κ=1), 28 unmarried youth (κ=2), 19,20 injection drug users (κ=2), 24,40 men who have sex with men (κ=2), 21,32 college students (κ=1), 30 truck drivers (κ=1), 33 children of migrant workers (κ=1), 17 ethnic cultural groups (κ=1), 23 general population (κ=1), 39 female migrants (κ=1), 38 rural primary school students (κ=1), 37 both high school and college students (κ=1), 18 both health workers and villagers (κ=10). 36 In addition, the 26 reviewed studies conducted an average of 1.27 (SD=0.45) postintervention follow-up surveys (76.9% one follow-up and 23.1% two follow-ups).
In the current review, only 35% studies (κ=9) reported using a theory or a conceptual model as a guiding framework for the intervention. The theories and models reported in these studies included the health belief model, 42 the theory of reasoned action, 43 social cognitive theory, 44 diffusion model, 45 protection motivation theory, 46 subcultural model, 47 leadership-focused model, 48 communication model, 49 empowerment model, 50 and social action model. 51 Also, only 31% intervention studies (κ=8) reported conducting some formative research during the development of intervention. The methodologies of formative research in these studies included pilot testing, focus groups, in-depth case studies or interviews, special workshops, and group discussions. In addition, 42% (κ=11) of the studies reported conducting some type of process evaluation, including intensive interviews with prevention workers and focus groups with participants. Some studies reported the percentage of participants who read educational materials, were involved in intervention sessions, were familiar with educational materials, or received intervention manuals. Some studies reported duration or length of the intervention; for example, the days, hours, or sessions of workshops or seminars.
In the current review, two studies (8%) reported using printed logos along with other printed materials to deliver relevant intervention messages. 21,26 Most studies tended to use peers (κ=9, 35%), or professionals/paraprofessionals such as faculty members, health workers, physicians, nurses, fieldworkers, and project staff (κ=12, 46%) to facilitate the intervention delivery. Two studies (8%) used popular opinion leaders to disseminate the intervention messages and 3 (12%) used the Internet as an intervention delivery channel. In addition, most of the studies employed a combination of printed materials (e.g., brochures, pamphlets, books, flyers, newsletters, billboards, blackboards, posters), face-to-face (e.g., workshops, seminars, voluntary counseling and testing programs, didactic lectures, group discussions, role plays, peer education, or outreach), and visual/audio materials (e.g., videos, audio tapes, VCDs and cartoon folders) to deliver the intervention messages. Only one study 36 mentioned that radio and television were used to deliver intervention programming. In addition, a number of studies used a variety of creative art items such as coaster and making-friend cards as well as other preventive activities such as distribution of free condoms, free needles, and other sterile injection equipment.
Furthermore, the current review found that condom use (κ=16, 62%), HIV knowledge (κ=21, 81%) and attitudes toward PLWHA (κ=6, 23%) were the most common outcome measures, followed by condom knowledge (κ=4, 15%), condom use self-efficacy (κ=4, 15%), intention to use condoms (κ=3, 12%), attitudes toward HIV (κ=3, 12%), and HIV/STD infection (κ=3, 12%), communication on HIV/AIDS (κ=1, 4%). Since studies that included general condom use, condom use with casual partners, and condom use with regular partners were coded separately, κ=24 rather than κ=16 effect sizes were included in the data analysis related to condom use. In addition, one study assessed attitudes toward PLWHA for two different target populations, therefore, κ=7 rather than κ=6 effect sizes were included in the data analysis related to this variable. Table 1 presents the characteristics of the reviewed studies and the effect sizes for each outcome variable.
Efficacy of interventions
Mean weighted effect sizes, 95% confidence intervals, and significance tests on the outcome variables were shown in Table 2. The significant Q statistics demonstrate that all of these mean effect sizes exhibited heterogeneity, which indicates that the variance of the sample of effect sizes is greater than what is expected from sampling error alone. Compared to control conditions, HIV prevention/sexual risk reduction interventions improved HIV knowledge (d=0.706, 95% confidence interval [CI]: 0.477–0.935, κ=21; Fig. 1), condom knowledge (d=0.620, 95% CI: 0.204–1.036, κ=4), attitudes toward PLWHA (d=0.625, 95% CI: 0.172–1.077, κ=7), and attitudes toward HIV (d=0.385, 95% CI: −0.023–0.794, κ=3). Of those studies that assessed condom use (Fig. 2), interventions significantly increased condom use with regular partners (d=0.477, 95% CI: 0.090–0.863, κ=6), condom use with casual partners (d=0.444, 95% CI: 0.155–0.660, κ=9), general/unspecified condom use (d=0.408, 95% CI: 0.155–0.660, κ=10), and condom use self-efficacy (d=0.584, 95% CI: 0.262–0.905, κ=4). Also, HIV prevention/sexual risk reduction interventions lowered HIV/STD infections (d=0.159, 95% CI: −0.007–0.325, κ=3). Random effect sizes ranged from d=0.159 (attitudes toward HIV) to d=0.706 (HIV knowledge). Forest plots of effect sizes and 95% confidence intervals of the interventions' impact on the two most common outcome measures (i.e., HIV knowledge and condom use) were displayed in Figs. 1 and 2.
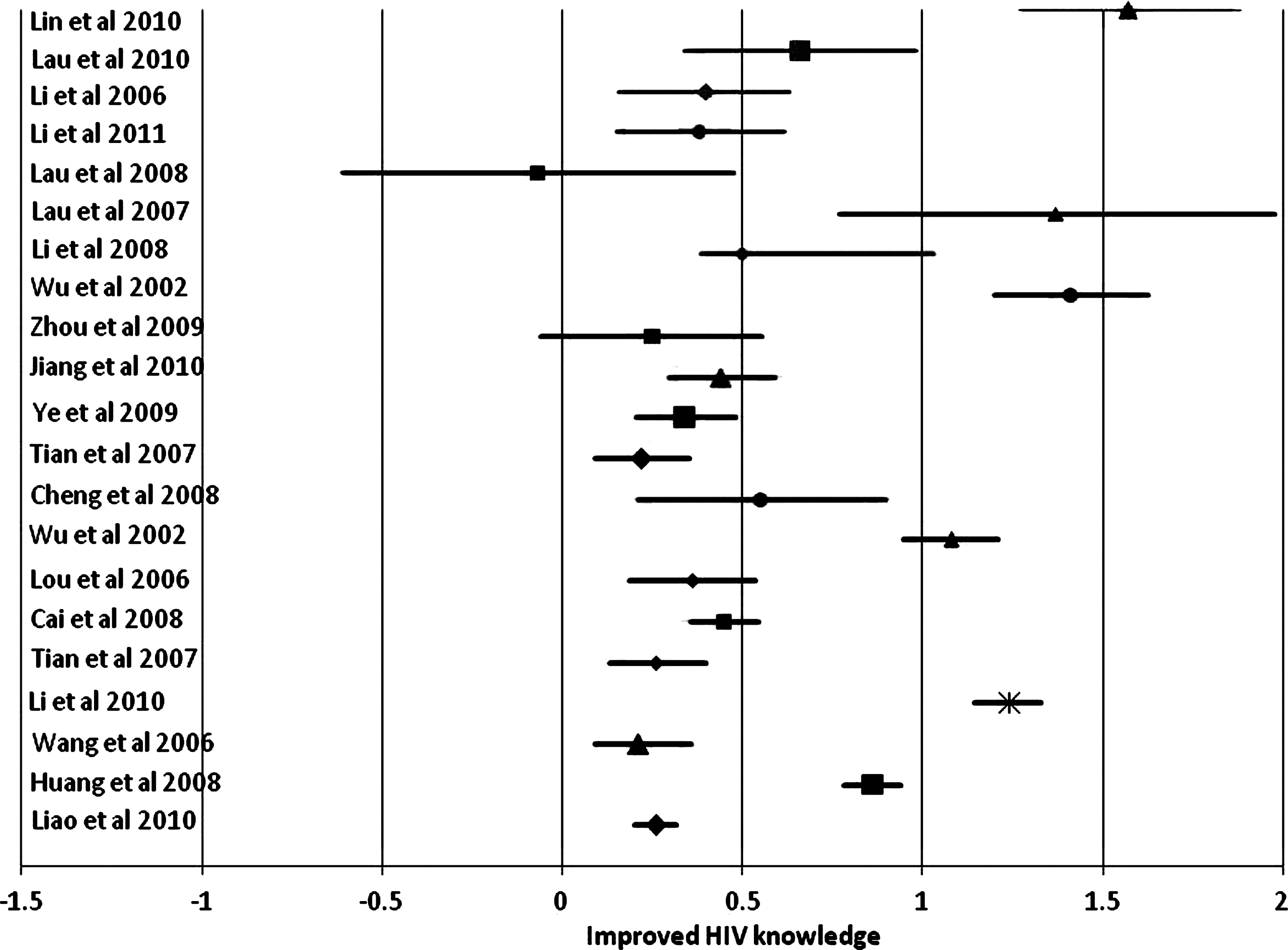
Forest plot of effect size and 95% confidence interval (CI) of the impact of interventions on HIV knowledge.
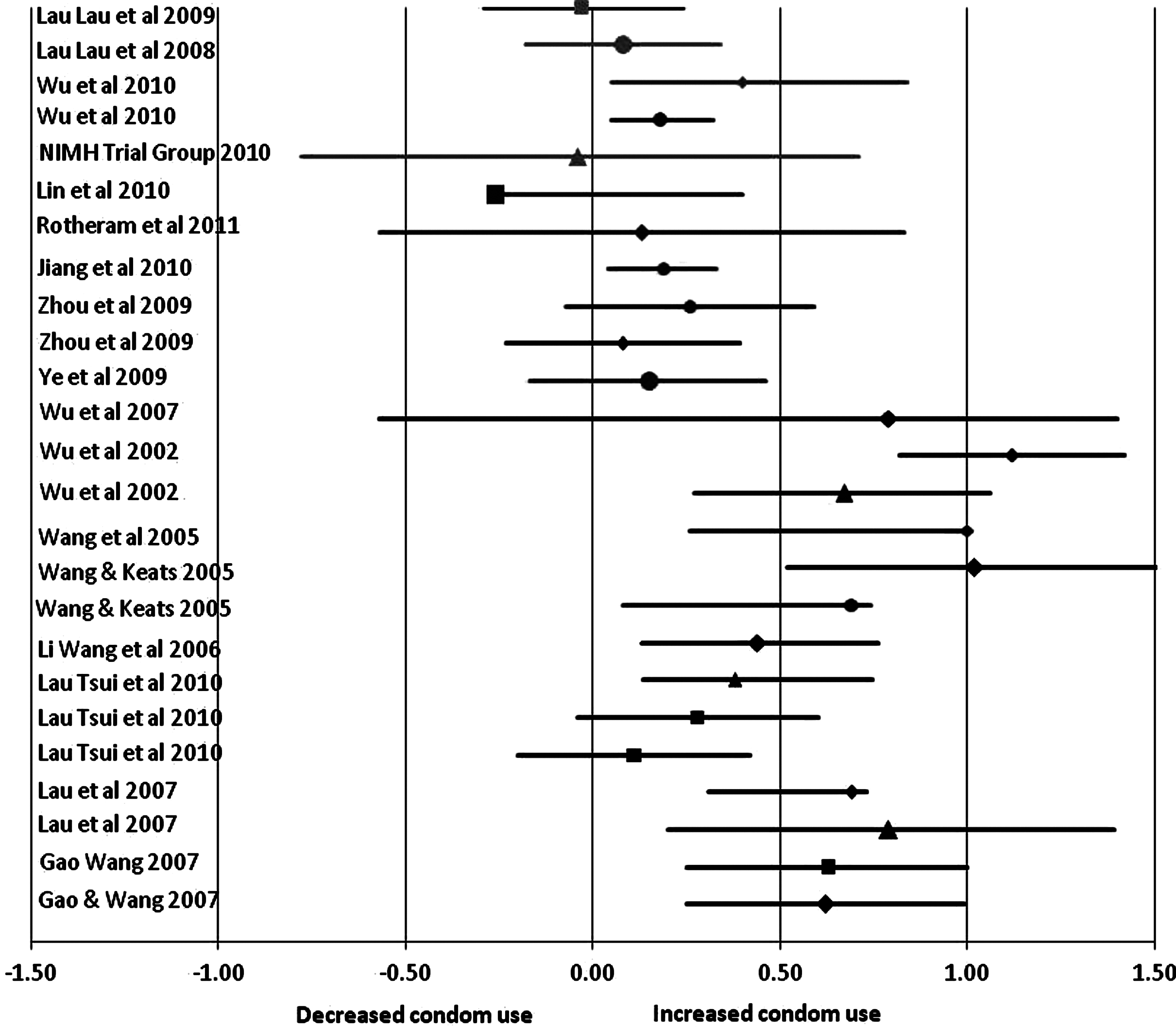
Forest plot of effect size and 95% confidence interval (CI) of the impact of interventions on condom use.
p<0.001.
p<0.01.
p<0.05.
CI, confidence interval; PLWHA, people living with HIV/AIDS; STD, sexually transmitted disease.
Publication bias
Visual inspections of the funnel plots did not show obvious evidence of asymmetry in funnel plots of the effect sizes of the interventions for HIV knowledge (Fig. 3) and condom use (Fig. 4). However, the Begg's 13 rank correlation test indicated a significant association between effect sizes and variances for condom use (r=0.654, p<0.001), but not for HIV knowledge (r=0.465, p=0.08). Egger and colleagues' 14 regression asymmetry test indicated that the intercept from the regression analyses was significantly different from zero for condom use (intercept=0.323, p=0.045), but not for HIV knowledge (intercept=0.303, p=0.245).
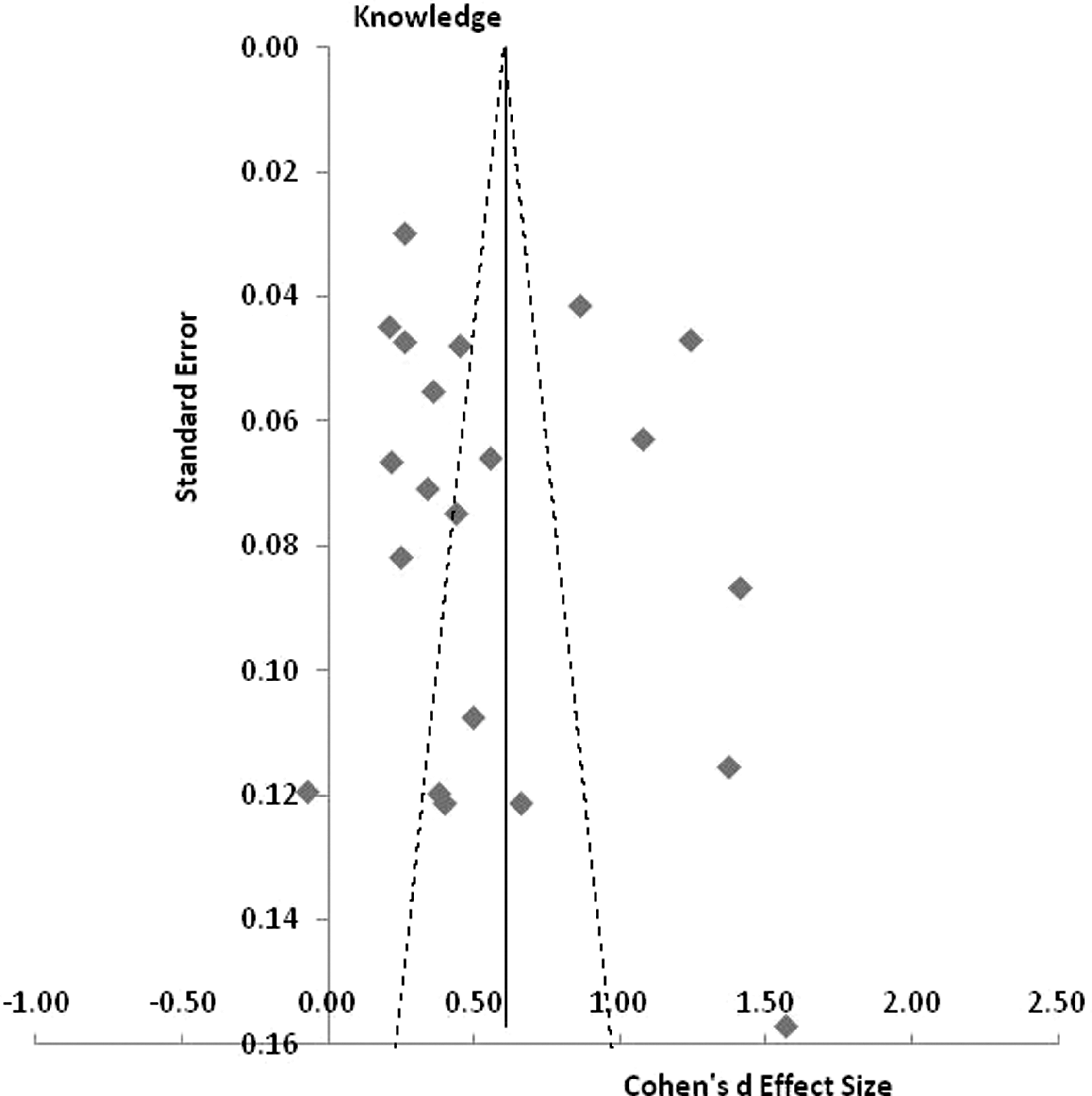
Funnel plot of Cohen's d effect size by standard error for HIV knowledge.
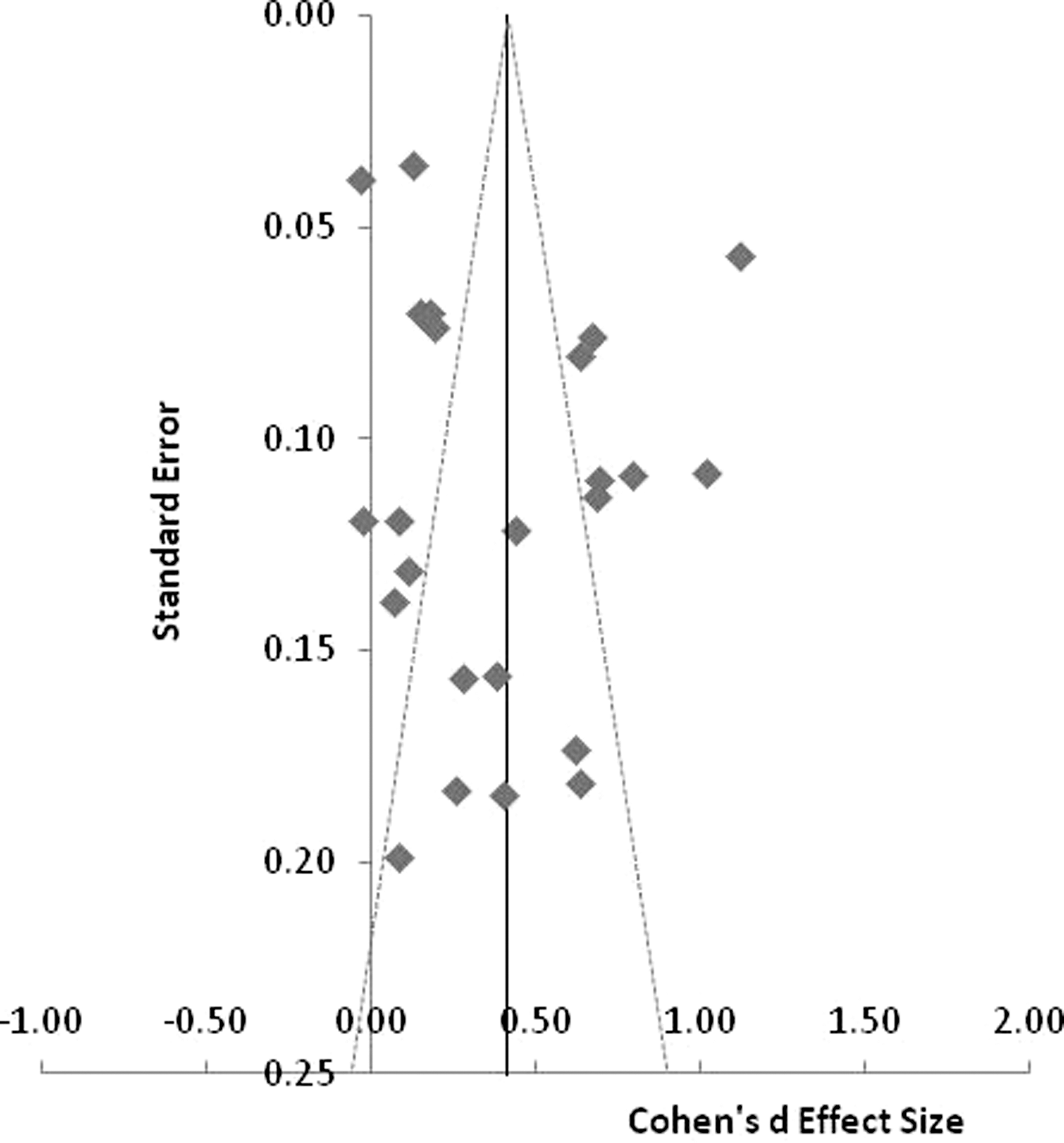
Funnel ploto Cohen's d effect size by standard error for condom use.
Moderator tests
Given the facts that HIV knowledge (κ=21), condom use (κ=25) and attitudes toward PLWHA (κ=7) were examined most frequently in the reviewed studies and the effect sizes for these three variables were heterogeneous, moderator tests were conducted on these three variables. Different categories of condom use, including condom use with regular partners, condom use with casual partners, and general condom use, were combined for the purpose of these moderating analyses. These moderating analyses help understand what characteristics of intervention design were associated with greater effects on these three outcome measures. Sample size and age of the target audience were examined for their association with effect sizes of HIV knowledge, condom use, and attitudes toward PLWHA. However, intervention effect sizes were not significantly correlated with age and sample size.
Effect sizes of three outcomes measures were examined across intervention characteristics, including inclusion of formative research (yes/no), use of a theory (yes/no), inclusion of process evaluation (yes/no), type of intervention facilitators (peer-led versus professional-led), and number of postintervention follow-up surveys (one versus two or more). As shown in Table 3, interventions that reported some type of formative research were significantly more likely than those did not report any formative research to have impacted HIV knowledge (p<0.001), attitudes toward PLWHA (p<0.001), and condom use (p<0.001). In addition, interventions that were theory-based were significantly more likely than those that used no theory to have impacted HIV knowledge (p<0.001) and attitudes toward PLWHA (p<0.001). However, theory-based interventions (d=0.353) and those used no theory (d=0.380) had similar impact on condom use (p=0.437). Interventions that reported process evaluation were significantly more likely than those that reported no process evaluation to have impacted condom use (p<0.05) and attitudes toward PLWHA (p<0.001). However, interventions that reported no process evaluations were significantly more likely to have impacted HIV knowledge (p<0.001). In addition, peer-led interventions were significantly more likely than professional-led interventions to have impacted HIV knowledge (p<0.001) and condom use (p<0.001). However, professional-led interventions were significantly more likely to have impact on attitudes toward PLWHIA (p<0.001). Finally, interventions that included one follow-up survey were significantly more likely than those that included more than one follow-up surveys to report a significant impact on HIV knowledge (p<0.001), condom use (p<0.001) and attitudes toward PLWHIA (p<0.001).
p<0.001
PLWHA, people living with HIV/AIDS; CI, confidence interval
Discussion
Because of the magnitude of the HIV epidemic in China, numbers of HIV/sexual risk reduction interventions to promote behavior change among at-risk Chinese populations have been increasing during the past decade. However, very little quantitative research has examined the efficacy of these interventions. The purpose of this study was therefore to conduct a meta-analysis of the efficacy of educational, psychosocial, or behavioral interventions to promote HIV/sexual risk reduction in China.
Overall, the results of this meta-analysis revealed that the interventions reviewed were successful in improving HIV knowledge, condom knowledge, attitudes toward PLWHA, and in increasing condom use and condom use self-efficacy. The results were consistent for all outcome measures. While the exiting primary interventions have targeted a variety of populations, including both high- and low-risk groups, more efforts are needed in the future to focus on the most-at-risk populations such as MSM, female sex workers, and migrants to effectively curtail the HIV epidemic in China.
Approximately one third of the studies reported conducting formative evaluation research and those interventions that reported the conduction of formative research were more likely to have influenced HIV knowledge, attitudes toward PLWHA, and condom use behaviors among target audience. These findings are consistent with the recommendations in the field of HIV prevention. 52 Future intervention studies in China should recognize the importance of conducting and reporting formative evaluation research. Formative research allows researchers to investigate potential barriers and facilitators among target audience for intervention adoption, obtain input from participants regarding the content, design, and delivery modality of the intervention, and optimize the feasibility, acceptability, and efficacy of interventions. 53 –55 Formative research usually presents the first opportunity for the researchers to interact with study communities, so it can help investigators to establish collaborative partnerships with the communities and participants. 56
Similarly, interventions that reported process evaluations were more likely to have a positive impact on condom use and attitudes toward PLWHA. This finding was consistent with previous studies in other cultural settings. 57,58 However, the current study found that process evaluation was not significantly associated with improved HIV knowledge. One possible problem with the data on process evaluation in the current review was the lack of specific information on the nature and scope of the process evaluation. Future research is needed to examine this issue more closely by examine the type/scope of process evaluation activities that could be more influential on outcome variables, and more useful in improving the efficacy of HIV intervention prevention programs.
Approximately one third of the interventions in the current review were theory-based. According to Cappella, 59 behavioral theories, when properly applied, allow researchers to identify the determinants that influence a behavior change among a given target audience. Likewise, information processing theories, 60 and message effects theories 61 can help make intervention messages more persuasive. Through moderating analyses, this review did find evidence that theory-guided interventions had stronger effects on outcome measures such as HIV knowledge and attitudes toward PLWHA compared with non-theory–guided studies. However, the current study found that theory-guided interventions do not have stronger effects on condom use behavior than non-theory–based studies, which is not consistent with previous literature. 62 One possible explanation is that some of the theories and models reported might not be the appropriate theories to study the change of condom use behavior or make intervention messages more persuasive in this regard. Another possible explanation is that the short duration of follow-up (e.g., 6-month) for most of these interventions was not sufficient to observe a significant change in behavior, although the intervention may indeed be efficacious in changing the condom use behavior. The third possible explanation is that most of these theories and models were originally developed in Western countries and they might not be optimal in changing condom use behavior among some Chinese populations, who may be quite different in attitudes and beliefs in terms of sexuality and condom use behavior. Given the fact that theory-based interventions have been demonstrated to be more effective in achieving intervention goals in multiple cultural settings across the global, 63 future HIV prevention efforts in China should integrate theories of behavior change, information processing and message effects into development of intervention programs, whenever feasible and appropriate. However, these theories and models should be specifically developed or culturally adapted for Chinese populations.
The data in the current study suggested that peer-led interventions might be more effective than professional-led interventions in improving HIV knowledge and condom use, while professional-led interventions were more effective in changing attitudes toward PLWHIA. Peer-based HIV risk reduction interventions have shown effects among young people and students in other countries 64 –66 and MSM 67 because of the normative influence of peers on decision-making. 66 For the same reason, peer-led interventions might be more effective in China for youth, students, MSM, or other populations to whom a clear peer social circle or social network can be well defined. Likewise, because of the authority-oriented culture in China in which individuals are inclined to defer to authority figures including persons who hold a higher social status and/or who possess greater knowledge, professional-led interventions could therefore better impact the decision-making process of individuals regarding their behavior and attitudes, especially those who have a low socioeconomic status or were low-educated. Future studies need to test the impact of various intervention facilitators in Chinese setting so we can maximize the intervention effect.
Finally, this study suggests that interventions that included only one follow-up survey had significant larger effects on improving HIV knowledge, attitudes toward PLWHA, and condom use than those included two follow-ups. This finding suggests a short-term effect for most of the interventions and also a possible decay of intervention effect over a longer period of follow-up. Future efforts are needed to develop interventions that can demonstrate a long-term effect and be sustainable over time.
Several limitations of the current meta-analysis should be noted. First, there were only 26 studies qualified for this meta-analysis, and even smaller number for most of the effect size calculations, which limits the accuracy of weighted mean effect sizes for some outcome measures such as condom knowledge, different measures of condom use, condom self-efficacy, intentions of condom use, and others. Second, due to the small sample size, moderator tests were limited to three outcome measures. In addition, the small sample size also made it unfeasible to conduct analysis on some important moderators such as target populations. Third, the current review only included published studies and only English publications. While such inclusion criteria were justified based on the access concern, we might have missed some studies/reports that also reported the efficacy of relevant interventions in China. In addition, some studies might remain unpublished due to nonsignificant findings, therefore, the so-called file drawer problem or publication bias 7 might exist in this study. Fourth, some of the studies in the review did not provide sufficient information on some of the outcome measures (e.g., attitude toward HIV) or key design characteristics (e.g., dose of intervention exposure). In conclusion, this meta-analysis provides encouraging preliminary evidence that HIV prevention/sexual risk reduction interventions conducted in China improved HIV knowledge, condom knowledge, attitudes toward PLWHA among target audience. Also, these intervention significantly increased condom use and condom use self-efficacy among target audience. These studies support the use or adaptation of psychosocial, educational, and behavioral interventions targeting various at-risk or vulnerable populations in China. Future research is needed to improve the feasibility and efficacy of the interventions by employing a culturally appropriate theoretical or conceptual framework, employing a rigorous research design and methodology including formative research and process evaluation, and targeting factors at both individual and community levels. Future research also needs to develop interventions that will demonstrate a long-term and sustainable effect among various populations across different settings in China.
Footnotes
Author Disclosure Statement
No competing financial interests exist.