
Abstract
This study examined the feasibility, acceptability, and outcomes of a culturally tailored smoking cessation intervention for HIV-positive African American male smokers. Eligible smokers were enrolled in a seven-session group-based treatment combined with nicotine patch. The mean age of participants was M=46 years. The majority were daily smokers (71%), smoked a mentholated brand (80%), and averaged 8.6 (standard deviation [SD]=8.1) cigarettes per day. Baseline nicotine dependency scores (M=5.8) indicated a moderate to high degree of physical dependence. Of the 31 participants enrolled, the majority completed treatment (≥3 sessions; 68%), 1-month follow-up (74%), and 3-month follow-up (87%) interviews. Program acceptability scores were strong. However, adherence to the patch was low, with 39% reporting daily patch use. The majority of participants (80%, n=24) made a quit attempt. Furthermore, over the course of the intervention, smoking urge, cigarettes smoked, nicotine dependence, withdrawal symptoms, and depression scores all significantly decreased. Follow-up quit rates at 1 and 3 months ranged from 6% to 24%, with treatment completers having better outcomes. This first of its kind intervention for HIV-positive African American male smokers was feasible, acceptable, and showed benefit for reducing smoking behaviors and depression scores. Smoking cessation outcomes were on par with other similar programs. A larger trial is needed to address limitations and to confirm benefits.
Introduction
Tobacco use and HIV infection
The prevalence of tobacco use among HIV-positive men is notably higher than for men in the general population (i.e., 40–70% versus 20%, respectively). 9 –11 Contrary to the presumed increase in motivation to quit smoking after diagnosis of a serious illness, 12 data suggest that without intervention, more than 80% of HIV-positive smokers continue smoking. 10 Despite these alarming statistics, HIV-positive smokers have historically not been targeted for intervention due to poor disease prognosis, the absence of culturally appropriate treatments, and the absence of smoking cessation as part of HIV clinical care models. 13 However, with new antiretroviral regimens, HIV-positive individuals are living longer and are more susceptible to the negative consequences of smoking. 14 For example, among HIV-positive smokers, tobacco use is associated with increased incidence of opportunistic infections, cardiovascular and lung disease, cancers associated with human papilloma virus (HPV), and increased overall mortality. 10,15 –19 The reasons for the excess risk for diseases such as lung cancer are thought to be primarily attributable to the high rates of smoking, rather than the direct influences of HIV-linked immune suppression. 10 The clinical and public health significance of reducing smoking among HIV-positive smokers is further underscored when one considers that smoking is known to be associated with higher viral loads and lower CD4+ cell counts. 20,21 Finally, nicotine dependence has emerged as a significant and independent barrier to adherence to antiretroviral therapy in HIV-positive smokers. 22
Smoking cessation interventions for HIV-positive smokers
Many HIV-positive smokers are interested in quitting smoking. 9 However, to date, there is a limited research on the effectiveness of smoking cessation interventions involving HIV-positive smokers. The majority of available research is based on results of small pilot tests (n=4) of clinic based interventions. 23 –26 For example, Cummins et al. 23 examined the impact of a combined counseling, written educational materials, and 8 weeks of nicotine replacement therapy (NRT) on smoking cessation outcomes. More than half of participants (59%, n=16/27) completed treatment and 22% achieved biochemically confirmed quit rates at 5-month follow-up. The results of three larger randomized clinical trials were mixed. Lloyd-Richardson and colleagues 27 reported on quit rates following a five-session motivational enhancement intervention trial with NRT (n=232) compared to two-session brief counseling plus NRT (n=212). Abstinence rates at 2-, 4-, and 6-month follow-up were 12%, 9%, and 9%, respectively, and did not differ between treatment groups. In addition, Vidrine and colleagues 28 reported on abstinence rates following an eight-session telephone counseling intervention (n=236) versus usual care (physician advice, written materials, and NRT; n=238). At 3 months, participants in the telephone counseling intervention were 4.3 times more likely to be quit compared to the usual care group. Another recent study compared a tailored group-based intervention, Positively Smoke Free, plus NRT compared to standard of care (n=145). Smokers in the Positively Smoke Free condition had nearly double the quit rates of control participants (19.2% versus 9.7%). 29 While results of these trials are promising, some limitations were noted with samples restricted to non-drug users, smoking status not confirmed by biochemical verification, and active treatments not targeted to racial minority or MSM issues. Furthermore, representation of African Americans was limited in the majority of available studies. Given the detrimental impact of smoking on HIV infected persons, innovative and systematic research is needed to increase access to effective treatments for those most vulnerable to adverse HIV-related health outcomes. 30
Specific aims
The Tobacco Use and Dependence Clinical Practice Guidelines 31 has called for research to determine the effectiveness of standard and culturally-tailored smoking cessation interventions for at risk populations. Our group 32,33 has examined a culturally tailored treatment in African American smokers and the results suggest that culturally targeted smoking cessation interventions may improve program completion and end of treatment quit rates. However, the sample was largely female, and interventions developed for general African American smokers may not address the unique psychosocial, behavioral, and medical issues facing African American MSM who are also HIV positive. 6,34 To address this gap in the literature, the primary aim of this project was to conduct a pilot study to determine the feasibility, acceptability, and adherence to a new culturally tailored group intervention for HIV-positive African American MSM smokers. Secondary aims were to identify the impact of the intervention on changes in psychosocial variables (i.e., depression), smoking-related outcomes (e.g., smoking urges, withdrawal symptoms), and smoking behavior (reduction in number of cigarettes smoked and quit rates).
Methods
Figure 1 shows a CONSORT diagram of the flow of participants through the study. Participants were recruited from February to July 2011 by referrals from medical providers, posted flyers, venue recruiting, and from a volunteer database. Interested individuals were screened for eligibility via phone interview. Study inclusion criteria were: (1) male gender, (2) age between 21 and 65, (3) self-identification as African American, (4) self-reported seropositive HIV status, (5) attraction to men or both men and women, (6) current regular smoking (i.e., more than 100 cigarettes lifetime and at a frequency of 3 or more days per week in the last year), and (7) interest in quitting smoking (i.e., a score of at least 5 on a 0 [no interest] to 10 [high interest] scale of interest in smoking cessation). A total of 44 individuals contacted study personnel regarding participation in the study. The majority of callers (93%, n=41/44) met eligibility criteria and was invited to participate in a 60-minute study orientation session. Seventy-six percent of those meeting eligibility attended the orientation session (n=31/41) to obtain additional information about study procedures, provide informed consent, and complete baseline assessment measures. The time from the initial telephone screening and attendance at the orientation session ranged from one to five weeks for most participants with the average length of time being about three weeks. Of those who attended the orientation session, 81% (25/31) attended Session 1. The study protocol was approved by the institutional review boards of the University of Illinois at Chicago, the University of Chicago, and the Howard Brown Health Center (HBHC).

Flow of participants through recruitment, intervention, and follow-up.
Procedures
The project was conducted in the research department of HBHC, a community-based health center serving primarily lesbian, gay, bisexual, and transgender (LGBT) patients. The staff was experienced in recruitment, consent procedures, interview methods, and data collection with high-risk, multiethnic, and HIV-positive sexual minority men. Treatment included six 90-min, semi-structured, group-based counseling sessions. A total of five intervention groups (n=31 participants) were conducted each averaging about six members. Participants who missed either the first or second session (sessions prior to quit day) received a make-up session prior to the next scheduled session. Each week, subjects completed questionnaires and a brief interview with a research assistant, provided an expired air carbon monoxide (CO) sample (Smokerlyzer®, Bedfont, Medford, NJ), and starting at Session 3, received a weekly supply of nicotine patches. These pregroup procedures took approximately 30 min to complete and were followed by a treatment session. The quit date was targeted for the third week (Session 3) of the intervention. Follow-up assessments were conducted at 1 and 3 months postquit date. Participants were compensated $15.00 for the completion of the baseline assessments, $5.00 per session to cover transportation costs, and $20 and $25 for 1- and 3-month follow-up assessments, respectively.
Nicotine replacement therapy
As recommended by the Treatment Practice Guidelines, 31 the benefit of nicotine replacement was explained to participants during orientation and transdermal nicotine patches (Nicoderm CQ © , GlaxoSmithKline, Clifton, NJ) were provided to all participants as appropriate (n=3 participants were not appropriate for patch use due to low smoking levels). Patch use was advised to start on the quit date and samples were provided for the next 4 weeks. After that juncture, participants could purchase them on their own if interested. The study nurse determined whether NRT was counter-indicated for any participants, provided information about correct usage, and monitored for side effects. Patch use was not a requirement for participation. Consistent with use guidelines (Nicoderm CQ), the initial starting dosage was based on the number of daily cigarettes reported by participants: those who smoked 10 or more cigarettes per day received 21 mg patch for 2 weeks, 14 mg patches for the next week, and 7 mg patches for the final week. Those who smoked less than 10 cigarettes per day used a 14 mg patch for 2 weeks before transitioning to a 7 mg patch for 2 weeks. The rationale for providing patch samples for 4 weeks rather than longer intervals suggested by manufacturers was that adverse effects could not be monitored regularly after end of the treatment and quit rates with 4 weeks of patch use has been shown to produce good quit rates at end-of-treatment at 4 weeks in general adult smokers (44–57%) 35 and in African American smokers (34%). 33 This interval is also consistent with the median duration of typical over-the-counter patch use reported by most smokers. 36
Smoking cessation treatment
The pretreatment, orientation session was delivered by a licensed clinical psychologist (A.M.) with expertise in providing culturally competent counseling. The actual treatment sessions were delivered by a female clinician with extensive experience in conducting smoking cessation interventions with LGBT smokers. The intervention counselor was trained and supervised by A.M. The intervention was an adaptation of a standardized smoking cessation treatment developed by A.K. (Courage to Quit©).
33,37
Courage to Quit (CTQ) is a psychosocial treatment based on evidence-based interventions and includes cognitive-behavioral, motivational, and 12-step addiction techniques (
Project Exhale, the culturally adapted CTQ program included the same techniques in the standard CTQ program but with additional content addressing issues relevant to smokers who are African American, MSM, and HIV positive. The modifications were developed by systematic and formative research methods 38 including focus group feedback, expert review, and learner verification trials. These procedures helped to tailor the curriculum (for details, see Matthews et al., unpublished data). Cultural adaptation was also based on strategies outlined in the literature. 32,39 The adapted curriculum also included: (1) culturally appropriate images; (2) general and unique triggers; (3) norm-shifting messages; (4) discussion of minority stress; (5) information about the higher rates of smoking among HIV positive individuals and the additional health risks associated with smoking when HIV positive, (6) information about tobacco industry targeting of the African American community; (7) culturally appropriate spirituality/motivational messages; (8) specific quotes from focus group participants to illustrate key issues; (9) use of cultural references to illustrate key concepts; and (10) the importance of NRT (Table 1). In general, the culturally tailored groups contained 1–2 additional or adapted modules per session and were 30 min longer than the typical CTQ sessions (90 min versus 60 min).
MSM, men who have sex with men; NRT, nicotine replacement therapy.
Assessments
Study measures were collected at baseline, weekly sessions, and at 1- and 3-month follow-up, as appropriate. Baseline measures included questions about participants' background, smoking behaviors, and psychosocial variables. Smoking-related measures included readiness to quit (Likert scale ranging from 0 to 10, with higher scores indicating more readiness to quit), the Fagerström Test for Nicotine Dependence (FTND), 40 the Brief Questionnaire of Smoking Urges (QSU-brief), 41 and the Minnesota Nicotine Withdrawal Scale (MNWS) 42 . Daily frequency and patch use was determined by self-report, as obtained via Time Line Follow-Back interview (TLFB). 43 Psychosocial variables measured included the Perceived Stress Scale (PSS) 44 and the Beck Depression Inventory (BDI). 45 Finally, potential problem drinking behavior was assessed via the Michigan Alcohol Screening Test (MAST). 46 Weekly and follow-up assessments included readiness to quit, smoking urges, withdrawal symptoms, and 7-day point prevalence quit rates. Quit status was biochemically verified via expired CO breath reading such that, if CO was higher than 8 ppm, the participant was conservatively classified as a current smoker.
Program feasibility was determined by treatment completion rates (the mean number of sessions attended and the percentage of participants completing at least half of weekly sessions) and 1- and 3-month follow-up retention rates. Program acceptability was measured at the end of treatment (1-month follow-up visit) and included ratings of treatment satisfaction, usefulness of the treatment manual, and whether the program was targeted to their needs (scale 1–10, with higher scores meaning more satisfaction). Treatment elements were evaluated using a 5-point scale (1–5, with higher scores meaning more satisfaction): weekly CO tests, identifying smoking triggers, methods of handling triggers, stress management, cognitive techniques, self-monitoring (“wrap sheets”), and addressing weight and health concerns. 33 Participants also rated their satisfaction with their smoking cessation counselor using a 5-point Likert scale on the following: competency, communication skills, and overall satisfaction.
Data analysis
Given the pilot nature of this acceptability/feasibility trial, the study was not specifically designed to determine the efficacy of this program, but rather establish if the intervention was acceptable and feasible and to examine possible effects on smoking outcomes. Therefore, we were most interested in participant attendance and retention, patch adherence, and biochemically-verified 7-day point prevalence smoking quit rates. With regard to analysis, we first described the sample on demographic and background characteristics, smoking behavior, psychosocial health, and substance use. Then, we summarized participants' attendance as well as their evaluation of therapists and the overall program. Finally, we summarized the smoking and psychosocial outcome variables of interest at 1- and 3-month follow-up and compared them to baseline values via paired t tests.
Results
Participant characteristics
Participant baseline characteristics are described in Tables 2 and 3. The average age of participants was M=46 years. The majority were daily smokers (71%), smoked a mentholated brand (80%), and averaged 8.6 (standard deviation [SD]=8.1) cigarettes per day. Baseline FTND nicotine dependency scores (M=5.8) and BQSU smoking urge scores (M=45.2) indicated a moderate to high degree of physical dependence. Recreational substance use was prevalent in many participants, including past year use of alcohol (80%), marijuana (45%), and cocaine (36%). With regard to alcohol use, 45% had a total score of three or above on the SMAST, indicating the possible presence of problem drinking behaviors. Furthermore, 9% of the sample reported clinically significant levels of depression, defined as a total score of 10 or above on the BDI.
Feasibility: treatment enrollment, adherence, and retention outcomes
As stated earlier, the majority (76%; n=31/41) of eligible study candidates enrolled in the study, completing both the orientation session and at least one of the six intervention sessions (see Fig. 1 for enrollment and retention details). As the study progressed, attendance decreased steadily (Table 4). Participants did attend an average of 4.0 (SD=2.3) sessions, however, with 68% completing at least half of the intervention sessions (i.e., ≥3 sessions). Despite good session attendance, NRT use was low with 68% (n=21/31) of participants initiating any nicotine patch use (i.e., reported using at least one patch). Those reporting any NRT initiation averaged use on 11.0 (SD=10.4) of a possible 28 patch days (39% adherence to daily use). Finally, retention of study participants for follow-up was high: 74% (n=23/31) completed the 1-month interview and 87% (n=27/31) the 3-month interview.
Total n=31.
Acceptability: program and therapist evaluations
Program acceptability scores (0–10 scale) at end of treatment (1-month) were high including: satisfaction with treatment (M=9.6), perceived usefulness of the program (M=9.0), readability of the treatment manual (M=9.5), and whether the program was targeted to their needs (M=9.3). Participant ratings of the perceived helpfulness of various treatment components were also positive. The opportunity for group interaction, weekly measuring of carbon monoxide, strategies for identifying and managing smoking triggers, didactic information about the cycle of addiction and relapse, cognitive strategies for managing negative mood states, and strategies for managing weight gain were all highly rated (mean scores 4.0–4.7 on a 5-point scale). Therapists ratings in terms of comfort level, competency, and helpfulness were also high (all means=4.7 on a 5-point scale).
Treatment outcomes: smoking and psychosocial variables
The means and standard deviations for smoking and psychosocial outcome measures are shown in Table 5. At 1-month follow-up, readiness to quit scores had improved from baseline (t(19)=−3.51, p<0.01). There were also significant reductions in FTND nicotine dependency scores (t(14)=3.70, p<0.01), BQSU smoking urge scores (t(20)=5.90, p<0.001), MNWS withdrawal symptoms (t(20)=2.73, p<0.05), numbers of cigarettes smoked per day (t(20)=3.45, p<0.01), and BDI depression scores (t(18)=3.11, p<0.01). At 3-month follow-up, BQSU smoking urge scores (t(19)=6.43, p<0.001), number of cigarettes smoked per day (t(15)=2.73, p<0.05), and depression scores (t(16)=2.10, p=0.05) remained reduced compared with baseline.
p≤0.01.
p≤0.001.
p<0.05.
Data are mean (SD). For both 1- and 3-month follow-up, values were compared to baseline.
Treatment outcomes: quit status and reduction in number of cigarettes smoked
As shown in Table 5, CO-verified quit rates in the intent-to-treat sample were 16% at 1 month and 6% at 3 months. Among participants completing three or more sessions, quit rates were somewhat higher (24% at 1 month and 10% at 3 months). Among those participants who did not completely quit smoking, significant reductions in smoking were observed, with fewer daily cigarettes at 1 (−6.6; t(20)=3.45, p<0.01) and 3 months (−5.2; t(15)=2.73, p<0.05), as compared with baseline. Among these reducers, CO readings confirmed that number of cigarettes smoked daily decreased from baseline to follow-up: the proportion of participants with readings of 21+ppm (indicating regular smoking) was significantly smaller at both 1- (12.9%) and 3-month follow-up (19.4%) than at baseline (35.5%; Fig. 2).
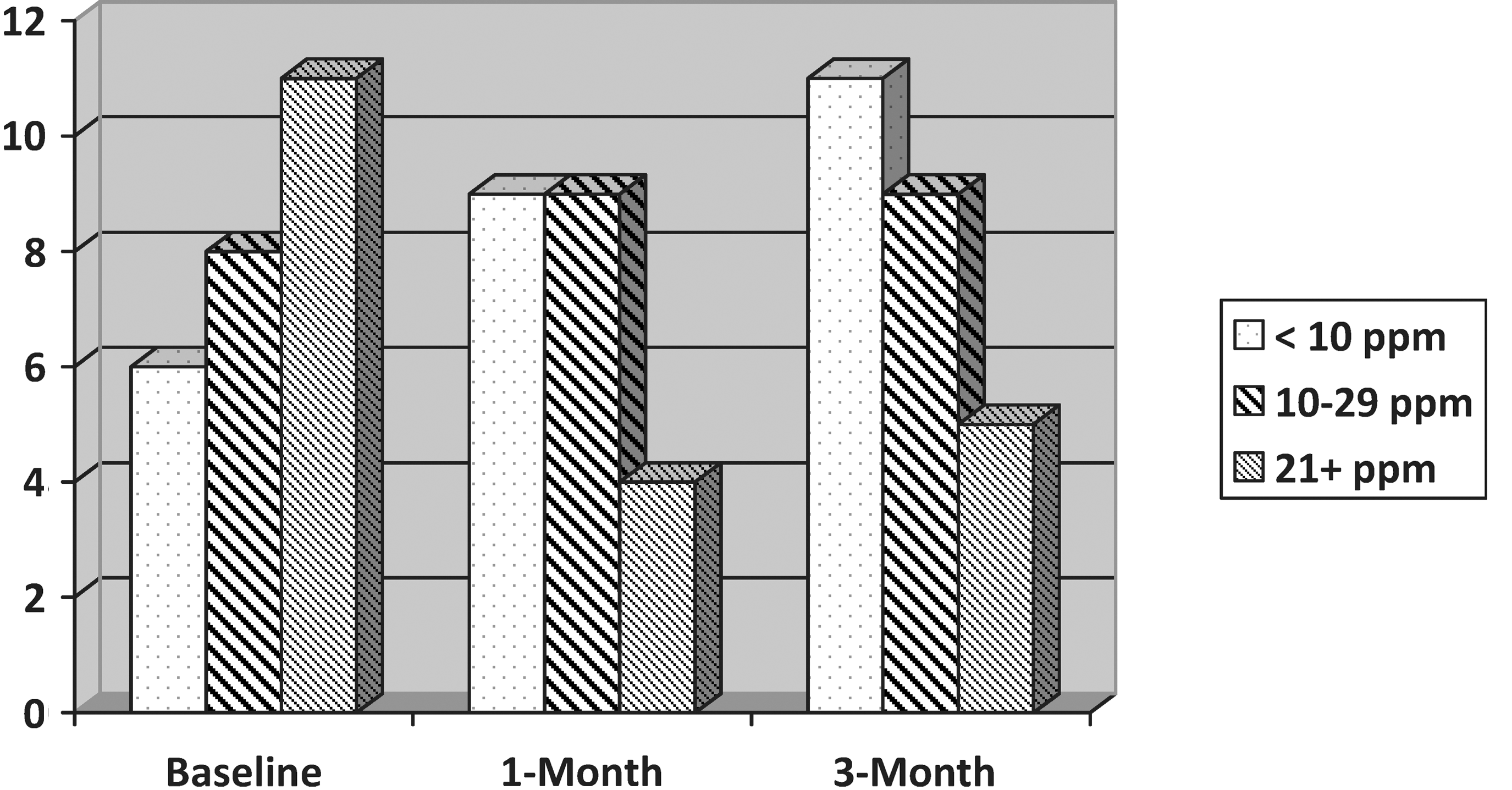
Carbon monoxide (CO) readings for intent-to-treat sample. Participants are categorized into groups based on CO readings, which are typical of nonsmokers or “chippers” (<10 ppm), light or occasional smokers (10–20 ppm), and regular smokers (>21 ppm) at baseline, 1, and 3 months. Frequencies reflect the number of participants who fell into each category at each time point.
Discussion
With the advent of antiretroviral medications, HIV treatment has shifted from primarily palliative care to a chronic disease model. 47 As with other chronic illness, smoking negatively impacts the disease trajectory of HIV-positive individuals. However, HIV-positive smokers experience unique barriers to cessation necessitating the need to adapt standard programs to their special circumstances. 5,6,48 To date, there is a paucity of research examining acceptability, feasibility and outcomes associated with tailored smoking cessation interventions among HIV-positive smokers and/or racial and ethnic groups within this population. To our knowledge, this study is the first to report on the development, implementation, and delivery of a novel group based intervention targeting the unique barriers and facilitators to smoking cessation among HIV-positive MSM African American smokers. Strengths of the study include systematic development and evaluation of a new treatment manual targeted to an underserved and medically compromised and minority subgroup, obtaining high study completion and retention rates, use of nicotine replacement therapy, and the biochemical verification of quit status. Despite the limitations of the study, results have implications for the delivery of culturally appropriate smoking cessation treatment to HIV-positive smokers and the reduction of smoking-related health disparities among MSM African Americans who are HIV-infected.
Examination of the acceptability and feasibility of the intervention was the main focus of the study. Conducted at a health care agency serving LGBT persons, overall level of satisfaction with the smoking cessation treatment and counseling services received was high. Further, acceptability ratings for the tailored materials were encouraging especially regarding the perceived usefulness and readability of the treatment manual and the relevance of the intervention to their smoking cessation needs. These findings are consistent with a recent study of African American smokers that suggested that culturally specific material were more effective at capturing attention, providing encouragement and gaining interest compared to standard materials. 49 These findings were also consistent with the stated preferences of HIV-positive MSM for a culturally adapted cessation program aimed specifically for MSM and for services provided by a LGBT health care provider. 50
As demonstrated in earlier studies, 23 we found high levels of interest among HIV-positive in receipt of smoking cessation treatment. The ratio of eligible to enrolled African American smokers in general smoking cessation clinical trials has been shown to be low compared to whites. 51 In this pilot study, 93% of interested callers were eligible for the study and of those eligible callers, 76% went on to enroll in the study. Treatment participation was also good with 76% of the sample receiving at least half of the intervention (≥3 of 6 treatment sessions). Retention of study participants was high given the presence of co-occurring alcohol and substance use behaviors, which is typically a strong predictor of poor intervention retention. 52 The overall attrition rate of less than 20% similar was similar to that of a telephone-based counseling intervention for HIV-positive smokers (19% at 3 months). 53
The psychosocial profile of the HIV-infected community, characterized by high rates of psychiatric comorbidity, drug and alcohol use, and low levels of social support, suggests that achieving high cessation rates will be a great challenge. 6 Overall quit rates were modest with the short-term quit rates at 16% for participants who attended at least one treatment session and 24% for treatment completers. Despite the modest outcomes, our rates in this challenging populations compares favorably with the results of the two most rigorously evaluated programs—an eight-session randomized telephone counseling intervention (37%) 53 and a four-session motivational enhancement intervention (12%). 27 However, by 3-month follow-up, quit rates for the enrolled sample were 6% and 10% for treatment completers. While both quit rates are comparable to the standard of care (approximately 7%) observed in general populations samples, additional research will be needed to improve upon these smoking cessation outcomes. HIV-positive smokers may benefit from more frequent contacts over extended periods of time to enhance long-term success rates. 54 For example, extending treatment following an intensive group based intervention by incorporating additional sessions via text messaging, telephone counseling, social media, or other online options may prove effective in improving outcomes, ongoing support, and relapse prevention in a less costly fashion. 14,55,56
More promising were the changes observed in other smoking and psychosocial variables. Statistically significant reductions from baseline to follow-up were achieved in levels of nicotine dependency, smoking urges, withdrawal symptoms and the number of cigarettes smoked daily. Although levels of depression were not clinically elevated in the majority of our participants, depression scores declined even further throughout the course of treatment and improvements were maintained at 3-month follow-up. Overall, the finding that patients adhered to the treatment at a high rate and improved in the outcomes of interest suggests that using a group-based and tailored intervention for smoking is feasible and acceptable to African American HIV-positive smokers.
Important lessons learned and implications for future research
Dissemination of “lessons learned” when working with underserved populations is critical to enhancement of research methods and the identification of future best practices. Several strategies shown to increase recruitment and retention of minority populations into smoking cessation research were used including using culturally relevant recruitment materials, hiring a recruitment specialist, and having a diverse team of research assistants. 57 In addition, word of mouth was very effective with this population of smokers. Research suggests that the social networks of African American MSM in urban settings are close knit. 58 As such, respondent-driven sampling (RDS) may also be an effective method for recruiting a larger and potentially more diverse sample of HIV-positive African American smokers into future studies.
The second lesson learned relates to eligibility requirements for smoking cessation interventions. Most trials enroll smokers who consume between 12–40 daily cigarettes. 31 This range has been used to minimize sample heterogeneity and ensure safety with nicotine replacement which was initiated at the highest dose (21 mg/day). However, the majority of African American smokers are light smokers (<10 cigarettes per day) who often present with similar or even greater nicotine dependence scores as more frequent smokers. 59 In addition to low numbers of cigarettes smoked, the vast majority of our HIV-positive participants would have been ineligible for standard smoking cessation interventions due to co-occurring substance and alcohol use. Comorbid conditions negatively impact smoking cessation outcomes. 52,60 However, the majority of HIV-positive smokers present with psychiatric and substance use comorbidities. 61 Future cessation programs will need to be adapted to address these co-morbidities 62 and determination of eligibility classifications for African American smokers in smoking research trials. 51
The majority of smokers in our study smoked a mentholated brand of tobacco. In some but not all studies, 63 –66 menthol cigarette use (versus nonmenthol) has been shown to be associated with lower likelihood of making or sustaining a quit attempt, and higher relapse rates. 67 –71 Among HIV-positive smokers, smoking menthol cigarettes is a significant predictor of elevated proinflammatory markers such as interleukin (IL)-6 levels 16 that have been linked to kidney 72 and cardiovascular diseases, 73 and increased risk of all causes of mortality. 74 –76 Smoking cessation interventions should be developed that specifically address the more difficult cessation trajectory of menthol smokers.
Overall, adherence to NRT was low among study participants. A number of barriers to the use of NRT have been identified among African American smokers including viewing NRT as a drug with potentially serious side effects, beliefs that the use of NRT will increase levels of nicotine dependence, lack of familiarity and dissatisfaction with the lack of control over the delivery of nicotine when using NRT. 77,78 In addition, HIV-positive smokers in our study reported additional barriers including “not wanting to take another medication” and fears that NRT would “interfere with HIV medications” (data not shown). The benefits of NRT were emphasized as part of our tailored curriculum; however, perhaps more focus on repeating this message and addressing medication concerns in this underserved group would increase adherence in future trials. Another approach may be to employ reminders of adherence via text message approaches which have been effective in other behavior change programs 79 and may be useful in reducing barriers to NRT adherence by providing daily reminders, tips for managing minor side-effects, and countering attitudinal barriers. Use of other pharmacotherapy approaches other than NRT should also be considered. A recent study reported on the safety, tolerability, and effectiveness of Varenicline in HIV-positive smokers. 80 Smoking cessation counseling and consistent follow-up by health care providers working with HIV-positive smokers has also been shown to be effective 81 and may serve to reduce barriers to adherence to NRT and other stop smoking medications.
Objective verification of smoking status is the gold standard in smoking cessation research. 54 In the present study there were large differences between self-reported and CO-verified quit rates. Research suggests that under-estimation of smoking prevalence rates based on self-reported measures has been shown to be minimal in U.S. samples (0.6%). 82 Demand characteristics of the data collection process may have been associated with the discrepancies between self and CO-verified smoking status. Additional potential factors may include the high percentage of marijuana smokers in the sample (45%), high percentage of participants that reported other tobacco use such as cigars (42%) and smokeless tobacco (39%), and the high exposure to second-hand smoke from partners (36%) and friends (48%) who smoke. Measurement of smoking status via measurement of salivary cotinine may overcome some of these potential confounders to accurate smoking status readings from the CO monitors.
Limitations
This study is a preliminary feasibility trial and, as such, includes come inherent limitations in terms of size and scope of the findings. First, there was no control condition, therefore we cannot rule out the possibility that changes in smoking behaviors were due to other factors independent of the intervention. In addition, the study design and sample size for this study carry with them certain limitations concerning the reliability with which means and mean change scores are estimated and the ability to rule out the influence of extraneous variables. The study was conducted with a small sample of HIV-positive smokers from one urban geographical area, which may limit the generalizability of the findings to other settings. Finally, NRT was only provided for 4 weeks. However, given the high nicotine dependency scores, other substance use, and depressive symptoms in the sample, longer duration of counseling, NRT, or both may have improved outcomes. Given these limitations, we emphasize that the results of this feasibility trial, while promising, should be interpreted with caution.
Conclusions
As the first study of a culturally tailored intervention for HIV-positive African American MSM smokers, this study opens a line of research that has the potential to improve our understanding of how to enhance smoking cessation outcomes in this population. Data from the pilot test provide data for the improvement of tobacco use behaviors and mood among a sample of HIV-positive African American MSM smokers. Additional research is needed to improve overall quit rates by addressing barriers to the initiation and adherence to NRT and by exploring novel approaches to relapse prevention.
Footnotes
Acknowledgments
This study was supported by the Campus and Community Health Disparities Pilot Grants Program sponsored by the Center for Health and the Social Sciences in the Department of Medicine at the University of Chicago, and the Institute for Research on Race and Public Policy at the University of Illinois at Chicago. Special appreciation is extended to the Respiratory Health Association of Metropolitan Chicago and the Howard Brown Health Center for their support of this study. We thank Karyn Haney for providing counseling, Nicole Martin, Alejandra Onate, Elizabeth Ortiz, and Kyle Jones for data collection and database management assistance, Patrick McNamara for technical and administrative assistance, and Sarah Flanagan for medical assistance. We also thank the participants for their involvement in this project.
Author Disclosure Statement
No competing financial interests exist.