
Abstract
Indian truck drivers and their younger apprentice drivers are at increased risk of HIV infection. We determine network and risk practices associated with willingness to adopt HIV prevention interventions currently not being used in India: rapid HIV testing, circumcision, and preexposure prophylaxis (PrEP) in order to inform the National AIDS Control Program (NACP). Truck drivers and truck cleaners were systematically recruited to participate in a social network and risk survey in Hyderabad, Southern India. Three separate composite measures of acceptability of rapid HIV testing, circumcision, and PrEP acceptability were utilized to independently assess the relationship of these prevention interventions with risk-practices and social network characteristics. An 89% participation rate yielded 1602 truck drivers and truck cleaners with 54.2% younger than 30 years of age and 2.8% HIV infected. Twenty-five percent of respondents reported sex with female sex workers (FSW) and 5% with men (MSM). Rapid testing, circumcision, and PrEP acceptability were 97.4%, 9.1%, and 85.9%, respectively. Participants reporting prosocial network characteristics were more accepting of rapid testing (adjusted odds ratio [AORs] 3.07–6.71; p<0.05) and demonstrated variable PrEP acceptability (AORs 0.08–2.22; p<0.001). Sex with FSWs was associated with PrEP acceptability (AOR 4.27; p<0.001); sex with MSM was associated with circumcision acceptability only (AOR 2.66; p<0.01). Social network factors and risk-practices were associated with novel prevention acceptability, but not consistently across intervention type and with variable directionality. The NACP will need to consider that intervention uptake may likely be most successful when efforts are targeted to individuals with specific behavior and social network characteristics.
Introduction
Individual's perceptions of specific risk practices may influence prevention behavior (e.g., condom use, 11 microbicides 12 ). A major component of several health behavior change models is that existing risk practices and the knowledge of these practices are critical to behavior change. For example, the AIDS Risk Reduction Model (ARRM) posits that the perception of risk leads to labeling and initial commitment for HIV prevention behavior. 13 Because there are individual, social, and structural variables that affect risk and risk perception, it is possible that high-risk persons from the same subpopulation may prefer different prevention modalities. It is important to understand the factors that influence the acceptability of each modality so that public health officials can make informed choices about which programs to prioritize.
With respect to social networks, it is well understood that social networks influence individuals' behaviors, and that changing the norms of the network can be effective in changing risk and prevention behaviors. 14 Social network analysis provides a framework for which difficult to quantify social norms can be conceptualized, and provides further guidance to prevention scientists as to which individuals might be targeted based upon their network structure and the avenues by which targeting might occur. 10 Previous studies have examined the relationship between social networks, risk behavior and HIV status. 15 –17 Some research has examined the role of social networks and HIV prevention behavior, 14,18 however, examination of the relationship between social networks (e,g., composition, tie quality) and novel prevention interventions is unstudied.
In this study, we examine the relationship between several social network characteristics, risk practices, and willingness to accept rapid testing for HIV, circumcision, and PrEP. We focus on India, a setting where there is a large, well-established ongoing epidemic, with over 2.5 million infected persons. National surveillance has established that HIV/AIDS is spreading most rapidly among men who have sex with men and injection drug users and other large subpopulations such as truck drivers and internal migrants who are at increased risk because of their mobility and access to sex workers at major transit areas. 19 We focus specifically on truck drivers sampled from the state of Andhra Pradesh because of the 10 to 20 times higher HIV prevalence among truck drivers compared to the general adult Indian male population, 20,21 a noticeable paucity of HIV prevention interventions for truck drivers, 22 –24 and because this state has the highest numbers of HIV infected in India. 25,26 Because the three modalities are currently not yet approved for HIV prevention in India, we could not focus on adoption and use, so we sought to better understand the relationship between social networks, risk practices and the acceptability of interventions that might be effective in this context 8 in order to inform National AIDS Control Program (NACP) HIV prevention programming in this and potentially other high-risk male populations.
Methods
Participants and setting
This study was conducted from 2010 to 2011 at the intersection of two national highways in Hyderabad, Andhra Pradesh, India. Both truck drivers and young apprentice drivers (cleaners) between the ages of 16 and 65 were recruited in a proportional manner from 12 locations within 4 areas near entry points into the city. Trucks parked at these locations were approached in a systematic manner with information on eligible nonparticipants recorded. Truck drivers and cleaners who understood either Telugu or Hindi were eligible for participation. Of eligible truck drivers and cleaners, 7 truck drivers and 3 cleaners were randomly selected to be interviewed each day. A 60-min face-to-face survey was administered.
Survey
Sociodemographic and HIV risk measures
Sociodemographic and risk measures were based upon previous surveys used in this population and setting 21,25,27 ; made available in English, Hindi, and Telugu; pretested, and extensively analyzed to ensure equivalence of different language versions and appropriateness for low literacy participants. Measures included sociodemographic characteristics, work and lifestyle characteristics, sex behavior, HIV/sexually transmitted infection (STI) knowledge and access to services. Caste categories as designated by the Indian Government were utilized and included a hierarchy of “Forward caste,” “Backwards caste,” “Scheduled caste,” and “Scheduled tribe.”
Social network measures
In designing our social network instrument, we followed an established method of gathering network data that is used in several large national surveys, including the General Social Survey, 28 the National Health and Social Life Survey, 29 and the National Social Life, Health, and Aging Project. 30 Based upon formative work in India, 31 we modified this approach by asking about information on “close friends” instead of “confidants,” and limited the expanded information on these friends (e.g., sociodemographics, perception of risk, discussion topics) to the two closest friends within the network. Thus respondents identified whether they had “a few friends” or “lots of friends,” then estimated the number of close friends and finally identified their two closest friends. Detailed information on the two closest friends included: level of closeness, frequency of communication, closeness of friend to the respondent's family, importance of advice and opinions to the respondent, discussion of sexual matters, importance of advice and opinions to the respondent on sexual matters, friend's history of a sexually transmitted disease, and whether the respondent would consider getting an HIV test if the friend were getting an HIV test. This approach of elicitation follows previous work 32 and for the primary analysis was operationalized as to whether at least one of the friends was categorized in this way (e.g., at least one of the friends is very close, at least one of the friends communicated at least daily, etc.).
Rapid testing, circumcision, and PrEP measures
Several measures of novel HIV prevention intervention knowledge, use and acceptability exist, 33 –36 however, they are often limited by a general inability to assess for participant comprehension of these interventions, many of which participants may not have never heard of previously. We utilized a standardized paragraph tailored to each of the three interventions (rapid testing, circumcision, and PrEP) and implemented a teach-back approach to assess for comprehension. 37 Teach-back is an iterative communication strategy in which the interviewer checks for comprehension by asking participants to repeat, in their own words, what they know about the intervention. Experts have proposed teach-back as a useful tool for improving understanding of health information by patients, for example, with low literacy. 37 Interviewers did not proceed with acceptability items until three prespecified core concepts about each intervention were explained by the respondent. We developed our acceptability measures starting with existing acceptability measures for novel prevention intervention 33 and modified them based upon formative work with this population. 31 The resulting acceptability items were each based on four-point Likert scales. Respondents rated their likelihood of (1) trying to get more information about the intervention, (2) considering obtaining the intervention, (3) obtaining the intervention if it were provided for free, (4) obtaining the intervention if they had to pay, and (5) advising their friends to obtain the intervention; with each domain rated on a scale from 1–4 as “very unlikely” (1), “unlikely” (2), “likely” (3), and “very likely” (4). Mean scores across each set of five items (range of 1–4) were calculated for each intervention separately, and then dichotomized as very unlikely/unlikely (<2.5) and likely/very likely (>2.5) resulting in a summary measure for each of the three interventions. In addition, respondents were asked to identify PrEP delivery method preferred; either daily (1 pill once daily) or intermittent (1 pill 1–2 days before sex and daily for 28 days afterwards).
Blood samples
Dry blood spots (DBS) were collected using a validated finger-prick method with a safety lancet and prepared on Whatman No. 3 paper according to procedures utilized previously. 38 –40 Three sequential HIV antibody tests were conducted according to NACO guidelines 41 using standard methods and kits (Vironostika HIV Uni-Form Ag/Ab, bioMerieux, France; Vidas HIV Duo Ultra; bioMerieux, France; and HIV Tridot; J. Mitra, New Delhi, India). HSV-2 IgG (HerpeSelect 2 ELISA IgG, Focus Diagnostics, CA) and Treponemal pallidum IgG (Treponostika sandwich ELISA, bioMerieux, France) testing was also conducted as in previous work. 42
Analysis
Descriptive statistics for the total sample and stratified by truck-driver/cleaner status are reported. Cronbach α was calculated for the five acceptability items within each of the three interventions. We examined the relationship of intervention acceptability and social network characteristics in separate bivariate analyses for each intervention. We then utilized a stepwise approach by creating three separate initial logistic regression models for rapid test, circumcision, and PrEP acceptability that included other sociodemographic, risk and HIV/STI serostatus variables significant at the p<0.05 level from bivariate analysis. Variables that remained statistically significant in the initial regression analyses were then combined into a final multiple logistic regression model for each of the three interventions separately. Truck driver status (truck driver or cleaner) was forced into all final models. Analyses were performed using STATA software version 11.0 (StataCorp, Austin, TX).
Ethical considerations
The protocol was approved by the Indian Council of Medical Research (ICMR), the National AIDS Control Organization (NACO), and institutional ethics panels in India and the United States. All study participants provided written informed consent and received a gift worth 120 Indian Rupees (∼$3 USD) for participation.
Results
Respondent characteristics
Of the 1800 eligible truck-drivers and cleaners we achieved an 89% participation rate (Fig. 1) for a total of 1602 respondents. Table 1 depicts relevant sociodemographic, risk, and serostatus characteristics.
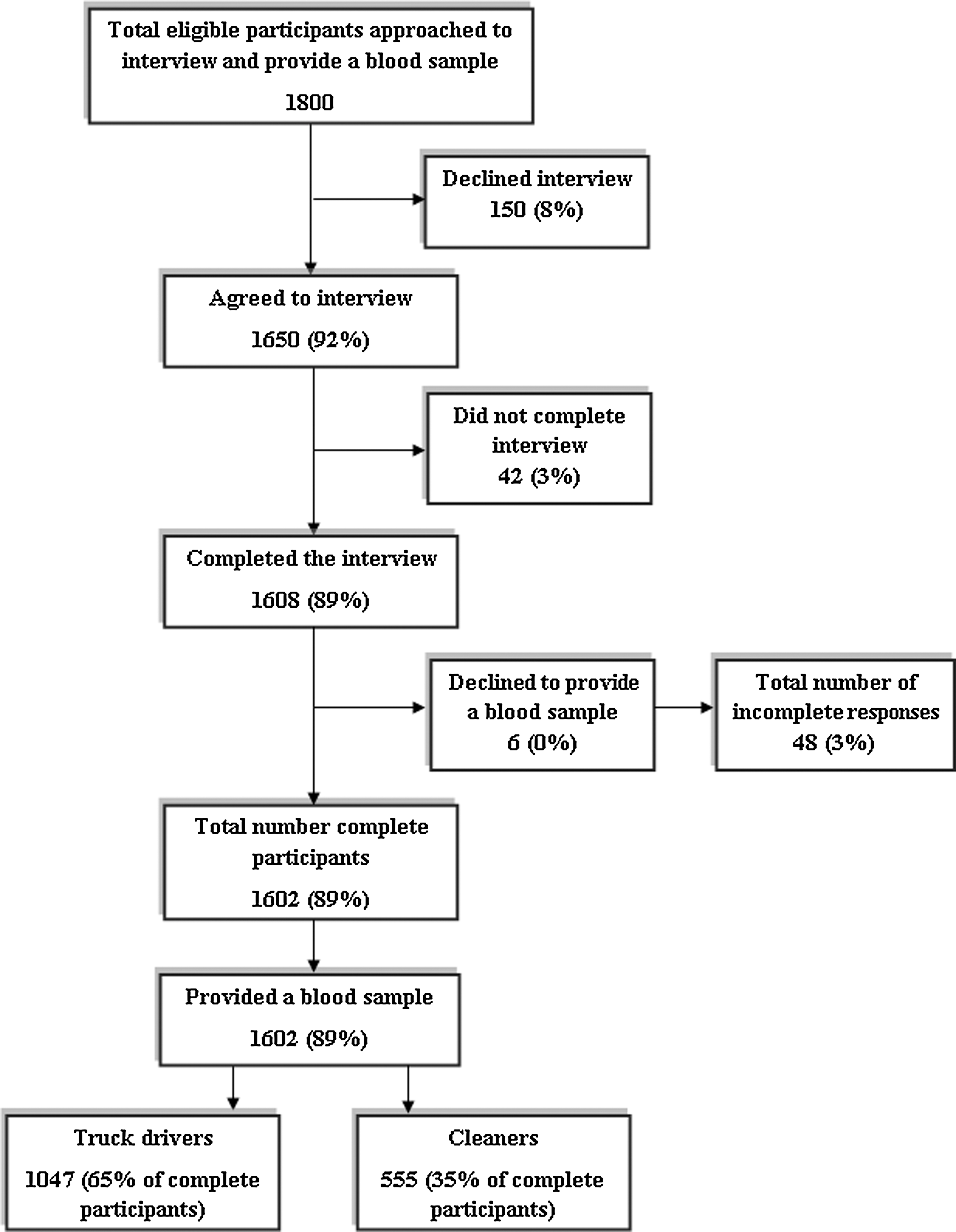
Enrollment and participation.
Indian Government designation in hierarchical order.
Social network characteristics and intervention acceptability
There was excellent internal consistency for acceptability items across each of the three interventions (Cronbach α=0.96–0.98). Figure 2 depicts acceptability of rapid testing, circumcision, and PrEP. High acceptance of rapid testing was reported by respondents: only 2.6% (42) were unlikely to accept such testing. Among uncircumcised participants, however, only 9.1% (113) were likely to be accepting of circumcision. For PrEP, 85.9% (1376) of study participants were likely to be accepting, however, a pericoital formulation was preferred to a once-daily PrEP formulation among 57.5% (800) of those likely to accept PrEP and 97.4% (222) of those unlikely to accept PrEP. Table 2 depicts the distribution of social network characteristics for respondents.
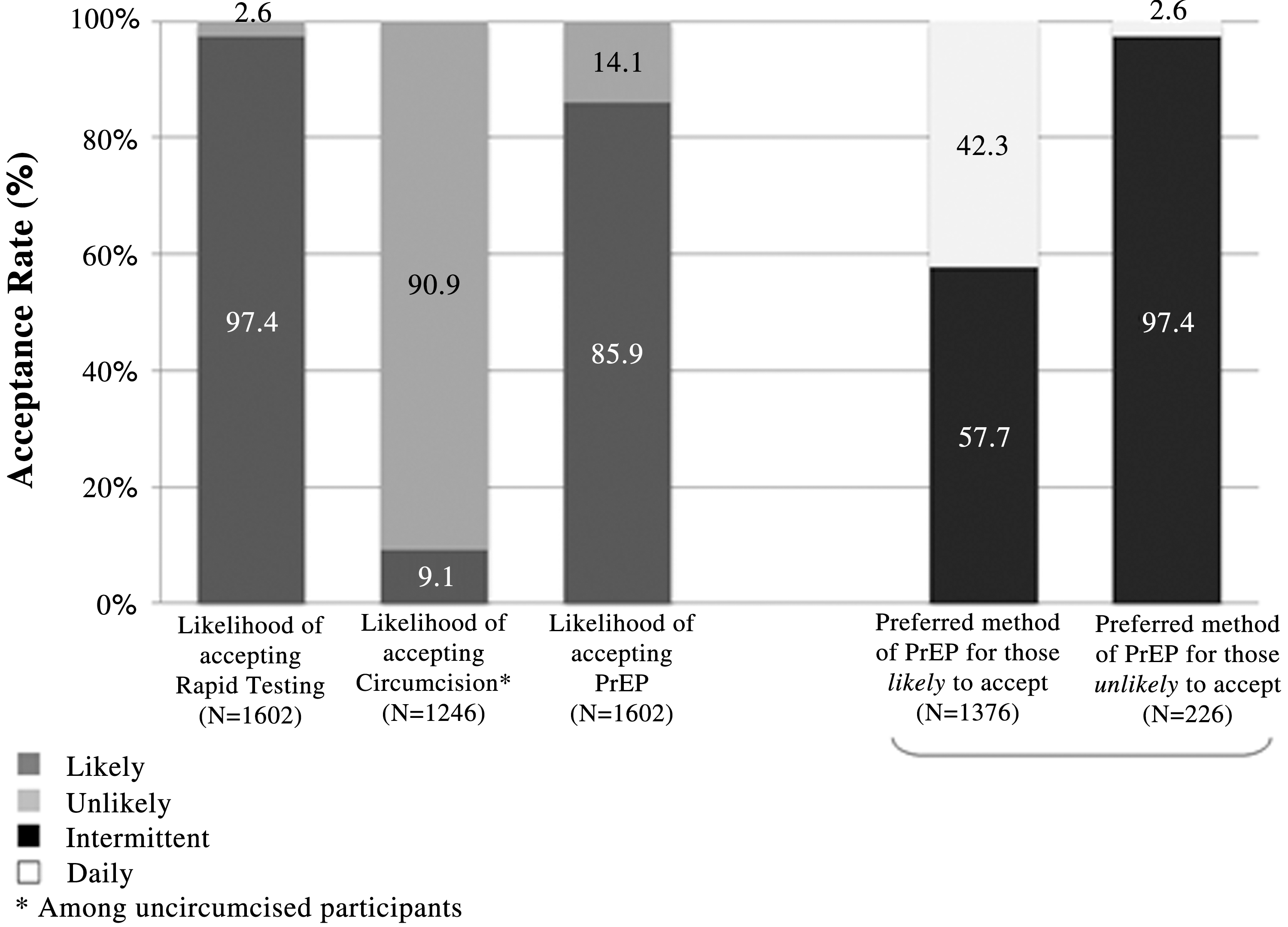
Novel prevention intervention acceptability among Indian truck drivers and cleaners (n=1602).
Risk practices, social network characteristics, and intervention acceptability
Bivariate analysis with the following variables were associated with significantly increased odds of accepting rapid testing (p<0.05): current alcohol use, more than one female sex partner, sex with female sex worker in past 6 months, having many friends, friend closeness, daily communication, importance of friend advice, discussing sexual matters with friend, importance of friend advice on sex behavior, and considering HIV testing if friend was tested. Married status, Christian religion and traveling on a southeastern route were associated with significantly decreased odds of accepting rapid HIV testing in bivariate analysis (all p<0.05).
For circumcision acceptability, the following variables were significantly associated with increased odds of accepting circumcision in bivariate analysis (p<0.05): Christian religion, history of sex with men, daily communication with friend and friend closeness to family. Married, Backwards caste status and traveling on the southeastern route resulted in significantly lower odds of accepting circumcision.
Bivariate analysis with the following variables were significantly associated with increased odds of accepting PrEP (p<0.05): 20–24 age range, current alcohol use, alcohol use prior to sex, current drug use, more than 1 female partner in past 6 months, last female partner as nonwife, history of sex with men, and friend closeness. Low-middle and high income levels, traveling on a southeastern route, having many friends, daily communication with a friend, and closeness of friend to respondent's family, were associated with decreased odds of accepting PrEP.
Table 3 depicts three final multivariate models based upon a stepwise approach that include variables significant from at the p<0.05 level from both bivariate and initial multivariate models. Participants reporting prosocial network characteristics were more accepting of rapid testing (adjusted odds ratios [AORs] 3.07–6.71; p<0.05) and with variable acceptability of PrEP (AORs 0.08–2.22; p<0.001). Sex with FSWs was associated with PrEP acceptability (AOR 4.27; p<0.001), whereas sex with MSM was associated with circumcision acceptability only (AOR 2.66; p<0.01).
Variables included in rapid HIV test acceptability final multivariate model: number of close friends, friend closeness, advice of friends being important, discussing sexual matters with friends, current alcohol use; variables included in PrEP Acceptability final multivariate model: friend closeness, daily communication with friend, sex with FSW, religion, monthly income; variables included in circumcision acceptability final multivariate model: daily communication with friend, friend close to respondent's family, ever sex with man, marital status, religion, caste type, and route. All three final multivariate models included truck driver vs. cleaner status.
Data missing: 17 for caste type, 3 for sex with female sex worker, 1 for number of close friends, 1 for being very close to friends, 1 for talkin g daily to friends, 1 for advice/opinions of friends, 1 for discussing sexual matters with friends, 2 for closeness of friend to respondent's family.
Only among uncircumcised (n=1246).
p<0.05.
p<0.001.
p<0.01.
PrEP, preexposure prophylaxis; AOR, adjusted odds ratio; CI, confidence interval.
Discussion
Over the past few years there has been a substantial increase in the number and diversity of biomedical interventions available ranging from adult male circumcision to PrEP, earlier initiation of antiretroviral therapy; all of which require increased uptake of HIV testing to appropriately determine optimal strategies. 43 The current study illuminates several important factors that are likely to influence novel prevention intervention acceptability among at risk Indian men. We found that acceptability of rapid testing was high, PrEP was accepted by most study participants—with a pericoital strategy preferred—and circumcision was generally unacceptable. Additionally, several social network factors were associated with prevention intervention acceptability. Prosocial factors were generally associated with prevention intervention acceptability for rapid testing and circumcision. Acceptability of rapid testing for example, was associated with having more close friends, having a very close friend, communicating daily with friends, feeling that friend advice is important and discussing sexual matters with friends. Finally, we found that the level of risk taking did not predict acceptability of most of the prevention interventions with the exception that individuals who were riskier had favorable attitudes of PrEP, but the only predictor of circumcision acceptability was prior history of sex with a man.
Although rapid testing was found to be highly acceptable which replicates previous work in this setting, 44,45 overall rates of adults tested and who receive their results in India are some of the lowest in the world at 10.8%. 46 These findings suggest that low rates of testing may reflect insufficient public health promotion of testing as part of comprehensive HIV prevention strategies. Strategies to decrease barriers to HIV testing in this highly mobile and at risk population are urgently needed given that only 19% of the sample overall and 8.8% of cleaners had ever received an HIV test previously.
In the case of PrEP, overall acceptability was much higher at 85.6% than in previous work with this population where initial willingness to consider PrEP was only 32.9%. 8 The reason for this may be due to differences in data collection methods utilized, analytic methods employed, changes in PrEP attitudes over time, or perhaps increasing use of antiretroviral medications for treatment over time in this context. For example, the study by Schneider et al. 8 utilized qualitative interviews for data collection with subsequent analysis of one acceptability item and a willingness to pay application that differed from the acceptability analysis utilized in this study. Prior studies have suggested that Indian patient satisfaction is enhanced when medications are offered by their physicians 47 –49 that would tend to corroborate oral prophylaxis as one of the more attractive prevention interventions in this study. However, considerable challenges remain requiring additional investigation such as the concept of taking pills long term, which often clashes with the symptomatic disease model in India in which patients often decide that they do not need medications when they feel well. 50 The finding in this study of a general preference for pericoital dosing of PrEP may alleviate concerns for long-term use of medication in a daily format. Current work is underway to determine efficacy of other PrEP formulations such as fixed intermittent or pericoital compared to daily dosing. 51 Intermittent formulations, for example, may be highly relevant for this mobile population given that they have predictably episodic risk.
Finally, the low acceptability of circumcision in this setting is not surprising. The potential for negative response due to religious connotation (in a country where being circumcised is highly predictive of being Muslim) poses a major barrier to circumcision for HIV prevention in India. 8,52 Several strata of uncircumcised men within our sample, however, were more likely to find circumcision acceptable: Christians and MSM. The finding of MSM as being more accepting of circumcision is of interest and worth further investigation. It is feasible that for some MSM circumcision may be considered as a form of cleanliness or even attractiveness, 53 however, others have found that uncircumcised partners may be preferred. 54 Studies of circumcision among MSM populations are currently underway 55 and if found to be effective, may be a population worth considering for intervention in India 56 , although use of circumcision outside of generalized epidemics would require careful examination. 57
Our findings that higher risk practices are associated with intervention acceptability follow previous findings of perceptions of risk and willingness to use PrEP or circumcision. 8 Of concern from our data is that MSM were not more likely to find rapid testing or PrEP more acceptable than heterosexual truck drivers; two interventions with proven benefit in this population. 58,59 The lack of a difference in acceptability between heterosexual truck drivers and those truck drivers who have sex with men could suggest that perception of risk for HIV is similar between the two groups. Truck driver targeted HIV behavior change communication may not include messages specific for MSM. Furthermore, we are unaware of empirical data that describes the behavior and risk practices of men who are both truck drivers and MSM.
Several of the relationships between social network characteristics and composition and acceptability of the prevention interventions are of interest. Notably, prosocial network characteristics were consistently associated with increased acceptability of rapid testing, potentially reflecting the increasingly normative nature of HIV testing in this population. Truck drivers are increasingly aware of their HIV infection risk, sometimes to the point of stigmatizing the profession. 60 However, although prosocial factors were universally associated with acceptability of testing, this was not the case with PrEP where some prosocial features were associated with less acceptability of PrEP. For example there was discordance between having at least one close friend and speaking daily with friends and PrEP acceptability. Previous work suggests that daily communication, usually by phone, is likely with individuals who reside in the truck drivers' hometown. 31 Close relationships with such individuals, who may in turn be close to truck drivers' families might affect the willingness of the participants to acknowledge their HIV risk 61 and thereby limit their willingness to consider this prevention modality as acceptable. Close relationships with such friends whose norms may not include frequent contact with female sex workers at rest stops may be a source of cognitive dissonance 62 for the respondents given their described sexual behavior when away from home. Additional research is needed to elucidate how acceptability of different prevention modalities is established in relation to the different friend typologies that exist within distinct geographic spaces of this highly mobile population. 63
Ability of social networks to influence attitudes may be a function of the invasiveness of the intervention. For things that are less intrusive such as oral testing and taking a pill, social networks may be playing a role, but for something requiring minor surgery at the individual level, social networks may not play as much of a role. In general, social network variables seemed to play a greater role in the likelihood of accepting HIV testing than in accepting PrEP, while none were significantly associated with circumcision likelihood. As the interventions become increasingly burdensome for the individual, the persuasiveness of social network effects in the individual's uptake of these interventions may diminish. Mobilizing communities to obtain HIV testing through social networks as is currently being tested (Project Accept 64 ) and may be useful in the Indian setting if it is found to be efficacious.
Respondents with higher income were less likely to find PrEP acceptable. This is similar to findings from a PrEP acceptability study in the United States where high-risk men who were less educated were more interested in PrEP. 34 Further research into the conceptual understanding of PrEP among diverse social and economic strata is required if effective adoption and adherence is to be obtained among high-risk men such as Indian truck drivers and younger apprentice drivers. Because younger apprentice drivers earn less and are less educated, they may require specific PrEP messaging and monitoring compared to their older and more experienced truck driver mentors.
Our study had several limitations. First, we focus on acceptability of HIV prevention interventions that are not yet available in India for HIV prevention in this population. However, as in other studies, initial acceptability has been shown to be linked to future behavior in multiple settings for multiple behaviors. 11,65,66 Because the interventions examined in this study are either under investigation or currently unavailable for HIV prevention in India, actual uptake of the interventions could not be assessed. Additionally, we did not directly ask respondents about behavioral disinhibition and risk compensation, and these themes will be needed to be addressed in further studies of HIV prevention interventions that are found to be modestly effective in high-risk men. Furthermore, we focused on the close social networks, and particularly friends of these truck drivers and did not measure characteristics of expanded social networks. We also did not examine other potentially useful interventions such as an HIV vaccine or the use of microbicides.
Findings from this work can be further developed in order to inform NACP policy decisions. Obtaining an understanding of the social network characteristics of various types of prevention interventions could help target resources toward the individuals most likely to benefit from them. This study has demonstrated an often robust association between social interconnectedness and willingness to accept PrEP and HIV testing in Indian truck-drivers and cleaners. Further interventions could take advantage of high-risk Indian men's interconnectedness in order to increase the uptake of HIV prevention interventions within their social networks, recognizing that uptake may also be concomitantly driven by individual risk practice and risk perception.
Footnotes
Acknowledgments
We would like to thank the field staff and study participants. This work was supported by NIH grants KL2RR025000 and P30AI42853-10.
Author Disclosure Statement
No competing financial interests exist.