
Abstract
Integration of HIV with other primary health services, including sexual and reproductive health (SRH) care, is being widely promoted in sub-Saharan Africa. However, evidence on its benefits is equivocal, and some studies indicate client preferences for stand-alone HIV services. A comparative case study investigated the relationship between integration and client satisfaction across different models of care in Swaziland: two clinics integrated with SRH services, and two stand-alone HIV clinics. An exit survey (n=602) measured satisfaction across model using logistic regression. In-depth interviews (n=22), repeated three times, explored satisfaction and how it was influenced by integration or not. Satisfaction was highest at the fully stand-alone clinic; in multivariable models, clients there were more satisfied than partially integrated and partially stand-alone sites (adjusted odds ratio [aOR] 0.45, 95% confidence interval [CI] 0.25–0.81; and aOR 0.53, 95% CI 0.31–0.90, respectively); there was no difference between the fully integrated and fully stand-alone sites. Qualitative analysis suggested that satisfaction was constituted by eleven dimensions of care, including access to HIV medication, interpersonal care, efficiency, and confidentiality. Some dimensions were positively influenced by integration, while others were positively influenced by stand-alone care; some were not influenced by integration at all. Assumptions on the inherent value of integrated care were challenged in this high HIV prevalence setting, where stand-alone HIV care could be equally if not more satisfying to many clients. Those aiming to scale-up access to HIV care in this region may need to consider providing a variety of treatment models for clients with different health care needs.
Introduction
W
Integrated SRH-HIV services are considered to have distinct advantages over stand-alone models, including greater efficiency and cost effectiveness, enhanced service access and increased utilization of separate service components, increased client satisfaction, reductions in service-related stigma through the delivery of care in more generalist health care settings, and potential improvements in health outcomes due to greater and higher quality service access. 4,6,7 Integration, to quote the Director of Joint United Nations Programme on HIV/AIDS (UNAIDS), is therefore “intuitively appealing.” 8 (p806)
However, evidence on the impact of SRH-HIV integration on these outcomes is neither robust nor extensive. 9 One area that remains particularly understudied is the impact of service integration on client satisfaction. While integration may increase satisfaction by delivering a broader range of services to clients or reducing the need for multiple queues, it may also increase dissatisfaction, for example if health workers were to become overloaded and their capacity to deliver individual service components was compromised. 10 Studies have indeed demonstrated multiple challenges for providers following service integration, often stemming from additional workload without concomitant improvements in infrastructure, working conditions, salary or career structure. 11 Following integration of SRH with HIV services, reports also demonstrate that providers continue to lack relevant technical skills, 12 –14 even following specific SRH interventions. 15 –17
Defined as an individual's subjective evaluation of service received against his or her expectations, 18 satisfaction is of particular importance due to its association with adherence to treatment, utilization of services, continuity of care and clinical outcomes, 19,20 including within HIV services. 21 It is understood to be constituted by, and usually measured over, a range of dimensions of health care including perceptions on interpersonal communication with providers; competence of providers; accessibility and convenience; costs; improvements in health; continuity of care; physical environments; and availability (e.g., sufficient drugs or providers). 19 However, attention to quality of care in HIV programming has focused on outcome measures (such as loss to follow-up, retention in care, adherence, response to therapy and mortality), 22 while users' perspectives on quality remain neglected. 23 Among the few studies that have been conducted on satisfaction within HIV care in Africa, most demonstrate high overall scores, 24 –26 in part stemming from the substantial reporting bias common with evaluations of satisfaction in health care. 27 –29 Nevertheless, differences across clinical settings remain, and evidence on the role of integration is inconclusive. A review of integration of HIV and sexually transmitted infection (STI) services into family planning services in developing countries found that clients generally reported an appreciation of accessing a broader range of services, although much of this evidence is from qualitative reports or uncontrolled observational studies. 30 More recent studies within HIV services (both qualitative and quantitative) also demonstrate that clients are satisfied when able to access a broader package of care under one roof. 31,32
However, other service attributes may be equally, if not more, important to people living with HIV (PLWH) including convenience, confidentiality, waiting times, food assistance, being treated with respect, costs, and having specialist HIV providers. 25,28,31,33 Studies in HIV settings indicate patient preferences for stand-alone HIV services, as well as concerns about decentralization of ART into primary care. 34 A comparative study in Uganda also indicated higher satisfaction within a specialist HIV unit than the general outpatient hospital unit. 35 Clients in integrated PHC-HIV clinics in Zambia, while demonstrating preferences for integrated care on the one hand, also had concerns about increased waiting times. 36
This study therefore aimed to evaluate the relationship between service integration and client satisfaction in a setting where decisions about HIV treatment models are of great importance. Swaziland suffers from the world's highest HIV prevalence (26% among adults), 37 and while there have been rapid increases in the numbers of clients on ART in the past 7 years, 38 gaps in coverage remain (in particular in reaching men) and more than one third of clients are lost to follow-up within the first 12 months of initiation. 39 The study formed one part of a broader comparative case study investigating the process and outcomes of integrating SRH and HIV services in Swaziland, 40 and this in turn forms a subcomponent of a multicountry study aiming to investigate the benefits and costs of service integration in sub-Saharan Africa, the Integra Initiative. 41
Methods
Design and setting
A comparative case study of four clinics offering HIV treatment services in Manzini town in Swaziland investigated satisfaction with integrated and stand-alone models of care. Quantitative methods measured differences in satisfaction scores across facility, while qualitative methods explored whether these differences were attributable to the model of care (integrated versus stand-alone), or rather to other aspects of HIV service delivery. By triangulating quantitative and qualitative methods within a case study approach, the study aimed to overcome some of the methodological limitations of many evaluative studies on service integration, which often fail to identify the causal pathways (process) through which a model of care impacts on client outcomes measured. 42,43
The clinics were identified purposively to represent a specific model of integrated SRH-HIV or stand-alone HIV service delivery accessible to the same geographic catchment population (all provided ART free of charge). The sites were the only HIV care facilities operational in Manzini at the time of the study, and represented a continuum of service integration (Table 1): Clinic A, the most integrated site, offered ART together in the same consultation room as other SRH services (fully integrated); Clinic B offered ART in the same building as other SRH services (partially integrated); Clinic C offered ART in a stand-alone outpatient clinic located on a hospital campus (partially stand-alone); and Clinic D offered only ART and HIV testing services (fully stand-alone). The degree of integration at each clinic and the designation of the models was evaluated using a clinic characteristics review form, completed through interviews with clinic staff and observations of clinic structure and process of care by the research team.
Other staff also onsite at all clinics included lay counselors, lab technicians, pharmacists, receptionists and data management clerks.
FP, family planning; STI, sexually transmitted infections; ANC, antenatal care; MCH, maternal and child health; PMTCT, prevention of mother-to-child transmission services; PNC, postnatal care; VCT, voluntary counseling and testing of HIV; SRH, sexual and reproductive health; NGO, nongovernmental organization; ART, antiretroviral therapy.
Quantitative methods
An exit survey was conducted among HIV care clients (n=602) (either pre-ART or on ART), aged 18 or over, in order to measure dimensions of satisfaction that were pre-identified in the literature and through baseline qualitative research with clients and providers, as well as preferences for integrated and/or stand-alone HV care. It was hypothesized that aggregate mean satisfaction scores would be higher at integrated sites than stand-alone sites. A conceptual model was developed based on the literature and knowledge of the research context to determine potentially confounding variables influencing satisfaction outcomes, including socioeconomic, geographic, and health-related factors, as well as preexisting client concerns about confidentiality.
A questionnaire was administered following each client's completion of service contacts at the clinic. Systematic random sampling was used to identify clients exiting the facilities, with sampling intervals based on clinic client load and interviewer capacity. Refusals were documented by fieldworkers. The following measures related to satisfaction were recorded. Respondents were firstly asked to state the reasons they chose to attend their clinic (through a free-list rather than predefined categories). A single-item Likert scale score (1 to 5) also evaluated preferences for specialist HIV services, with an agreement rating on the statement “HIV services should be separated from other health services.” Satisfaction was also measured with scales across the nine dimensions shown in Table 2, then aggregated into a mean overall satisfaction score. These dimensions were taken directly from other instruments in the Integra study, and were left untouched to ensure cross-model and cross-country comparisons. Their reliability as a scale was tested with Cronbach α coefficient (0.68). While median scores would have been a more appropriate measure of central tendency for these skewed data, means were compared in order to identify small differences between clinics. Bias arising from skewed score distributions should be consistent across sites. Differences in scores across clinics were tested with the analysis of variance (ANOVA) test and between clinics with the postestimation Tukey-Kramer pairwise comparison. Due to substantial end skew in the scaled data, the aggregate mean satisfaction score was categorized into a binary variable (score ≥4/5) in order to test the primary hypothesis using regression techniques.
Statistical analysis was conducted using STATA 10.0 (StataCorp, College Station, TX). A crude analysis examined the association between the key exposure (clinic model) and aggregate satisfaction score, as well as between potential confounders and both exposure and outcome, using the χ2 test for categorical variables, or ANOVA for continuous variables. Stratum-specific odds ratios of the association between clinic model and satisfaction were tabulated across potential confounders in a bivariate analysis, using the Mantel-Haenszel method: no significant interaction was identified. Multivariable logistic regression modeling was used to analyze the association between clinic model and overall satisfaction score. A parsimonious regression model was identified via backward-fitting regression techniques and confirmed using forward-fitting regression techniques (using the likelihood ratio test).
Qualitative methods
In-depth interviews (IDIs) were conducted with 22 clients (5–7 per clinic), interviewed at three points in time: on the day of ART initiation, and then with a 2- and 6-month follow-up. Clients were sampled both purposively and opportunistically: they were invited to interview during group counseling sessions or by adherence counselors, with the aim to reach at least 5 per site, but with potential for more if data saturation was not achieved; those exiting consultations first and/or when interviewers were available were interviewed, though efforts were made to ensure at least 2 men and 1 pregnant woman were interviewed per clinic. IDIs were conducted in SiSwati, either at the clinic (round 1) or at a local NGO or participant's home (rounds 2 and 3). Interviews were recorded, transcribed, and translated into English. Data were analyzed through an iterative process, including stages of (1) data familiarization, through transcript review; (2) development of coding framework (using NVivo 8.0), derived deductively from the research questions and inductively from the data; (3) abstraction of coded data into thematic matrices, allowing a constant comparative approach 44 across clinics and cases; and (4) interpretation, methodological synthesis and write-up.
Ethical approval and procedures
Ethical approval for the study was obtained from the Ethical Committee at LSHTM (approval no. 5436) and from the Swaziland Scientific and Ethics Committee (approval no. MH/139).
Results
The quantitative sample
Table 3 presents the key characteristics of the survey sample, by clinic, which was composed of 602 clients; 127 male and 475 female. The refusal rate (15.3%) varied by clinic, being lowest at Clinics C and D (6% and 5%, respectively) and highest at A and B (22% and 28%, respectively). Client populations at the four sites differed significantly across most various sociodemographic and health-related characteristics (p<0.05). Notably, the largest group of clients were in their 30s (37%); the great majority were on ARVs (82%); and 21% had strong concerns about confidentiality (“bothered if others in the waiting room know my status”).
ART, antiretroviral therapy; PMTCT, prevention of mother-to-child transmission.
Preferences for integrated care
When asked to cite reasons for clinic choice, factors related to integration, i.e., availability of specialist services or multiple services, were selected in less than 10% of responses overall. However, specialist services were mentioned more frequently than integrated services (7% versus 4%), even by clients at integrated sites (7% and 3% at Clinics A and B, respectively). The proportion citing specialist services as a reason for clinic selection was highest at the fully stand-alone site Clinic D (14%) but was not mentioned at all at the partially stand-alone hospital clinic (Clinic C), where instead the availability of multiple services was cited in 8% of responses.
Clients at Clinics C and D also scored higher than those at integrated sites when rating agreement on a scale for preferences for separated HIV services (“HIV services should be separated from other health services”), with mean score of 4.43 and 4.09 at Clinics C and D vs. 2.07 and 2.84 at A and B. While there was no statistical difference between clinics C and D (p>0.05), all other pair-wise comparisons were significantly different to each other (p<0.001).
Measures of satisfaction
Figure 1 displays mean scores across nine dimensions of client satisfaction and mean aggregate scores. While high rankings were given to most indices across all sites, there were significant variations across clinics (p<0.05). Waiting time ranked lowest overall, rating worst at the partially integrated site, Clinic B (2.99/5.00, standard deviation [SD] 1.44). Aggregate scores also varied markedly across site (F=23.31, p<0.001), with the highest score found at stand-alone Clinic D (4.47/5.00, SD 0.47), and lowest at partially integrated Clinic B (4.04/5.00, SD 0.47). In pairwise comparisons, all clinics differed from each other statistically except Clinics B from C, and Clinics A from D (p>0.05).
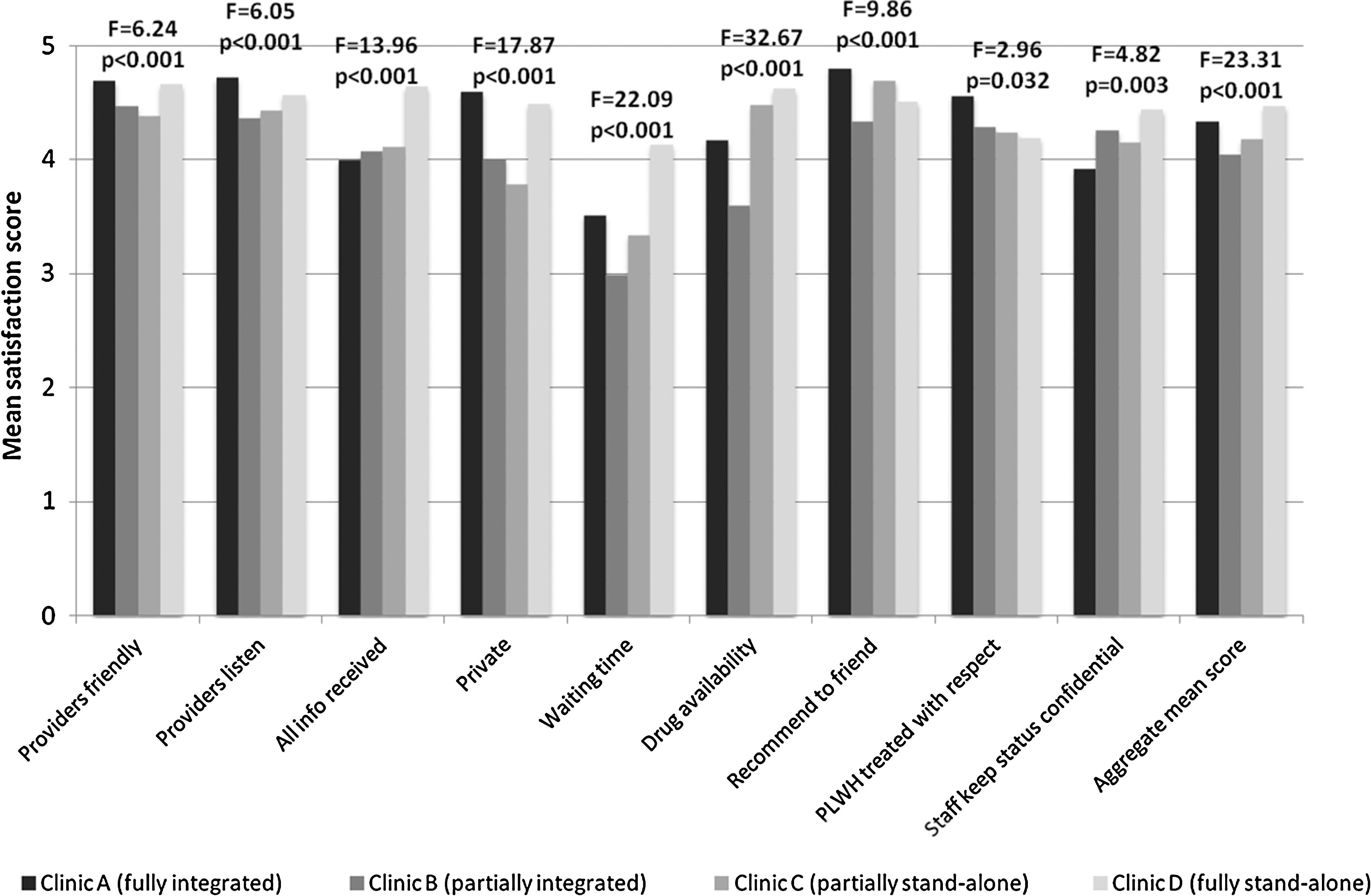
Satisfaction scores by clinic model (n=602).
When categorized as a binary measure, the proportion of clients at each clinic with an aggregate satisfaction score of 4.00 or more (out of 5.00) was highest at Clinic D (84%) and lowest at Clinic B (64%). Table 4 shows both the crude and adjusted odds of aggregate client satisfaction, across various sociodemographic and health factors. After controlling for all other variables in the table, there remained a strong association between clinic model and client satisfaction; clients at the partially integrated/stand-alone models, Clinics B and C, had significantly reduced odds of satisfaction compared with those at Clinic D (adjusted odds ratio [aOR] 0.45, 95% confidence interval [CI] 0.25–0.81, and aOR 0.53, 95% CI 0.31–0.90, respectively), but there was no statistically significant difference between Clinics A and D.
Adjusted for all other variables in table.
aOR, adjusted odds ratio; CI, confidence interval; ART, antiretroviral therapy; PMTCT, prevention of mother-to-child transmission.
Other factors significantly associated with satisfaction were age (although no trend across all age groups), living further from the clinic (with weak evidence); being on ARVs; and having fewer concerns about confidentiality in the waiting room.
Exploring satisfaction with HIV care: does service integration play a role?
While these quantitative data demonstrate satisfaction differences across clinic, other aspects of care also necessarily vary by clinic. Qualitative data help to elucidate which dimensions of care were either satisfying or dissatisfying to clients, and how these related (or not) to integration. Table 5 summarizes the key background characteristics of the qualitative sample. In total, 15 women and 7 men were interviewed at least once. Six clients were lost to follow-up (at 2 and 6 months post-ART initiation). The mean age was 31 (range, 22–45 years).
The data suggest that HIV client satisfaction in Swaziland was constituted by the following 11 dimensions of care, some of which related to integration or specialization, and some of which did not.
Access to medical care
The ability to access life-saving medical care was highly satisfying to clients interviewed, and they particularly valued access to doctor-led medical care, a benefit available across all models, since previously most had only experienced nurse-led care. This appreciation was also a consequence of ongoing health concerns common in HIV clients. Dissatisfaction was therefore expressed when clients felt providers were not adequately monitoring symptoms or addressing health problems. The model of care within which the treatment was delivered (integrated versus stand-alone site) did not influence their satisfaction with the access to ART drugs.
Costs
While all clients were theoretically accessing free ART, out-of-pocket costs could still be incurred and were dissatisfying to clients; including registration fees, or expenses for drugs or additional treatments beyond basic medications. While the need to pay fees was not a predominant thread in the data, integration could have a negative influence. At Clinic A, dissatisfaction was discernible when having to pay relatively high fees for additional SRH services: I:…how do you feel about the amount you pay? R:…I wouldn't say it's a lot…but I just don't like that fact that it's separated into bits […] you go for this, you have to pay, you go for that, you have to pay…[Female, Clinic A]
Perceptions of potential increased fees were also a reason why many clients at the hospital, Clinic C, felt strongly that HIV services should not be integrated with other health services. On the other hand, though, it was recognized that getting everything at once could also save money due to the reduced transport costs associated with multiple visits.
Access to multiple services
The co-location of different services within more integrated models of care formed an important dimension of satisfaction, with the potential to have complex health needs met on one site: when you have a problem with your eyes they also have a doctor for that, and when you have diabetes they check that here […] it's very important that it is all in one place rather than moving from one place to the next [Male, Clinic C]
Integration was also reported to have facilitated uptake of ART services in instances where other problems triggered an HIV test and diagnosis. Difficulties in accessing services when not colocated were also reported, underlining the important role that integration could play to help improve access to care.
But not all clients were able to reap the benefits of colocation, which was also influenced by the size of facility. The relatively small size of Clinics A, B, and D was contrasted positively with the larger hospital site, where problems attending referral services were highlighted: I don't want to go to a big hospital, like [Clinic C] which has so many departments, I prefer small clinics where it's better because you can walk around without getting tired, and most of the rooms are close to one another. At [Clinic C], they would tell you to go to Room 25, and sometimes you don't even know where it is and what to do when you get there [Female, Clinic B]
The relative proximity of the referral service was therefore important, and being sent further afield seemed to lead to diminishing returns of potential service uptake and decreased satisfaction. Referral down the corridor was even considered problematic for some.
Continuity of care
Internal or external referral to other providers also implied a diminished continuity of care. Many clients disliked repeating their ‘story’: I want to use family planning but it's not ok that I have to go […] to the other side [of the building] because […] you might find nurses who aren't like the ones we have this side, and also you have to explain to them and you might find someone who's not easy to talk to, and that's a problem [Female, Clinic B]
Seeing different providers was also seen to waste clients' time, and could even impinge on the quality of their medical care, since they “all treat you in different ways and give you different sets of medication.” Integrated care was therefore particularly important for those with diverse medical problems. Those attending stand-alone models also appreciated seeing fewer providers for different aspects of HIV care, implying that service fragmentation within HIV services may also be dissatisfying, irrespective of integration with other health services.
Technical competence
Provider expertise in HIV was appreciated by clients, and this was associated with HIV-only models. As one client at Clinic C put it, “they know about HIV” at the HIV clinic, unlike providers in other parts of the hospital. Having to see different ‘specialists' for different problems was thus seen to have its advantages, despite the inconveniences incurred: how can you be annoyed when you see several nurses ‘cause you find that this nurse specializes in this and the one specializes in something else […]? That would mean you don't really care about your health [Male, Clinic D]
Assessments of care were not, however, always based on technical criteria. Several statements alluded to poor technical competence, but these were not necessarily reported negatively by clients, who would often interpret them as good advice (for example, being told to avoid fizzy drinks). This highlights the clear difference between measures of technical competence, and measures of satisfaction.
Interpersonal care
The theme of providers' interpersonal skills recurred frequently in the data, suggesting this dimension of care was of critical importance to clients. High standards were reported across all sites, with providers often reported as kind, approachable, patient, remembering clients by name, giving good counseling, and allowing clients to ask questions. Conversely, areas of dissatisfaction were perceived violations of these behaviors, including lack of counseling, being rude, or ordering clients around. Clients were also appreciative if they felt providers were working hard for them, for example working through their lunch breaks; and particularly dissatisfied if they felt providers were being lazy, taking long breaks, or leaving early. While ratings of interpersonal care were generally unrelated to how integrated the clinic was (with the most effusive commentaries at the two NGO-run sites Clinics A and D), it was enhanced through better continuity of care and seeing fewer providers, as mentioned earlier.
Efficiency and coordination
Almost all clients appreciated fast, efficient service delivery, and this was particularly highlighted at stand-alone Clinic D, where the ART focus was seen as advantageous: I think it's better to be in a place that deals with just HIV. The waiting time is actually very short here…but if you are in a hospital or clinic that has many services available, with the little staff they have, you end up waiting longer. [Female, Clinic D]
However, while some considered the delivery of multiple services in one room a risk to efficiency, for others it could lead to time-saving, especially those with diverse needs (such as pregnant clients and those with TB). The hospital model was particularly beneficial for this client: It works for me, this setup here at [Clinic C]. The fact that I can get everything here, for my pregnancy needs and also the HIV treatment. […] Say for example, I have the same appointment for a [pregnancy] scan and checkup and also for [HIV] treatment at the other side…which is also the same as my appointment date at the TB centre [Female, Clinic C]
Achievement of this benefit, however, was also dependent on the effective coordination of care. Other clients reported having to return on multiple occasions for different services, wait for long periods in-between receiving different services, or being sent home without seeing anybody. This was particularly vexing when costs were implicated: Another thing that they do bad […], when you have come to take your ARVs, they say if you don't come on the right date they tell you to go back. […] They don't think money is involved when you have to come here. [Male, Clinic C]
As these quotes demonstrate, different clients reported differing experiences even within one site. Conversely, there was an appreciation for fixed appointment systems (in operation at Clinic D, and less effectively at Clinic A), seen to promote more ordered access to care.
Physical environment
Physical aspects of clinics were mentioned, although rarely. Overcrowding was mentioned by several clients, and this was intertwined with concerns about cleanliness, seating availability in waiting rooms, and waiting times. While such complaints were generally unrelated to integration, one client at Clinic C feared integration with the hospital outpatient unit due to increased client load, and one client at Clinic D feared an influx of pregnant women if SRH were to be integrated into the clinic.
Equity
Equity in access to care was important; clients were often aware of service entitlements at other facilities, and one particular “sore point” was the delivery of food parcels to those on ART at some sites and not others. However, this sense of injustice was unrelated to integration.
Confidentiality
Service integration played a role in the protection of client confidentiality. For some, attending an integrated clinic implied that HIV status remained protected. Many clients at Clinic A reported selecting the clinic for this reason (also demonstrated in quantitative data on reason for clinic choice). Nevertheless, there were still concerns at both integrated sites that HIV status could be revealed, for example if ART patients were to use the same room each time: Last year we were using the same room and even this year and people will start noticing that if you go into that room then it means you've come for this particular service [Female, Clinic A].
Provider actions or behavior were reported to exacerbate this problem, for example by calling out the ART clients to attend a particular room, or by handing out food parcels to those on ART.
Conversely, while some at stand-alone sites felt self-conscious about attending an “HIV clinic,” others felt that their status was actually more protected since every other client was HIV positive. Being able to be open about their status and talk to others living with HIV was satisfying for many of these clients: I: Since [this] is a clinic only dealing with HIV positive people, does that bother you? R: I actually thought about that when I first started here, but seeing people who're in the same situation as me encouraged me. So I don't feel like an outcast anymore. [Male, Clinic D]
Certain actions taken by clinics to increase confidentiality were also pleasing to clients, including separating out VCT and ART waiting areas at stand-alone Clinic D; and ensuring drugs could be collected inside the dispensary at integrated site Clinic A.
Respect for PLWH
Lastly, being respected as a PLWH was important for many and, encouragingly, all clients across all models reported positive provider attitudes towards them. In fact, some felt they were better treated now that they were positive: [the service is] even better when you've tested and you know your status (Laughing). I was talking to someone […and] she said when she went to her clinic, they treated the people who had tested better than the rest [Female, Clinic A]
Respect for their HIV status also encompassed positive provider attitudes towards clients' reproductive intentions, which again were reported across all models of care.
Discussion
This study has demonstrated that relationship between integrated care and client satisfaction is complex and multifaceted. While the quantitative survey demonstrated a significant association between clinic model and satisfaction score, the effect was not as anticipated since there was no difference in satisfaction between those in the most stand-alone clinic and the most integrated clinic. Furthermore, the qualitative analysis has demonstrated that satisfaction with these “models” is constituted by various dimensions of health care, some of which are attributable to service integration, and some of which are not (see center column in Fig. 2). Satisfaction dimensions identified here correlate closely with qualitative explorations of satisfaction with healthcare in general, 19 and specifically among PLWH. 25,28,31,33
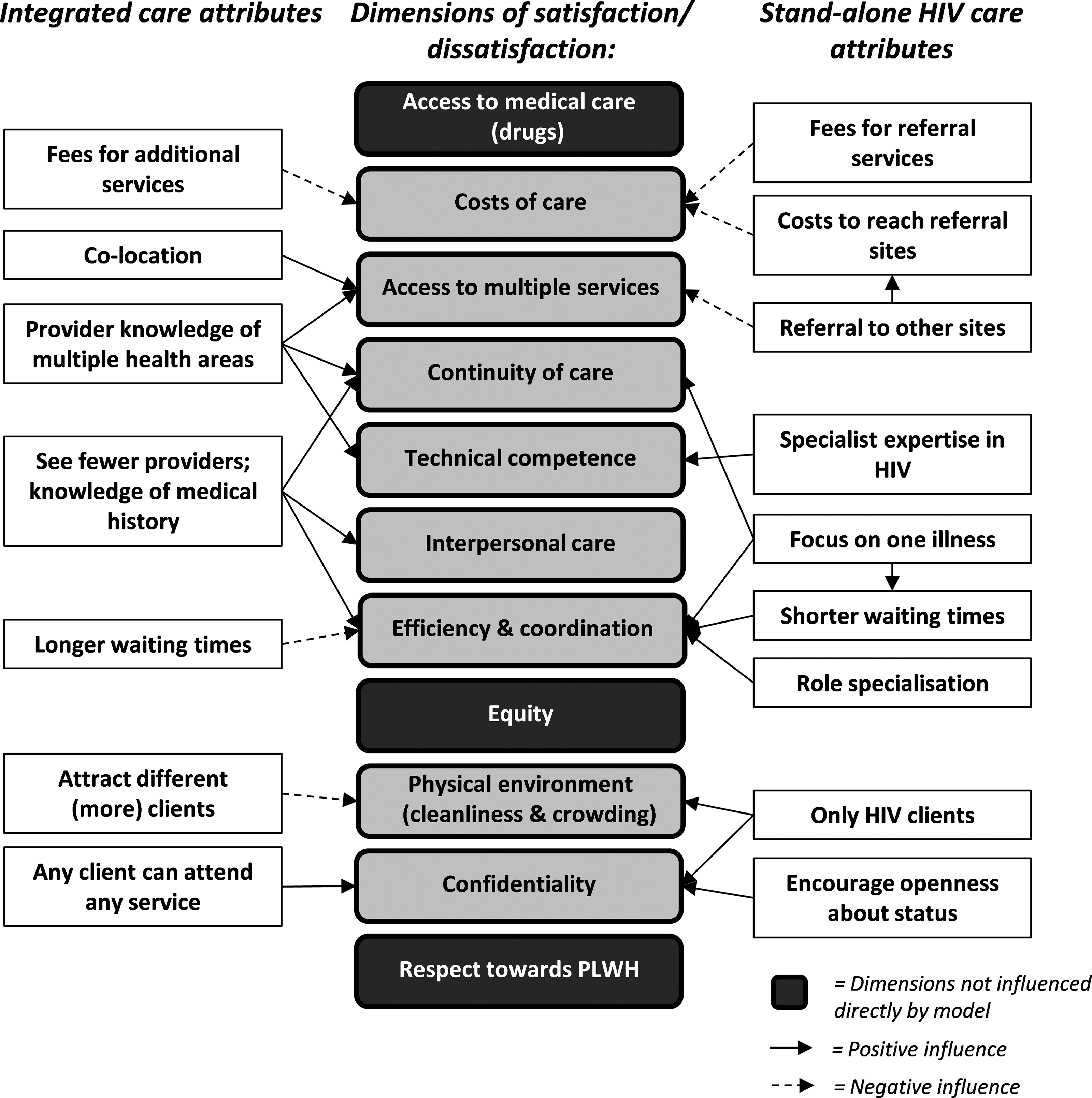
Relationship between model of care and client satisfaction.
As the figure shows, while certain dimensions of satisfaction were not specifically influenced by integration (black boxes), certain aspects of integrated care increased satisfaction, for example providing access to multiple services, or increasing continuity of care as clients had to “tell their story” less often. However, some aspects had the potential to decrease it (see dashed arrows), such as longer consultations resulting in longer queues, or higher fees for additional services. Attributes of stand-alone models (on right of the figure) were also differentiated in their impact; appreciation of specialist knowledge about HIV, for example, contrasted with dissatisfaction with referrals. And some dimensions could be impacted positively by both integrated and stand-alone models; for example, while efficiency was associated with HIV-only clinics, integrated care could also deliver this benefit, in particular for those with multiple health needs who could then see fewer providers.
Any potential negative impact of integration on waiting times is concerning, given clients' requirement to return regularly for ART refills and other visits. The fact that this dimension of care received relatively lower quantitative satisfaction scores across all sites indicates it is also an area of concern for clients. However, it is worth considering that such negative impacts of integration may be a price worth paying in order to more equitably distribute resources from well-funded vertical HIV programs into underresourced primary care settings. Nonetheless, the cost-effectiveness of integrated care still remains unknown 45 ; further research will be undertaken through the Intgra Initiative to evaluate the costs and cost-effectiveness of these different models of HIV care.
Furthermore, the achievement of some of the potential benefits of integrated care will necessarily be mediated by other external factors. For example, client load or clinic management capacity will influence waiting times and efficiency. However, as Table 1 shows, stand-alone Clinic D had a higher than average client load, suggesting that its potential negative impact was mitigated by other factors, such as clinic management or fixed appointments. Other resource inputs may also play an equal if not more important role in determining interpersonal care quality, an important dimension of satisfaction for clients. While integration may reduce the number of providers seen, thus enhancing trust and satisfaction, several aspects of interpersonal care also ranked highly at the most stand-alone site. This could be attributable to seeing fewer providers only for HIV, or instead factors like provider training. The fact that the two predominantly NGO-run clinics (A and D) achieved highest satisfaction scores may well reflect stronger management principals, provider training and greater resource inputs.
Overall, the high scores and positive reports achieved across all sites were encouraging. To some extent this may reflect reporting bias inherent in satisfaction surveys: the relative dependency of clients on the health system, the need to maintain constructive relationships with those providing care, and the general preference for holding a positive outlook all contribute to a series of psycho-social pressures that mitigate criticisms of health care received. 27,28,46,47 However, the positive responses recorded through in-depth probing in repeated qualitative interviews, as well as reports of superior care in HIV services compared to other health services, suggests that the HIV program is achieving satisfaction benefits across various dimensions of care. The extent to which this reflects satisfaction with treatment in general, rather than satisfaction with a clinic, is more ambiguous however. The fact that many of those at stand-alone models wanted to keep HIV services separate from other generalist health services is indicative of this. The quantitative analysis also demonstrated that those on ARVs had higher odds of satisfaction than those not yet on ARVs. While not specifically addressed in this paper, the broader study found that conceptualizations of satisfaction were relative (dependent on the user's own personal situation and background), changeable over time, and also dependent on the actions of individual providers, making clinic-wide assessments challenging. 40 A priori expectations derived from previous health care experiences were also important in determining satisfaction, a common occurrence in satisfaction studies. 18 The relativity of the construct therefore underlines the importance of using qualitative data to explore the potential mechanisms through which structural aspects of care can impact on satisfaction.
Aside from challenges in measuring satisfaction, the study also had other limitations. The differential survey refusal rates indicate selection bias and refusers may have had different levels of satisfaction to participants; but the direction of this bias remains unknown. The relatively low Chronbach α (0.68) on the aggregate satisfaction score also falls short of the recommended level for scale reliability (0.7), and further work is recommended to develop a measure of satisfaction with greater internal consistency in this context. The observational study design is also problematic: clients self-selected their facility, and while the multivariable modeling attempted to control for differences in client profiles between sites, it is unlikely to have eliminated selection bias. Given that client expectations are deterministic in satisfaction 18,19 and are likely to vary by sociodemographic and cultural determinants, there is potentially unmeasured confounding in the adjusted effect estimates. The cross-sectional design also precludes determination of causality between integration model and satisfaction. While the triangulation with qualitative data attempted to overcome this limitation, further longitudinal research would be helpful to investigate how satisfaction changes following service integration, including potential changes in the dimensions of satisfaction identified in this study, such as waiting times, costs, access to medication, and ratings of interpersonal care. The broader Integra Research Initiative (which this study forms a part of) will attempt to explore some of these questions through evaluative research in both Swaziland and Kenya. It is also important to note that satisfaction does not necessarily correlate with quality; a higher quality of care can raise expectations, which may then actually lead to lower levels of satisfaction. 48 Different levels of satisfaction may therefore simply measure different perspectives on health care, rather than different levels of satisfaction with the same experience. 18
These study results therefore add weight to a growing body of evidence indicating that HIV clients appreciate health services in different ways, depending on their needs and situation. Clients at a fully stand-alone HIV clinic were most satisfied in this study, even after controlling for differences between clinic populations. Generalizations about the inherent value of integrated care models must therefore be avoided; programmers need to recognize the potential for stand-alone HIV services to fill an important gap in service coverage in high HIV prevalence contexts. Integrated and stand-alone models had different benefits for different clients. Further ongoing research on the efficiency and cost-effectiveness of different models of care conducted through the Integra Initiative will contribute to these debates, and help to confirm whether stand-alone services do indeed have an important role to play in high HIV prevalence contexts, in particular in settings where demand for HIV services may overwhelm existing primary care services. Overall, however, the high satisfaction scores recorded, in particular the widespread respect towards PLWH, were encouraging, and suggest different models work for different types of clients. However, since this research was not longitudinal, and most clients had not experienced care in other settings, the positive reports also likely reflect the fact that, ultimately, people like what they know.
Footnotes
Acknowledgments
We would like to thank the fieldwork teams for their hard work, and the research participants who gave their time to be interviewed. We also would like to thank the managers of the four clinics who facilitated data collection, as well as the Ministry of Health in Swaziland who supported the research and is a key partner in the Integra Initiative. We finally would like to thank colleagues who advised on aspects of research design and/or analysis including: John Cleland, Ian Askew, Charlotte Warren, Natalie Friend du-Preez, Manuela Colombini, Andy Guise, Judy Green, and Andy Sloggett.
The study was partly funded by an Inter-Disciplinary PhD studentship to KC from the Medical Research Council and Economics & Social Research Council; and by the Bill and Melinda Gates Foundation through the Integra Initiative. The funders played no role in study design, data collection, analysis, and interpretation. The Integra Initiative is a research collaboration between the International Planned Parenthood Federation, the London School of Hygiene & Tropical Medicine, and the Population Council, investigating the benefits and costs of integrated SRH and HIV services. Research was conducted in Swaziland, Kenya and Malawi. Research team: Timothy Abuya, Ian Askew, Isolde Birdthistle, Kathryn Church, Manuela Colombini, Natalie Friend du-Preez, Joshua Kikuvi, James Kimani, Jackline Kivunaga, Joelle Mak, Susannah Mayhew (PI), Christine Michaels, Richard Mutemwa, Charity Ndigwa, Carol Dayo Obure, Sedona Sweeney, Anna Vassall, Charlotte Warren (PI), Charlotte Watts (PI), Weiwei Zhou.
Author Disclosure Statement
No competing financial interests exist.